Schistosomiasis
Schistosomiasis
Clinical features Schistosomiasis is a major neglected tropical disease. It is endemic in a number of tropical and subtropical regions, with an estimated 240 million people infected worldwide in more than 60 countries.1,2 There are three major anthropophilic species. Schistosoma haematobium and S. mansoni are both found extensively in Africa. S. mansoni is also found in the West Indies and in parts of South America. S. japonicum is found in China, Japan, and Southeast Asia. Two further species, S. intercalatum and S. mekongi,
may also cause disease. These trematodes (blood flukes) do not often cause major disease of the skin, but skin lesions do occur at various stages of infestation.3,4
Invasion of the human host by the aquatic cercarial stage may be associated with a dermatitis (swimmer’s itch, cercarial dermatitis).2,5,6 The rash is erythematous, pruritic, and urticarial, but eventually resolves to leave a pigmented spot. It is, however, more often associated with invasion of avian (Trichobilharzia) species.5,7,8 The cercariae of S. japonicum migrate more rapidly through the skin than those of S. haematobium or S. mansoni.9,10
The mature worms may be associated non-specifically with erythematous itching macules at the time of release of large numbers of eggs. This
974 Infectious diseases of the skin
probably represents a systemic reaction to antigen liberation. A more severe reaction seen most often with S. japonicum is Katayama disease or Yellow River fever. In addition to erythema, macules, and pruriginous lesions, patients may also have fever, malaise, chills, sweats, arthralgias, headache, lymphadenopathy, hepatosplenomegaly, diarrhea, bronchitis, pneumonitis, and peripheral blood eosinophilia.2,5,6
Specific skin lesions are seen, usually around the anus and the genitalia, most often in women. When ova are deposited, a granulomatous reaction is induced. This form of the disease is known as bilharziasis cutanea tarda (BCT). Extra-anogenital disease is very rare and seems to be more common in the trunk, particularly around the umbilicus; lesions have, however, also been described on the breast, back, scapular region, and the buttock.11–15 The lesions appear as grouped 2–4 mm solid papules, which subsequently become warty and vegetative.2,16 Occasionally, progression to squamous carcinoma supervenes. A keloidal appearance may be present. A zosteriform pattern is rarely seen, and a case with bilateral axillary involvement has been described.11,17 Periurethral granulomata due to schistosomes may be associated with thrombosis and necrosis, resulting sometimes in fistulation to the perineum (‘watering can perineum’).5 Lymphedema may be a late complication.6
Pathogenesis and histologic features Part of the life cycle of schistosomes takes place in water snails, and these release the cercariae, which penetrate the skin. They are carried to the lungs and then migrate as schistosomules to the portal vein where they mature into adult male and female worms. Adult females subsequently migrate to the mesenteric plexus (S. mansoni and S. japonicum) or vesical plexus (S. haematobium). Ova are then deposited in the venules and the clinical and pathological sequelae are a direct consequence of the immunological response to their presence.2,6
Eggs are released into the urine or feces where they hatch, releasing miracidia, which enter the snail host. Involvement of the female genital tract is usually due to S. haematobium and occurs as a consequence of worms being transported via anastomoses between the vesical and uterovaginal venous plexuses.
The pathogenesis of BCT is unknown. Several mechanisms have been proposed but none is entirely satisfactory. One mechanism proposes arteriovenous shunting of ova through a patent foramen ovale or arteriovenous fistulae in the lung. A further mechanism proposes egg-laying by the parasites locally within the affected area. This mechanism assumes the migration of adult worms to the skin through the valveless vertebral venous system.11 The mechanism of cutaneous involvement is more likely to be multifactorial.
Histologically, adult worms may occasionally be seen within the lumina of dilated deep dermal veins and lymphatics. Viable ova may be present with a recognizable miracidial structure. These are usually located within abscesses containing numerous neutrophils and variable numbers of eosinophils. Poorly formed granulomata with Langhans giant cells may also be a feature. S. haematobium is recognized by its terminal apical spine (Fig. 18.403). S. japonicum lacks a spine and in S. mansoni the spine is lateral. Dead ova typically calcify and provoke a chronic, frequently granulomatous, inflammatory response. The overlying epidermis is usually acanthotic, sometimes to the point of pseudoepitheliomatous hyperplasia, with variable transepidermal elimination of ova. It has been highlighted that in cases of extragenital BCT caused by S. haematobium, the parasite may be found in pre-existing cutaneous conditions including hidradenitis suppurativa and post-traumatic or iatrogenic scars.11
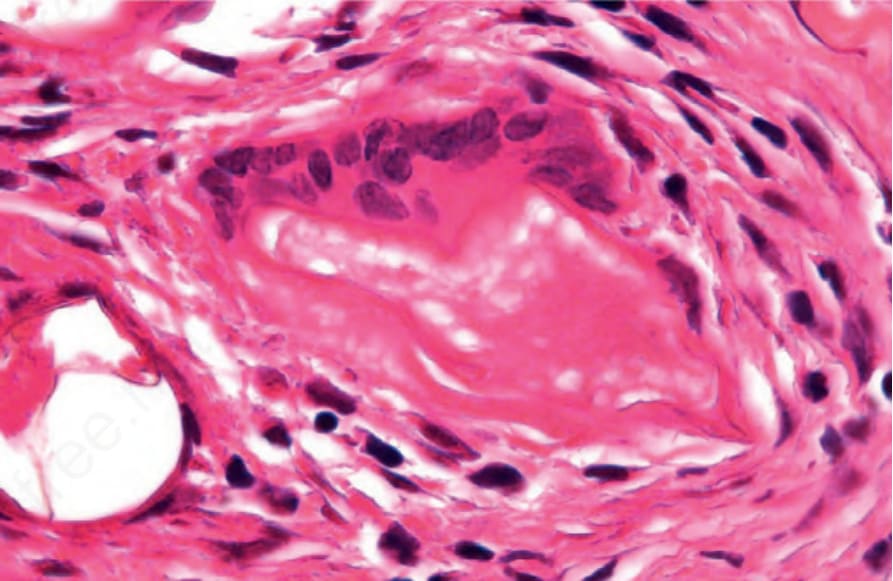
Fig. 18.403 Schistosomiasis: intradermal granuloma containing a Schistosoma haematobium egg. The characteristic terminal spine is clearly evident.