Gnathostomiasis
Gnathostomiasis
Clinical features Gnathostomiasis is a food-borne zoonotic nematode infection caused by Gnathostoma spp., including G. spinigerum, G. dolorosi, and G. nipponicum.1 Humans are accidental hosts who acquire the infection through the consumption of raw or partially cooked freshwater fish, or other intermediate hosts of the parasite such as frogs, chickens, or snakes. Fish-eating mammals in particular are the definitive host in which the adult worm resides.1,2 The latter measures 13–55 mm in length.2,3 The condition occurs in tropical and subtropical regions, including Japan, Southeast Asia, Central and South America, and Southern Africa.1,2,4,5 Gnathostomiasis should always be considered when a patient presents with the classic triad of intermittent migratory swellings, peripheral eosinophilia, and a history of travel to an endemic area.2 Humans are an unsuitable host. Consequently, the immature worm wanders through the internal viscera and subcutaneous tissues, inflicting tissue injury in the process.1
973 Schistosomiasis
The migration of excysted larvae through the gastric and intestinal walls and the liver may be heralded by fever, malaise, anorexia, upper abdominal pain, nausea, vomiting, diarrhea, and urticaria; these symptoms last for some 2 to 3 weeks.1,2 The subsequent migration of the parasite through the subcutaneous tissues results in the characteristic clinical presentation of intermittent, edematous, painful, or pruritic migratory plaques or nodules, referred to as nodular migratory panniculitis (Fig. 18.401).2,4 The presence of subcutaneous hemorrhages along the paths of larval migration is said to be pathognomonic of gnathostomiasis, and facilitates distinction from other parasitic infestations with migratory larvae, such as strongyloidiasis or sparganosis.2 The chest and abdomen are the most frequent sites of involvement, although lesions occasionally occur on the arms and hands.1 The lesions measure 5–15 cm in maximum dimension. They occur within 3 or 4 weeks of ingestion and last up to 2 or 3 weeks, only to reappear in the vicinity shortly thereafter.1–4 Although these episodes diminish in duration and intensity with the passage of time, intermittent recurrences have been known to occur for up to a decade or more in untreated individuals.2
Histologic features Although skin biopsy is the favored diagnostic modality, the large size of the infiltrated plaques and the relatively small size of the immature worm (2.5–12.5 mm in length and 0.4–1.2 mm in width) result in the organism seldom being identified in histologic sections, unless fortuitously included in the specimen.2,4 On occasion, however, the worm may be seen to emerge directly from a fresh sample shortly after completion of the biopsy procedure (F. Bravo, personal communication). A dense, eosinophil-rich inflammatory infiltrate is observed in the subcutis and dermis (Fig. 18.402). Unsurprisingly, intradermal flame figure formation reminiscent of eosinophilic cellulitis may be encountered.2,6

Fig. 18.401 Gnathostomiasis: migratory subcutaneous masses are a characteristic phenomenon. By courtesy of F. Bravo, MD, Lima, Peru.
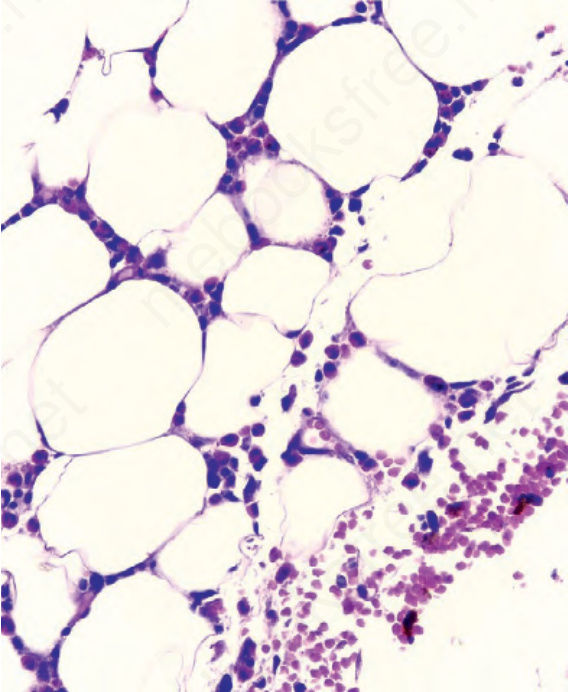
Fig. 18.402 Gnathostomiasis: the migration of an immature worm through the dermis and panniculus is invariably associated with a striking infiltrate of eosinophilic leukocytes. By courtesy of F. Bravo, MD, Lima, Peru.