Tungiasis
Tungiasis
Clinical features Tunga penetrans, the sand flea or jigger flea, causes skin lesions in Central and South American, Caribbean, sub-Saharan African, Indian, and Pakistani populations.1–4 Although increasing urbanization and improved housing has led to a decrease in the overall incidence of the disease, the condition remains highly prevalent in communities living in extreme poverty, with prevalence rates of around 80% recorded in some hyperendemic regions.4–6 Seasonal variation in the prevalence tends to occur, with a peak in the dry season.7 The disease is sometimes encountered in international travelers returning home from visits to endemic areas.2,5,8,9 Dogs, cats, and slum rats serve as animal reservoirs.4,10,11 T. penetrans is found most often in dry, warm, shady, and sandy soil.4 The gravid female flea burrows into the skin and is localized to the feet in an overwhelming majority of cases, most commonly along the edge of the plantar aspect, interdigitally, and under the nails.8,12 Involvement
968 Infectious diseases of the skin
A
of sites such as the hands, thigh, knee and inguinal area, however, has also been recorded.8,13,14 As the flea enlarges within the epidermis, a pruritic, painful white, or erythematous papulonodule develops. A black central punctum is characteristic. Pustular, wartlike, and bullous lesions have rarely been described.8,15 A remarkable case with vast numbers of bilateral lesions on the feet has been reported.16 The gravid flea, which has burrowed deep into the epithelium so that it is flush with the epidermal surface, extrudes eggs and excreta through the remaining epidermal opening. It eventually reaches a size of 1 cm in diameter. The eggs pass through the larval stages to a mature flea capable of jumping 35 cm – 350 times its own length! After laying its eggs the flea dies, the lesion collapses and is sloughed off before healing occurs. The eggs are visible on dermoscopy.17,18 Ex vivo dermoscopy has also been advocated as a useful diagnostic tool.19,20
B
The lesion causes irritation, but in itself is innocuous; however, secondary infections such as cellulitis, tetanus, and gangrene are more sinister. Autoamputation of the toes is an additional complication.21 Organisms most frequently associated with bacterial superinfection include Staphylococcus aureus and various enterobacteriaceae; secondary infection by anaerobes such as Peptostreptococcus spp. and Clostridium spp. may also occur.22,23 Although tungiasis is generally a benign, self-limiting infection in returning travelers, the condition is a source of considerable morbidity among the inhabitants of endemic areas.9
Histologic features The bulk of the flea is intraepidermal in location.20,24 It communicates with the outside through a pore in the stratum corneum via which it defecates, breathes, and lays eggs. The proboscis penetrates through the basement membrane into the dermis, which contains a mixed inflammatory infiltrate of lymphocytes, plasma cells, and eosinophils (Figs 18.387 and 18.388). The most consistently identifiable parts of the flea in skin biopsy specimens are the exoskeleton, a hypodermal layer beneath the latter, tracheae, and developing eggs; the head is rarely seen.20,24 Epidermal alterations that may be encountered include basal hyperplasia, acanthosis, hyperkeratosis, parakeratosis, and hypergranulosis. Microabscesses are also sometimes observed.20 Pseudoepitheliomatous epidermal hyperplasia has been reported.14
Dermatobia hominis, is the most common form and is endemic to parts of Central America and South America.1–4 Cordylobia anthropophaga (tumbu fly) infestation is encountered less frequently and is endemic to sub-Saharan Africa.1,2,5,6 D. hominis has a unique life cycle in that the eggs are not transmitted directly to the host by the female botfly. Instead, the eggs are attached to the abdomen of a variety of blood-sucking arthropods, usually a mosquito. The eggs hatch in the presence of body heat emanating from the warm-blooded host during a blood meal, and the larvae drop onto the skin.4
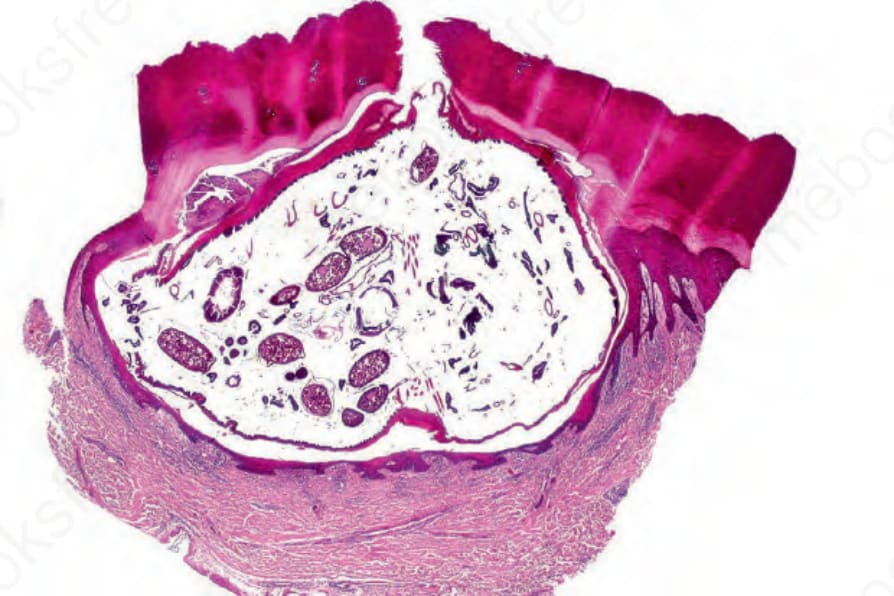
Fig. 18.387 Tungiasis: the flea is surrounded by epidermis except for an ostium in the stratum corneum through which it defecates and lays eggs. Similarly, its head penetrates into the dermis to feed from the superficial blood vessels.
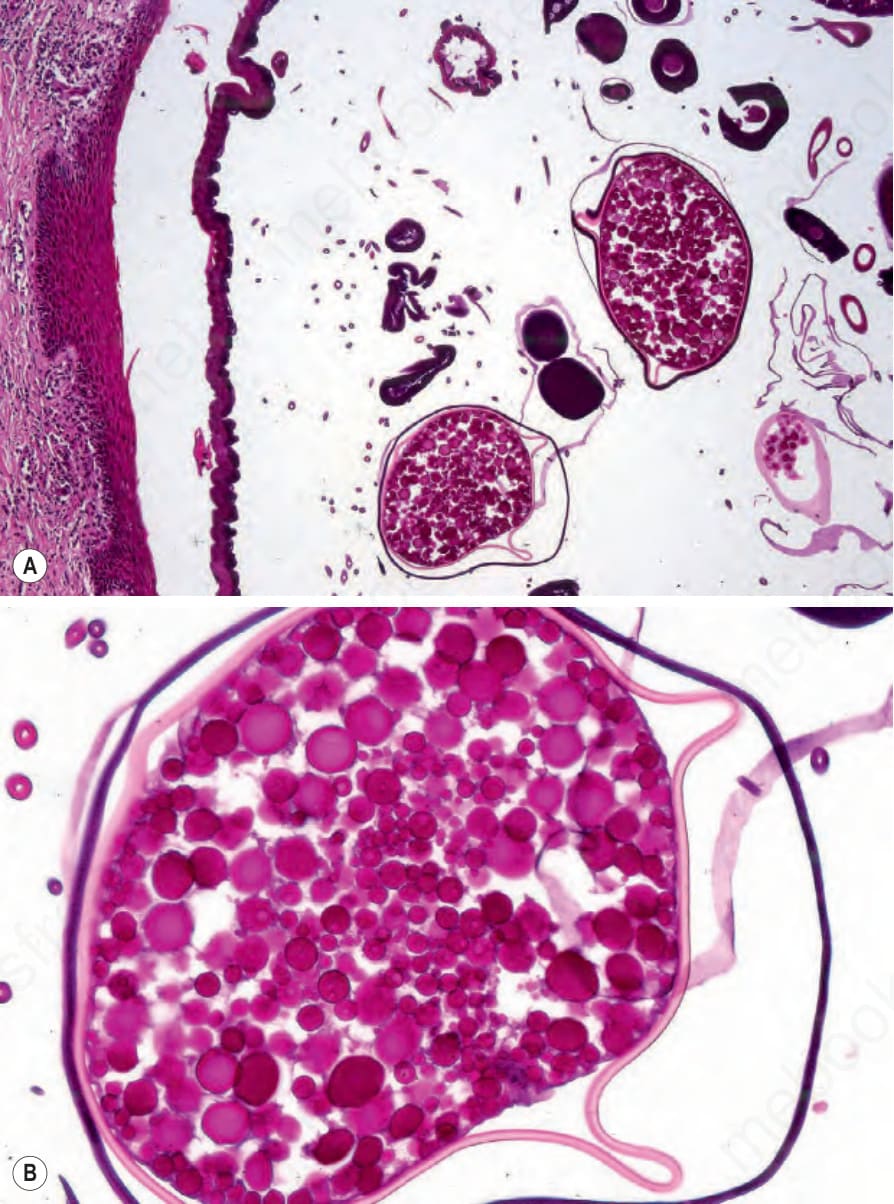
Fig. 18.388 (A, B) Tungiasis: numerous eggs are evident.