Scabies
Scabies
Clinical features Scabies is caused by the itch mite Sarcoptes scabiei (S. scabiei var. hominis), which penetrates the skin in many areas, but usually below the neck.1–5 An estimated 300 million people are affected worldwide.3,6–8 The most commonly affected sites are about the hands and feet (Fig. 18.382). Papules and burrows are often found between the fingers or along the sides of the fingers. The soles and sides of the feet are especially affected in children. As a secondary phenomenon (unrelated to burrows), patients develop an intensely pruritic papular generalized eruption, particularly affecting the abdomen, thighs, and buttocks. This reaction may be immune complex-mediated or develop as a consequence of a cell-mediated immune reaction. Patients may have raised serum IgE levels.9 Antigenic cross-reactivity with house dust allergens has been demonstrated.6 The papular eruption is often excoriated and may be associated with secondary bacterial infection (Fig. 18.383), which may in turn lead to complications such as septicemia, rheumatic fever, and postinfectious glomerulonephritis.2,10–12 This contagious infection is spread through close personal contact and may be transmitted sexually, resulting in genital scabies.1 Scabies may be masked by the use of corticosteroids (scabies incognito).6 Furthermore, the disease can mimic a variety of other dermatological disorders, resulting in delayed diagnosis.10,13,14
The pathogenetic roles of mite serine protease inhibitors of the serpin superfamily and mite aspartic protease have been highlighted recently.20–23
The fertilized female S. scabiei mite deposits eggs in the burrows in the epidermis. The larvae emerge in 3–5 days and mature in 10–14 days. The burrows extend at a shallow angle through the stratum corneum and may reach the deeper epidermis. There is acanthosis and hyperkeratosis and
The uncomplicated lesion is a sinuous burrow up to 1 cm in length and associated with intense itching, particularly at night. A small proportion of patients may go on to develop nodular scabies, which is seen particularly in the axillae, about the genitalia, and on the abdomen.9 These are intensely pruritic and remarkably persistent. Severe keratotic and psoriasiform lesions are seen in physically and mentally debilitated and immunocompromised (including HIV-positive and some iatrogenically immunosuppressed) patients owing to massive infestation and is termed hyperkeratotic, crusted, or Norwegian scabies (Fig. 18.384).15–18 Crusted scabies is a potential cutaneous manifestation of IRIS in patients with HIV/AIDS who have received ART.19
Pathogenesis and histologic features Scabies is associated with poor socioeconomic conditions, overcrowding, and poor personal hygiene, and may be acquired during sexual contact.3,8
967 Tungiasis
A
B
In nodular skin lesions, the dermal infiltrate may be very dense and, in addition to histiocytes, plasma cells, eosinophils, and lymphocytes, atypical and hyperchromatic cells may be evident, which may suggest a lymphomatous process if the clinical information is not evident.38 Hyperplasia of Langerhans cells has been reported; this may potentially be misdiagnosed as Langerhans cell histiocytosis.39–41
The papular lesions show mild hyperkeratosis and parakeratosis in association with acanthosis and spongiosis. A perivascular inflammatory cell infiltrate of lymphocytes, histiocytes, and sometimes neutrophils may be evident in the superficial dermis. Eosinophils may be absent.9 Rarely, scabies incognito may present with a subcorneal pustular reaction mimicking subcorneal pustular dermatosis.42
often associated spongiosis with a lymphocytic infiltrate in the epidermis (Fig. 18.385). The spongiosis may progress to vesiculation. Eggs, larvae, mites, mite parts, and excreta (scybala) may be identified in the stratum corneum.10,24–27 Eosinophilic spongiosis may be encountered.28 In the dermis, there is a superficial perivascular (and sometimes diffuse) infiltrate of lymphocytes and histiocytes, sometimes accompanied by polymorphs and less often eosinophils. The presence of the last may be associated with the features of acute vasculitis and flame figures.29 The lymphocytes are predominantly of T-cell lineage and may exhibit atypia.27,30 CD30 positive lymphocytes may be a feature. Fibrin thrombi are often encountered in the superficial dermal vessels.27
In the hyperkeratotic variant, mites and eggs are numerous, but they are scanty in the other forms. In such cases, PCR may be a useful adjunct to the diagnosis.43 Examination of sections under polarized light, however, provides a more affordable and practical alternative in subtle cases, as elements of the scabetic mites such as the spines and scybala are polarizable.44 The identification of curved, pink, often refractile structures (remnants of eggshell casings) within the intracorneal burrows (the ‘pigtail’ sign) is a useful diagnostic clue in those cases where the body of the mite is not visible in the plane of sectioning (Fig. 18.386).27,45,46 A further very useful clue is identification of the feces of the mites within the stratum corneum, displayed as bright yellow amorphous aggregates (‘golden nuggets’).
C3 and Ig may be detected at the epidermo-dermal junction and within the perivascular region, adding support to the concept of an immune complex-mediated pathogenesis.30 IgE has been detected in vessel walls and IgA and C3 in the stratum corneum.31 There have also been numerous reports of eruptions resembling BP in association with proven scabies.32–34 In one study, these patients were found to have circulating antibodies against BP180 and/or BP230 antigens, indicating that at least a proportion of bullous eruptions in scabetic patients are indeed attributable to BP.33 Others, however, have documented negative direct and indirect immunofluorescence in patients with bullous scabies whose lesions mimicked BP both clinically and histologically.35 One recent study nevertheless revealed that elderly patients with a history of scabies were at significantly increased risk for developing BP.36
There have been rare reports of Grover disease in association with Sarcoptes scabiei infestation.37

Fig. 18.382 Scabies: the burrows are linear, slightly raised lesions. The most common sites affected include the lateral aspects of the fingers, the web between thumb and first finger, and the wrists. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 18.383 Scabies: this is an intensely itchy condition and therefore secondary infection is a not uncommon complication, as for example in this child with staphylococcal sepsis. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

Fig. 18.384 Norwegian scabies: this example (also known as the hyperkeratotic variant) may affect widespread areas of the body, and is associated with severe crusting and a very heavy infestation of mites. It is exceedingly infectious. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
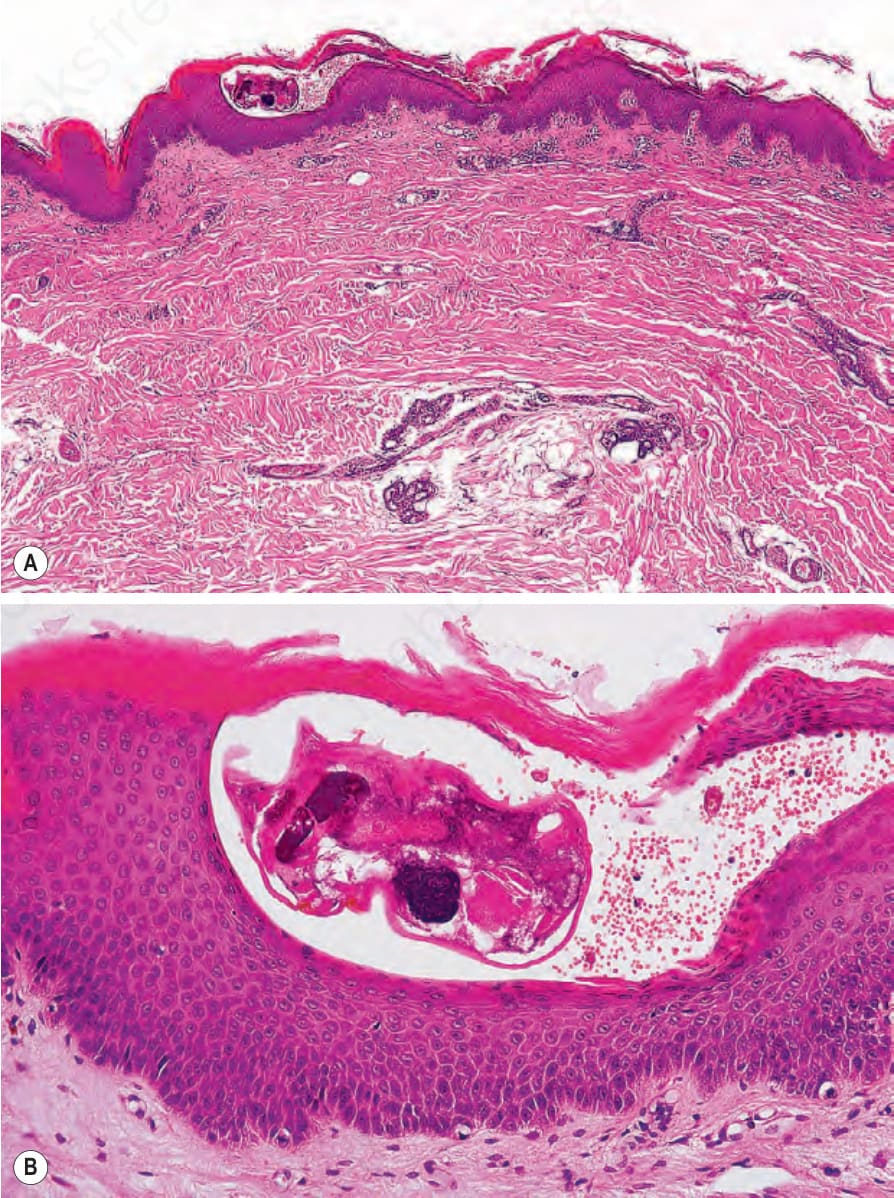
Fig. 18.385 (A, B) Scabies: the mite is located at the junction between the epidermis and the stratum corneum.
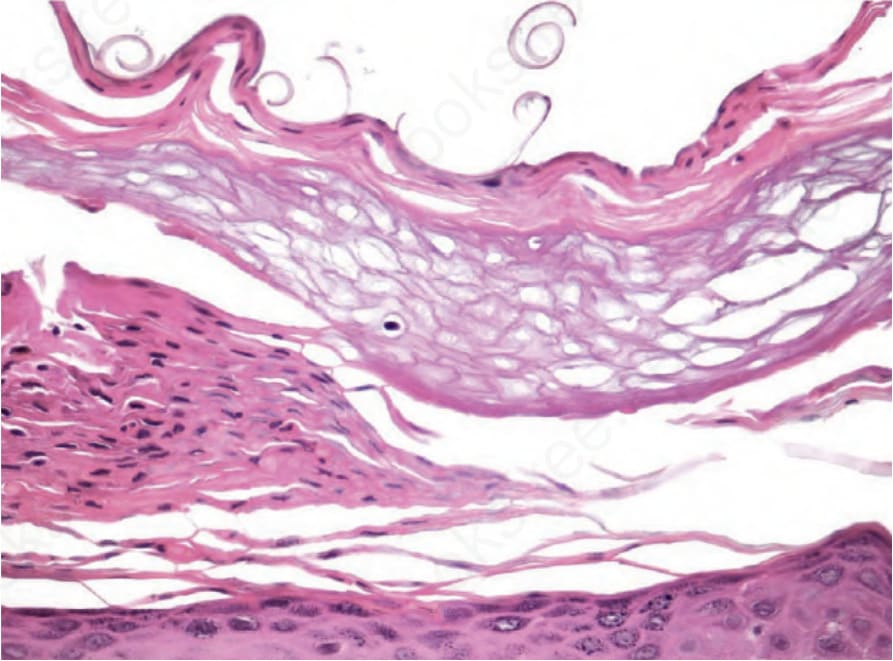
Fig. 18.386 Scabies: small, curved eosinophilic structures are attached to the stratum corneum, and represent fragments of Sarcoptes egg shell casings. This has descriptively been referred to as the ‘pigtail’ sign.