Condyloma acuminatum
Condyloma acuminatum
Clinical features A majority of sexually active individuals will have detectable HPV infection at least once during their lifetime. An estimated 14 million people are infected annually with genital HPVs.1 A recent systematic review of the literature concerning anogenital warts revealed a median incidence of 137 and 120.5 per 100 000 among males and females, respectively.2
except in association with HIV infection. They may regress spontaneously after a few weeks or months, or may persist for years. Signs of regression include pruritus, an erythematous, edematous appearance, depigmented haloes, and an eruption of multiple tiny plane warts.2,6,7 Cell-mediated immunity plays a key role in the spontaneous regression of plane warts in immunocompetent individuals.8 Multiple plane warts may evolve as a cutaneous manifestation of immune reconstitution inflammatory syndrome (IRIS) in HIV-infected patients receiving highly active ART.9 Exacerbation of lesions has been reported following facial laser resurfacing.10
Condylomata acuminata are particularly caused by HPV types 2, 6, 11, 16, 18, 30–33, 35, 39, 41–45, 51–56, and 59 and develop as a consequence of the trauma accompanying sexual intercourse.3–15 More frequent transmission has been reported from females to males than from males to females.1 HPV6 and 11 alone account for more than 90% of these lesions, with HPV6 present in about two-thirds of cases and the remaining one-third caused by HPV11.6,7 The incubation period is variable (usually between 2 and 3 months).16 Condylomata acuminata occur on the glans penis and prepuce or shaft as soft, fleshy, sometimes filiform plaques and may extend into the meatus (Figs 18.19 and 18.20). On the shaft, they are less exophytic. Vulval lesions may be bulky and macerated, and may extend into the introitus (Fig. 18.21). Similar fleshy and filiform soft masses occur perianally, more often in males (Fig. 18.22).17 Anal squamous carcinoma has also been shown to contain HPV6, 16, and 18 in a significant proportion of cases (Fig. 18.23).8 The rate of local recurrence is about 30%.18 The lesions are uncommon in children (where they may be a sign of sexual abuse) and are seen most often in young adults (second and third decades), frequently in association with other genital infections.6,11,19 Childhood condylomata regress spontaneously in more than 50% of cases.20 Genital warts are common among HIV-infected individuals.21
Histologic features Plane warts are acanthotic and show orthokeratosis with an open pattern reminiscent of ‘chicken wire’ (‘basket weave’ hyperkeratosis). Parakeratosis is not a feature and there is little papillary configuration to the acanthosis (Fig. 18.18). Keratinocytes of the upper part of the stratum spinosum show striking cytoplasmic vacuolation with margination of the keratohyalin granules and tonofilaments.4 Regression is characterized by keratinocyte necrosis (apoptosis), individual cell keratinization, parakeratosis, lymphocytic exocytosis with spongiosis, and a superficial perivascular chronic inflammatory
It is important to note that a significant proportion of genital HPV infections are asymptomatic.5,22 The female partners of male patients with condyloma acuminata have been shown to have an increased risk of cervical HPV infection and intraepithelial neoplasia (squamous intraepithelial lesion/ cervical intraepithelial neoplasia [SIL/CIN]).23 Cervical neoplasia associated with pre-existent condylomata acuminata has also been related to a background of immunosuppression, at least in some patients.24 The worldwide HPV prevalence in cervical carcinomas is reported to be 99.7%.25 HPV16, 18, 31–33, 35, 39, 42, and 51–54 are most commonly associated with cancers of the cervix, vulva, and penis.9–11,26–28 Patients with condylomata
833 Condyloma acuminatum
acuminata are at increased risk for developing not only carcinomas of the vulva, vagina, penis, and anus, but also certain nonanogenital squamous cell carcinomas.29 Routine vaccination with a quadrivalent vaccine against HPV types 6, 11, 16, and 18 has led to a significant reduction in the burden of vulval and cervical carcinomas, genital warts, and anogenital intraepithelial neoplasia.17,30–32
A large, exuberant, and locally destructive variant of condyloma (Buschke-Löwenstein tumor) may rarely be encountered (Fig. 18.24).33–36 This is associated with HPV types 6, 11, or 16. It is likely that this giant variant represents a variant of verrucous carcinoma but the issue has been controversial (see Chapter 22).33–39 Juvenile laryngeal papillomas containing HPV6 and 11 can be seen in children born to mothers with condylomata acuminata.5 They may show malignant progression if irradiated.
Malignant transformation of condyloma acuminatum is uncommon, but it is seen more often than in other lesions associated with HPV except for EV.
834 Infectious diseases of the skin
A
B
Histologic features Condylomata acuminata are characterized by marked acanthosis with a solid or trabecular pattern and a broad rounded exophytic growth (Fig. 18.25). There is a sharp, fairly regular, deep margin. The surface of the lesion is hyperkeratotic and parakeratotic. Superficial vacuolated keratinocytes (koilocytes) are characteristic (Fig. 18.26) and coarse keratohyaline granules may be present. The vacuolated epithelium is often most marked in the declivities. Condylomata that are treated with podophyllin prior to removal demonstrate marked epidermal pallor and increased mitoses and necrotic keratinocytes in the lower half of the epidermis.40 These changes may lead to a misdiagnosis of malignancy. Giant condyloma acuminatum (anogenital verrucous carcinoma, Buschke-Löwenstein tumor) occurs most frequently on the genitalia, and is larger and more cauliflower-like.33–36 It shows some tendency to endophytic growth, but without any suggestion of frank infiltration. It can recur locally, but metastasizes very rarely. Most experts regard this lesion as a variant of verrucous carcinoma. Anal condylomata may develop bowenoid features, and occasionally invasive tumor supervenes.8–10

Fig. 18.17 Plane wart: note the typical flat, flesh-colored papules, which have extended in a linear distribution due to scratching (Koebner phenomenon). By courtesy of B Al-Mahmoud, MD, Qatar, Oman.
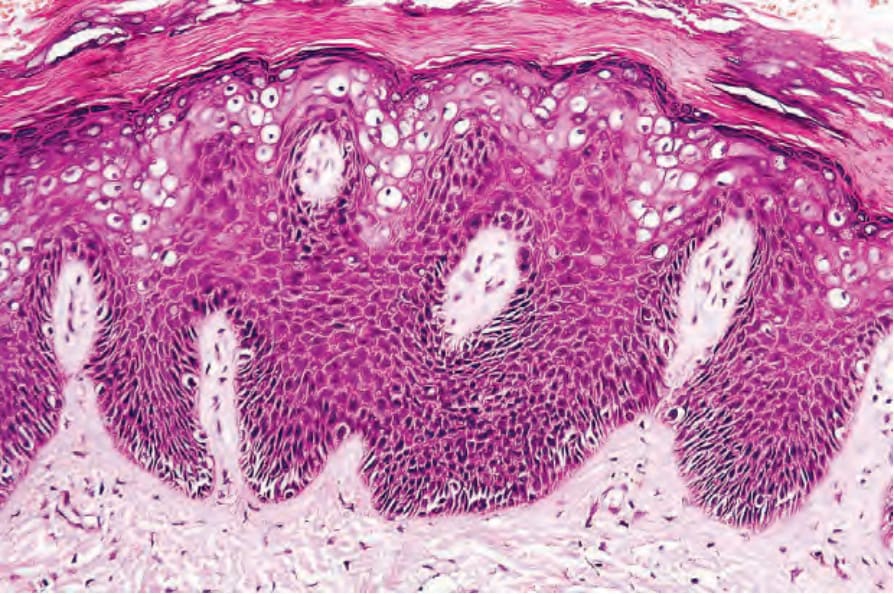
Fig. 18.18 Plane wart: there is hyperkeratosis and slight regular acanthosis; papillomatosis is only mild. Note the prominent cytoplasmic vacuolation.

Fig. 18.19 Condyloma acuminatum: note the typical filiform appearance. By courtesy of the Department of Genitourinary Medicine, St Thomas’ Hospital, London, UK.

Fig. 18.20 Condyloma acuminatum: there are multiple lesions on the shaft of the penis and scrotum. By courtesy of the Department of Genitourinary Medicine, St Thomas’ Hospital, London, UK.

Fig. 18.21 Condyloma acuminatum: in this patient, there is very widespread involvement of the vulva and perineum. This patient is likely to have cervical HPV infection. By courtesy of R.A. Marsden, MD, St George’s Hospital London, UK.

Fig. 18.22 Condyloma acuminatum: there is very extensive involvement of the perineum. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
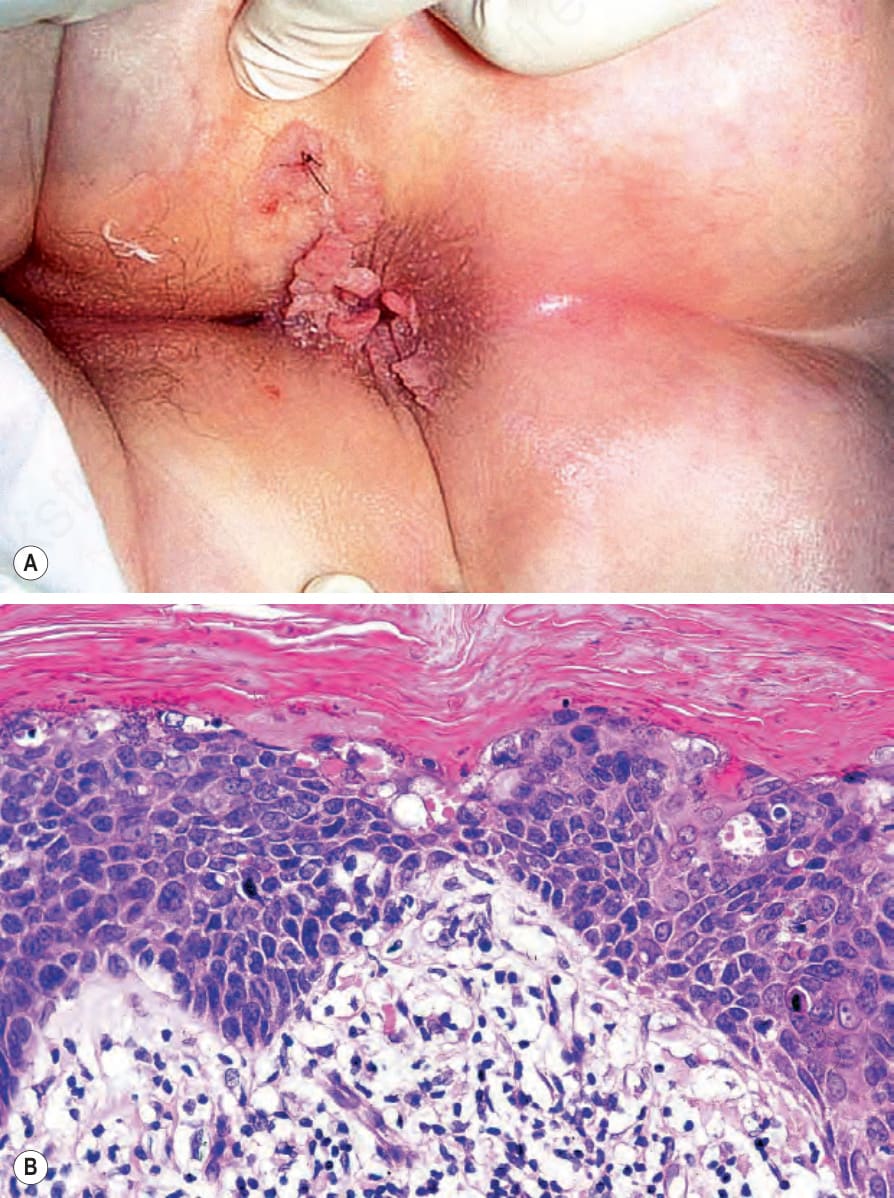
Fig. 18.23 (A, B) Condyloma acuminatum: in addition to multiple condylomata, there was histologic evidence of in situ squamous cell carcinoma. By courtesy of P. Ngheim, MD, Dana Farber Cancer Institute and Harvard Medical School, Boston, USA.

Fig. 18.24 Buschke-Löwenstein tumor: there is massive infiltration of the buttocks and perineum with numerous sinuses. HPV type 6 was identified by DNA in situ hybridization and Southern blot analysis. By courtesy of A. Grassegger, MD, University of Innsbruk, Austria.
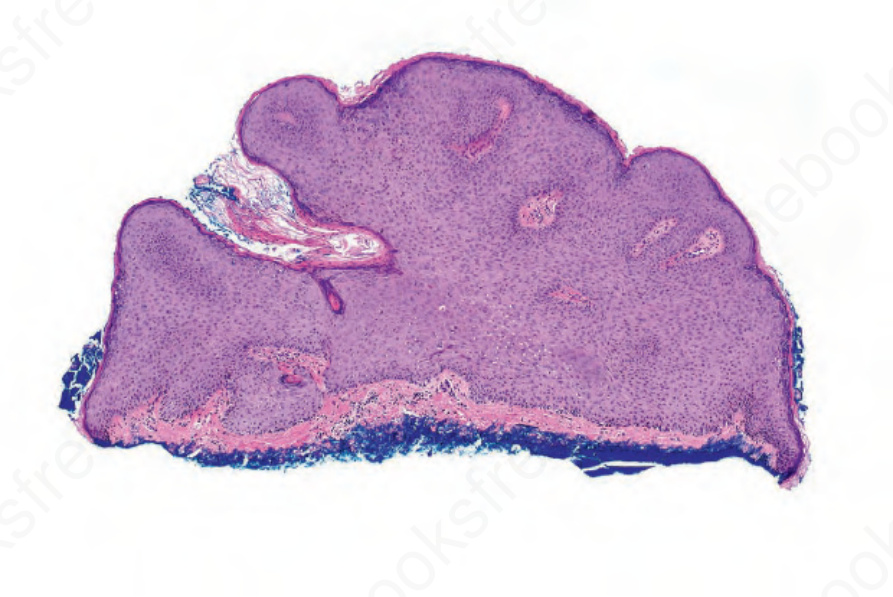
Fig. 18.25 Condyloma acuminatum: note the keratotic acanthotic epidermis with rounded lateral borders. Koilocytes are present in the declivities of the papillomatous epithelium.
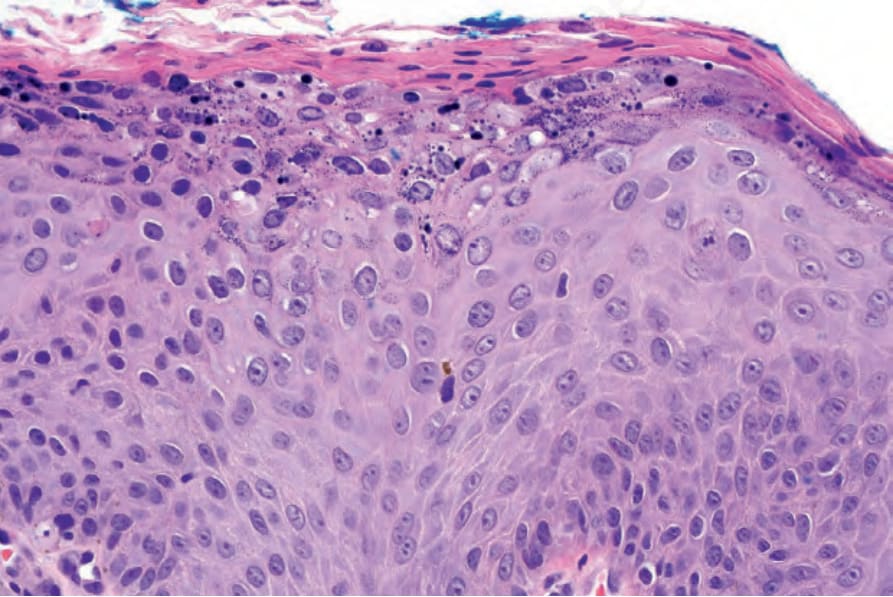
Fig. 18.26 Condyloma acuminatum: note the parakeratosis and vacuolation of the superficial keratinocytes.