Common wart
Common wart
The common wart (verruca vulgaris) is caused by infection with human papillomavirus (HPV) (Fig. 18.1). HPV is a DNA virus of the papovavirus family. The number of known HPV genotypes currently stands at more than 200, classified according to the extent of their DNA homology (DNA hybridization) (Table 18.1).1–5 In order for an HPV type to be regarded as ‘new’, sequences in selected genomic regions must exhibit more than 10% divergence compared to any of the known HPV types.2 Monoclonal antibodies to intact viruses have been produced and can demonstrate individual types of HPV; antibodies to viral components are only group specific (Fig. 18.2). Advances in molecular pathology have resulted in improved and more specific methods of HPV detection and classification, including in situ polymerase chain reaction (PCR), nonisotopic in situ hybridization (NISH), rolling circle amplification and next-generation sequencing.5,6 Five genera exist, namely, α, β, γ, µ, and ν. The α HPV types are predominantly mucosotropic, and are often classified as low-risk (e.g., HPV6, HPV11) or high-risk (e.g., HPV16, HPV18) based on their association with the development of cancer, including cervical and anogenital neoplasms and some carcinomas of the oral cavity.7–10 Although the other four genera are associated with cutaneous infection, it is the β HPV types that are of particular
827 Common wart
relevance in the etiopathogenesis of nonmelanoma skin cancer in the setting of epidermodysplasia verruciformis (EV).4,7,8,11,12
Papillomaviruses, which are small and nonenveloped and show icosahedral symmetry, contain circular double-stranded DNA composed of approximately 8000 base pairs. The viral particle, which has a diameter
HPV type Associated clinical lesions
1 Deep plantar warts, common warts
2 Common warts, flat warts
3 Flat warts
4 Common warts, plantar warts
5 Epidermodysplasia verruciformis (EV)
6 Genital warts, laryngeal papilloma
7 Butcher warts
8 EV
9 EV, keratoacanthoma
10 Flat warts
11 Laryngeal papillomas, genital warts
12 EV
13 Focal epithelial hyperplasia
14, 15 EV
16 Genital warts, bowenoid papulosis, cervical dysplasia, cervical carcinoma, digital, squamous cell carcinoma, nongenital Bowen disease
17 EV
18 Genital warts, bowenoid papulosis, cervical dysplasia, cervical carcinoma
A
19–25 EV, keratoacanthoma
26–29 Common warts, flat warts
30 Laryngeal carcinoma, genital warts
31–32 Genital warts, bowenoid papulosis, cervical dysplasia, cervical carcinoma
33 Cervical carcinoma
34 Bowenoid papulosis, Bowen disease
35 Cervical dysplasia, cervical carcinoma
36 EV
37 EV, keratoacanthoma
38 EV
B
39 Bowenoid papulosis, cervical carcinoma
41 Flat warts
42 Genital warts, bowenoid papulosis, cervical dysplasia, cervical carcinoma
43, 44 Genital warts, laryngeal papillomas
46, 47 EV
48 Bowenoid papulosis, Bowen disease
49, 50 EV
51–54 Genital warts, bowenoid papulosis, cervical dysplasia, cervical carcinoma
55 Genital warts, laryngeal papillomas
Reproduced with permission from Melton, J.L. and Rasmussen, J.E. (1991) Dermatologic Clinics, 9, 219–233.
828 Infectious diseases of the skin
of approximately 55 nm, contains 72 capsomeres.2,13 The HPV genome is divided into three functional regions: a late region, an early region, and a noncoding 1000 base pair upstream regulatory region (URR). The URR is located immediately upstream of the E6 open reading frame (ORF) and contains sequences regulating expression of all ORFs, including promoter elements and transcriptional enhancer sequences. In excess of 20 messenger RNAs are expressed, usually in a differentiation-specific and cell-specific manner.2 Genes in the early region (E1, E2, E4, E5, E6, E7) are responsible for transcription, replication, and cellular transformation.4 The E4 ORF is highly expressed in differentiated HPV-infected epithelial cells. Some forms of E4 encode a protein capable of disrupting the cytokeratin network, resulting in the phenomenon of koilocytosis.2 The E4 ORF represents a region of maximal divergence between different HPV types.14 Each viral genotype is most often detected in lesions at specific anatomical sites or shows distinct histologic characteristics.15–17
HPV infection in man results in a variety of cutaneous lesions including verruca vulgaris, filiform warts, verruca plana, plantar warts, anogenital warts, and bowenoid papulosis.13 Mucosal lesions include oral warts and condylomata, focal epithelial hyperplasia or Heck disease, nasal and conjunctival papillomas, laryngeal papillomatosis, and cervical lesions.2,13 HPV infection may be asymptomatic or result in a carrier status. One study showed that cutaneous HPV infections commonly persist on healthy skin over several years, and that persistence does not appear to be associated with age, sex, a history of warts, immunosuppressive therapy, or HPV type.18
Clinical features Common warts are caused by HPV types 1, 2, 4, 7, and 26–29.13 In immunosuppressed patients, HPV subtypes 75, 76, and 77 may be pathogenetic.19 A case with extensive, recalcitrant verrucae linked to infection with HPV type 57 has been reported.20 Rarely, HPV subtypes associated with genital warts such as 6 and 11 have been found in common warts in children.21 HPV16, a common genital HPV type with oncogenic potential, was detected in 6.6% of lesions in a series of 45 immunocompetent patients with nongenital cutaneous warts.22 Conversely, verrucae vulgaris may sometimes occur on the vulva. HPV type 2 has been detected in such cases. It is important to note that these ‘nonvenereal’ genital lesions may occur in girls less than 5 years of age, as an erroneous clinical or histologic diagnosis of condylomata acuminata could lead to allegations of sexual abuse.23
Warts are very common lesions, particularly in children.24 Adults are also frequently affected. In a survey of 2180 adults, 3.5% had warts.25 Butchers and slaughterhouse workers have an increased risk.26,27 Common warts may occur anywhere on the skin and in people of any age, but are most common on the backs of the hands and the fingers and on the knees of young children, where they appear as firm keratotic papules 1–10 mm across (Fig.
18.3).24 Koebnerization is common (hence, kissing lesions on fingers).13 In other sites they may appear more filiform and less firm (Fig. 18.4). The latter are particularly seen on the lips, nostrils, and eyelids.1 Giant periungual lesions have been described.28 Warts may also present as a cutaneous horn. They persist for a few months up to several years and often regress spontaneously, particularly in children.
Chronically immunosuppressed patients (e.g., following renal transplantation) often have a large number of warts (Fig. 18.5).29,30 Chronicity is associated with increasing numbers of lesions. EV-like lesions due to HPV5 have also been described in human immunodeficiency virus (HIV)-positive patients and following renal transplantation.31 Numerous warts may be seen in other immunosuppressed patients (e.g., with non-Hodgkin lymphoma, leukemia, Hodgkin lymphoma, and HIV infection).13,31–34 In patients with
829 Plantar warts
A
acquired immunodeficiency syndrome (AIDS), warts may regress following antiretroviral therapy (ART).35
Pathogenesis and histologic features In the skin, it is the inter-appendageal epidermis and the stem cells of the bulge region of the hair follicle that are the apparent targets of the virions.7 In situ hybridization studies of HPV lesions have shown that viral DNA synthesis in the epidermis occurs in the superficial prickle cell layer, and full virus assembly with capsid production occurs in the granular cell layer.13 HPV DNA has been demonstrated in apparently normal skin up to 15 mm from a virus-associated lesion.36 The requirement for growth in very well-differentiated epithelia may explain the difficulty of culturing HPV and why host destruction of the lesions may be protracted. Immune mechanisms are presumed to be less effective against organisms or altered cells that are situated superficially with no direct blood supply.
B
Regression of HPV lesions is usually spontaneous but may not occur for several years.37 Cell-mediated immunity seems to be important in effecting the regression since lymphocytes are seen infiltrating the wart epithelium at this stage. Other features of regression include liquefactive basal cell degeneration, epidermal degeneration, and vascular thrombosis.37,38 Toll-like receptors (TLRs) have been identified as important role players in viral recognition and the initiation of an antiviral host immune response. TLR3, TLR9, interferon-beta (IFN-β), and tumor necrosis factor-alpha (TNF-α) appear to play an important role in the skin’s innate immune response to HPV infection.39 Langerhans cells and Langerhans-like dendritic cells may exert direct antiviral activity. This is facilitated via the expression of TLRs such as TLR3, which may in turn trigger the release of IFN-inducible chemokines, including CXCL9, a monokine induced by IFN-γ.40
in the uninvolved epidermis. There is a prominent granular cell layer within which are enlarged clumps of irregular basophilic keratohyalin (Fig. 18.7).1 These are seen best in the concavities between the papillomatotic epithelial papillae. Large cells with prominent vacuolated cytoplasm and a small pyknotic nucleus are seen in the upper layers of the epidermis (koilocytes) (Fig. 18.8). Koilocytes are, however, more frequently observed in genital warts (see below). Connective tissue and tortuous small blood vessels may invade the filiform projections (Fig. 18.9). In some cases, involvement of the superficial portion of the hair follicles by HPV results in focal changes identical to a trichilemmoma or an inverted follicular keratosis.41 However, not all of these lesions are induced by HPV as has been suggested.42
Following regression of the wart(s), an individual is usually immune to further HPV infection. Patients with a deficiency in cell-mediated immunity – whether primary or acquired, iatrogenic or virally induced (HIV/AIDS) – are particularly susceptible to the development of warts, which tend not to involute spontaneously and can be a particularly refractory therapeutic problem.
Transmission of HPV is by inoculation of infected desquamated cells through close contact at points of minor trauma; hence, common warts are seen most often on the hands. Periungual warts are particularly associated with nail biting and plantar warts are especially related to prolonged immersion in water.25
Common warts show filiform acanthosis with vertical tiers of parakeratosis over the tips of the exophytic component (Fig. 18.6). There is also marked orthokeratosis. A downward extension of the acanthosis produces a curvilinear deep margin and curved distortion of the adjacent rete ridges
Ordinary common warts are only exceptionally associated with in situ or invasive squamous cell carcinoma.43,44 HPV16 has been associated with periungual Bowen disease and squamous carcinoma.45–47 The role of HPV in cutaneous neoplasia is discussed further in Chapter 22. Molecular studies have implicated cutaneous HPV infection as a carcinogenic cofactor in association with solar ultraviolet radiation in the evolution of nonmelanoma skin cancer.11,48

Fig. 18.1 Viral warts: (A) these are exceedingly common and may affect any site; (B) lesions are frequently multiple. (A) By courtesy of the Institute of Dermatology, London, UK; (B) By courtesy of J.C. Pascual, MD, Alicante, Spain.
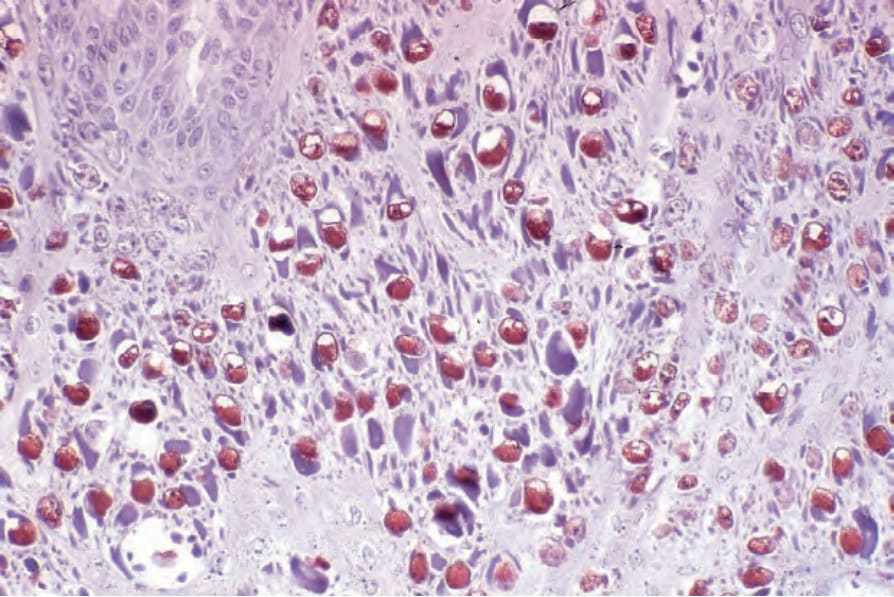
Fig. 18.2 Verruca vulgaris: note the positive labeling of the nuclei in this section stained with a peroxidase-labeled antiserum to papilloma virus.

Fig. 18.3 Verruca vulgaris: verrucae are most commonly seen on the hands and fingers. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 18.4 Filiform wart: this variant occurs most often on the face and around the axillae. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 18.5 Verruca vulgaris: presentation with such large numbers of lesions raises the possibility of immunosuppression. By courtesy of the Institute of Dermatology, London, UK.

Fig. 18.6 Verruca vulgaris: (A) note the hyperkeratosis and papillomatosis; (B) there is often marked parakeratosis typically arranged as a vertical tier. Koilocytes are conspicuous.
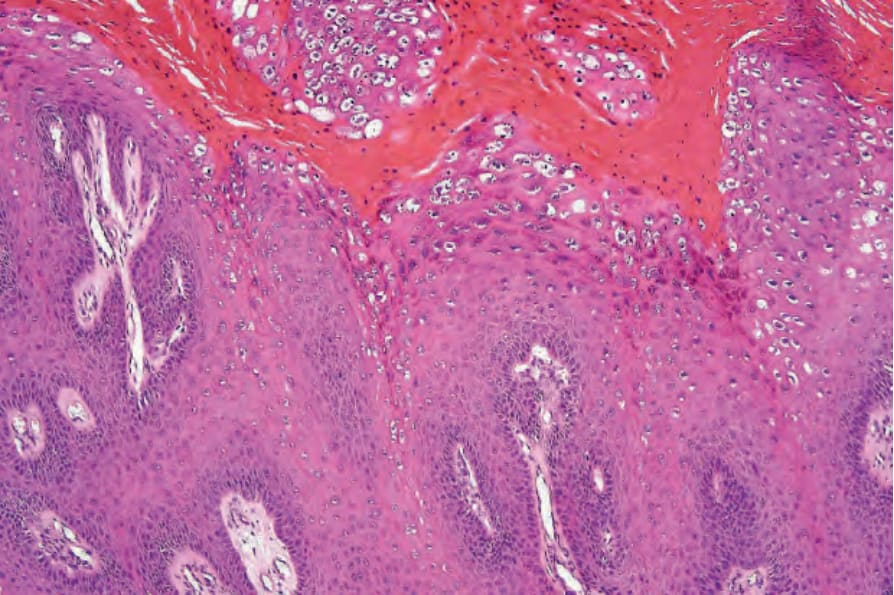
Fig. 18.7 Verruca vulgaris: large vacuolated cells with enlarged and irregular keratohyalin granules are characteristic.
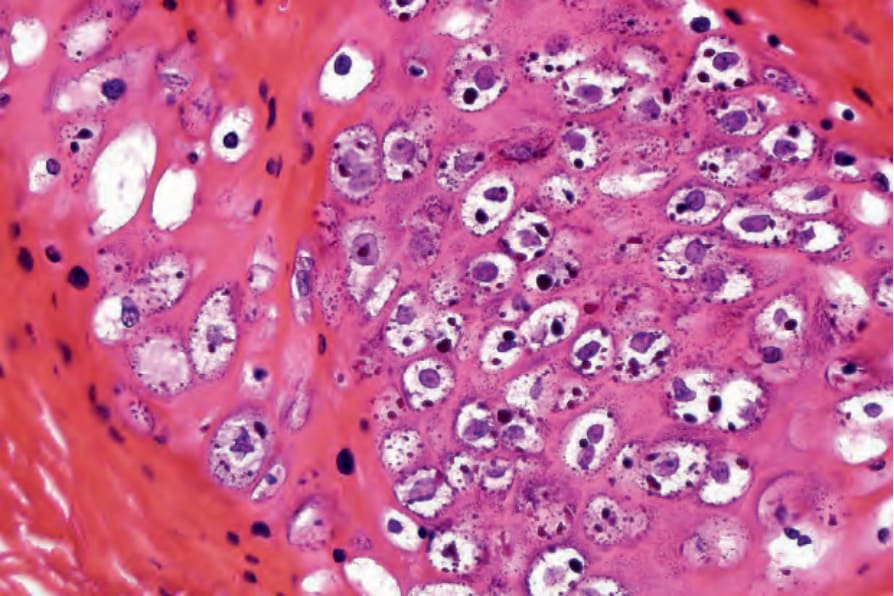
Fig. 18.8 Verruca vulgaris: high-power view of koilocytes.
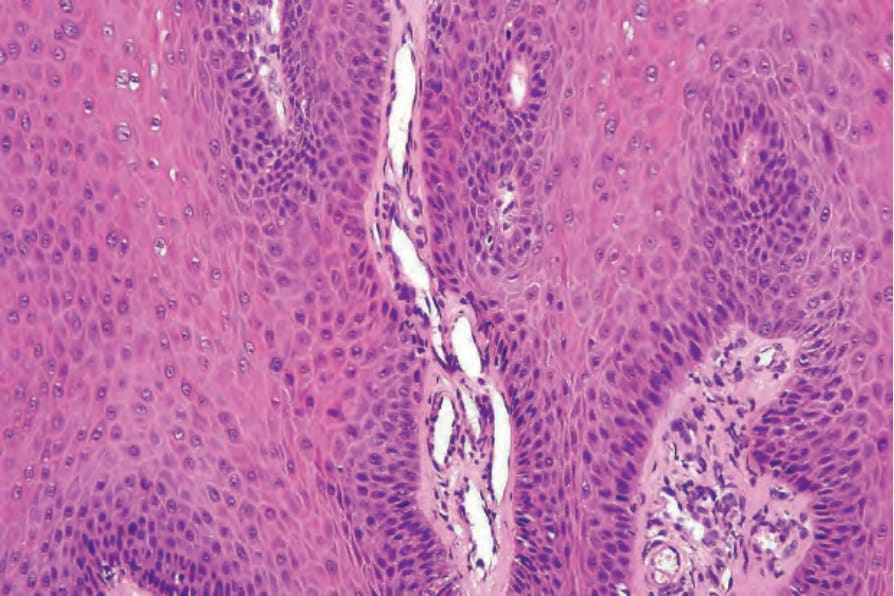
Fig. 18.9 Verruca vulgaris: the core of the papillary projection contains conspicuous dilated capillary loops.
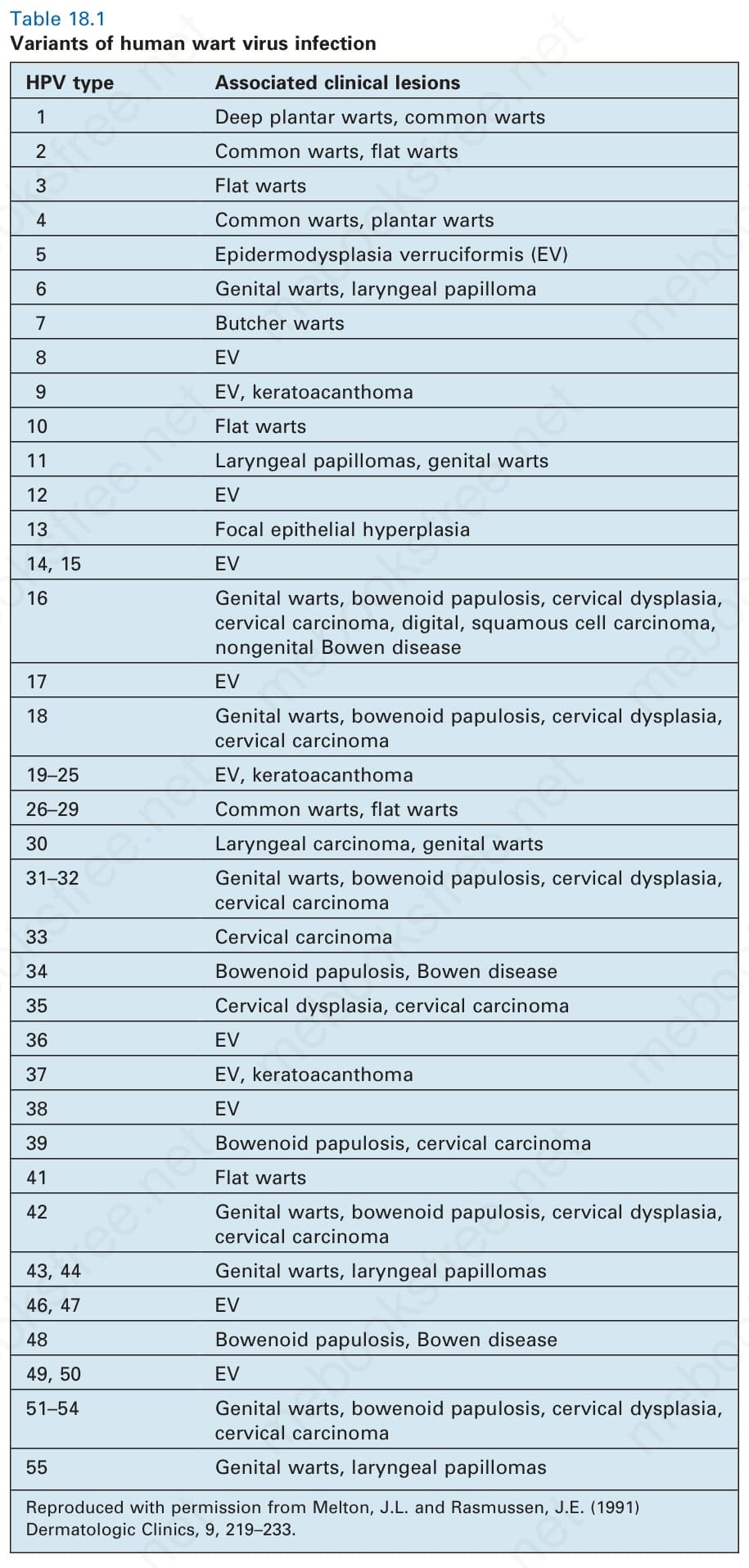
Table 18.1 Variants of human wart virus infection