Factor V (Leiden) mutation
Factor V (Leiden) mutation
Clinical features Mutation of factor V Leiden is the most common inherited condition predisposing to thrombosis.1 The mutation is associated with a prothrombotic state caused by factor V resistance to inactivation by protein C. It can be identified by PCR.
ITP has rarely been associated with vaccinations in children.15–16
The chronic form shows a predilection for women, and presents with a tendency to bruise easily following mild trauma and bleeding (Fig. 16.130). In severely affected patients, lesions develop in the mucous membranes of the respiratory, genitourinary, and gastrointestinal systems in addition to the integument.
Laboratory examination reveals thrombocytopenia and a prolonged bleeding time. Partial thromboplastin time and prothrombin time are not affected.
Pathogenesis and histologic features Immune thrombocytopenic purpura is an autoimmune disease caused by IgG antiplatelet antibodies, which lead to destruction of platelets.17–20 There is also a disruption of cellular immunity with a shift toward a type 1 and Th17 immune response.20 A cytotoxic T-cell-mediated process has also been implicated in platelet destruction.21 Molecular mimicry between HIV glycoproteins (GP120/160) and membrane antigens (i.e., glycoprotein GPIIb/ IIIa) on platelets may play a role in the development of thrombocytopenia in occasional HIV-infected patients.17,19,22,23
Patients with this mutation are at particular risk of deep venous thrombosis and may also develop pulmonary embolism, stroke, and peripheral vascular disease.2 Women with recurrent miscarriage have an increased incidence of this condition.3,4 Among patients with no known explanation for deep venous thrombosis, factor V Leiden mutation is a common cause. Patients may also develop skin ulcers.
Histologic features Biopsy of skin lesions shows features of thrombotic vasculopathy.5,6 IgM and C3 deposition has been demonstrated by immunofluorescence staining.5
The cutaneous (and other) lesions are characterized by perivascular hemorrhage; there is no evidence of vasculitis (Fig. 16.131). Bone marrow examination reveals increased numbers of rather immature megakaryocytes. The spleen is congested and shows reactive follicular hyperplasia and sometimes conspicuous megakaryocytes.
Differential diagnosis Biopsy findings are entirely non-specific. Serological and clinical correlation is necessary to arrive at a diagnosis.

Fig. 16.130 Idiopathic thrombocytopenic purpura: these legs show purpura, petechiae, and bruising. By courtesy of N. Slater, MD, St Thomas’ Hospital, London, UK.
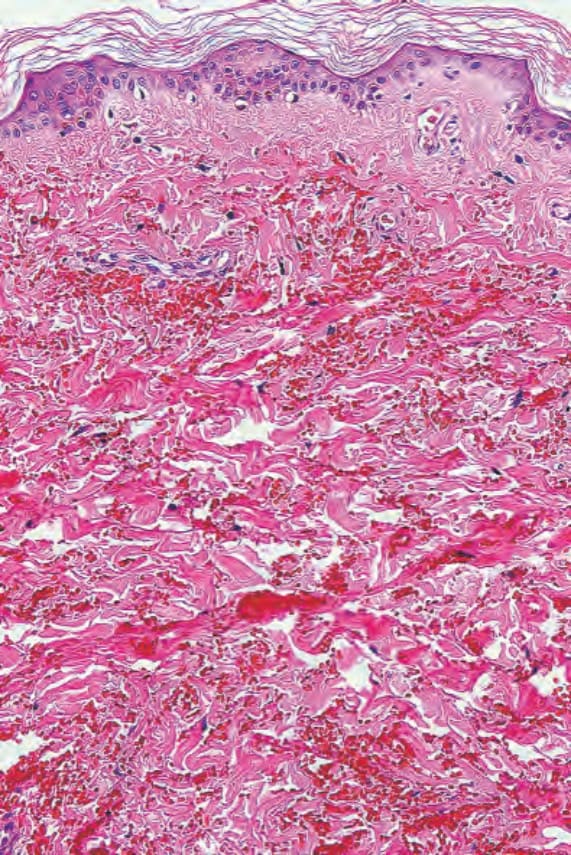
Fig. 16.131 Idiopathic thrombocytopenic purpura: there is hemorrhage but no evidence of vasculitis is seen.