Cryoglobulinemia
Cryoglobulinemia
Cryoglobulins are immunoglobulins that precipitate at low temperatures (4°C) and which redissolve on warming (Fig. 16.123). Typically, the greater
their concentration, the higher the temperature at which they precipitate. This has obvious clinical implications, particularly for plasmapheresis therapy.
Cryoglobulins may be subdivided into three classes: 1–3
• Type I cryoglobulin is composed solely of monoclonal immunoglobulin (either kappa or lambda) and is usually, though not invariably, associated with a variety of lymphoproliferative disorders, including multiple myeloma, Waldenström macroglobulinemia, chronic lymphocytic leukemia, and lymphocytic lymphoma.
• Type II (mixed) cryoglobulin is composed of monoclonal (usually IgM) immunoglobulin reacting against polyclonal IgG.
• Type III (polyclonal) cryoglobulin is composed of polyclonal immunoglobulins (usually IgG and IgM). The last two subtypes (mixed cryoglobulins) function as immune complexes and clinical manifestations are therefore due, at least in part, to allergic vasculitis. Mixed cryoglobulinemia may be clinically subdivided into two forms:
• Essential mixed cryoglobulinemia, in which most patients are infected with the hepatitis C virus.2–4 Hepatitis B virus has been also described in association with essential mixed cryoglobulinemia.2,35
• Secondary mixed cryoglobulinemia, which develops as a complication of a variety of conditions, including connective tissue diseases such as SLE, lymphomas, or infective disease processes (e.g., infective endocarditis and glandular fever).3,6
763 Cryoglobulinemia
but some patients may manifest hematuria, proteinuria (occasionally amounting to the nephrotic syndrome) and, rarely, anuria.9
Mixed cryoglobulinemia is characterized by joint involvement (arthralgia and arthritis), Raynaud phenomenon, fever, purpura, weakness, renal involvement, hepatosplenomegaly, and generalized vasculitis. Cutaneous manifestations include palpable purpura, inflammatory macules and papules, necrotizing vasculitis, crural ulcers and, occasionally, cold urticaria.8,10 Additional rare manifestations include follicular pustular purpura, erythema multiforme, and necrobiotic xanthogranuloma.8,11,12 Renal involvement, most frequently in the form of type 1 mesangioproliferative glomerulonephritis, may be identified by proteinuria, hematuria, and red cell casts.2 Patients can also have polyneuropathies.2 Prognosis is variable. Renal involvement, which occurs in 50% of cases, is associated with high morbidity and mortality.
Given the frequent association of hepatitis virus infection with cryoglobulinemia, it comes as no surprise that some patients develop hepatocellular carcinoma.13,14
Pathogenesis and histologic features In keeping with an immune complex-mediated pathogenesis, hypocomplementemia is the rule. The cryoprecipitate is composed of polyclonal IgG with either monoclonal or polyclonal IgM and is associated with rheumatoid factor properties.3,15 In some patients, hepatitis B virus surface antigen or antihepatitis B antibodies are identified in either the serum or the cryoprecipitate, suggesting a possible causal relationship. Both hepatitis C and hepatitis B viruses have been reported in cases of mixed cryoglobulinemia.16–18 Since most patients with essential mixed cryoglobulinemia are infected with the hepatitis C virus, it appears likely that this represents the cause of this form of the disease and consequently this aspect has received much investigative attention. Hepatitis C virus and hepatitis C virus antigen–antibody complexes have been demonstrated in cryoprecipitates.19 Hepatitis C viral RNA is detected by polymerase chain reaction (PCR) in peripheral blood monocytes of 81% to 90% of patients with mixed cryoglobulinemia.20,21 Hepatitis C genome has also been demonstrated in the bone marrow cells of patients with mixed cryoglobulinemia.22 Interestingly, the E2 envelope protein of the hepatitis C virus binds to CD81, which is present on B lymphocytes.23 What role this interaction plays in the pathogenesis of cryoglobulinemia is poorly understood.23
Clinical features The eponym ‘Meltzer triad’ has been applied to the combined features of purpura, arthralgia, and weakness that are often present.5 Cutaneous manifestations are common to all classes of cryoglobulinemia and are often the presenting complaint.1,3,5,7 Purpura is the most frequent initial sign.
Type I cryoglobulinemia is usually characterized by purpuric lesions, including inflammatory macules and papules on the extremities, accompanied by foci of ulceration (Fig. 16.124).8 Additional features may include livedo reticularis, Raynaud phenomenon, scarring, and infarction, which particularly affects the digits, ears, and nose.8 Renal lesions are uncommon,
High levels of CXCL10 (Interferon-γ-induced protein 10) are found in high levels in hepatitis C-related cryoglobulinemia. It is hypothesized that interferon-γ production from Th1 CD4+ T cells stimulates secretion of CXCL10, resulting in perpetuation of the autoimmune response.24
Other infective agents can also be associated with cryoglobulinemia including protozoa, fungi, bacteria, Chlamydia, and rickettsiae. Cryoglobulinemia has been reported in patients infected with the HIV virus.25–29 However, in HIV patients with circulating cryoglobulins, the clinical symptoms usually associated with cryoglobulinemia are often lacking.25 Another study has shown that in HIV-infected patients the presence of cryoglobulins is significantly associated with increased mortality and risk of developing neoplasia (including B-cell lymphoproliferative disorders).26 Interestingly, disappearance of the symptoms of cryoglobulinemia following infection with the HIV-1 virus has also been reported. The authors of this report speculate on a significant role for CD4+ T cells in the pathogenesis of cryoglobulinemia in a subset of patients.30
The histologic features of monoclonal cryoglobulinemia are those of vascular dilatation, endothelial swelling, and plugging of vascular lumina by hyaline material, which is diastase resistant and PAS positive (Fig. 16.125). Intravascular rouleaux formation may also be a feature.8 On occasion, monoclonal cryoglobulinemia may be associated with leukocytoclastic vasculitis.8
In addition to occasional intracapillary hyaline thrombi, patients with severe renal involvement sometimes manifest features of membranoproliferative glomerulonephritis.
Mixed cryoglobulinemia is associated with immune complex-mediated acute leukocytoclastic vasculitis. The cryoglobulins precipitate in small vessels at low temperature and the resultant complement activation ensures the changes of acute vasculitis. Immunofluorescence is positive for IgG, IgM,
764 Vascular diseases
and complement (Fig. 16.126). Occasionally, intravascular hyaline thrombi are present in early lesions. Red cell extravasation is often a feature.
In biopsies from acute cases, the renal glomeruli show intracapillary thrombi. Other renal manifestations include membranoproliferative glomerulonephritis and vasculitis.
Differential diagnosis The histologic differential diagnosis of monoclonal cryoglobulinemia includes other causes of thrombotic vasculopathy, for example DIC, TTP, protein C deficiency, and warfarin (Coumadin) necrosis. Although subtle histologic clues may suggest cryoglobulinemia, such as the waxy hyaline texture of the casts, definitive diagnosis is based on serological testing for cryoglobulins. The differential diagnosis of mixed cryoglobulinemia includes other causes of leukocytoclastic vasculitis.
A
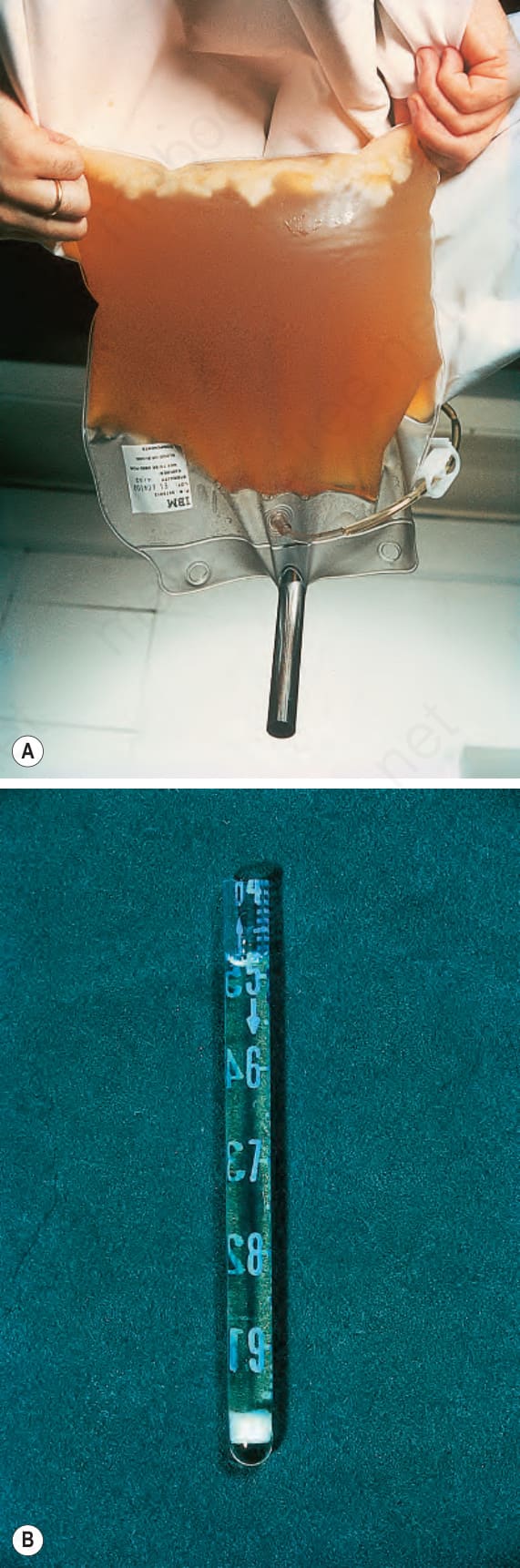
Fig. 16.123 Cryoglobulinemia: (A) there is a large quantity of precipitated cryoglobulin in this plasmapheresis specimen; (B) a cryoprecipitate. By courtesy of N. Slater, MD, St Thomas’ Hospital, London, UK.

Fig. 16.124 Cryoglobulinemia: there is purplish discoloration of the third toe. By courtesy of N. Slater, MD, St Thomas’ Hospital, London, UK.
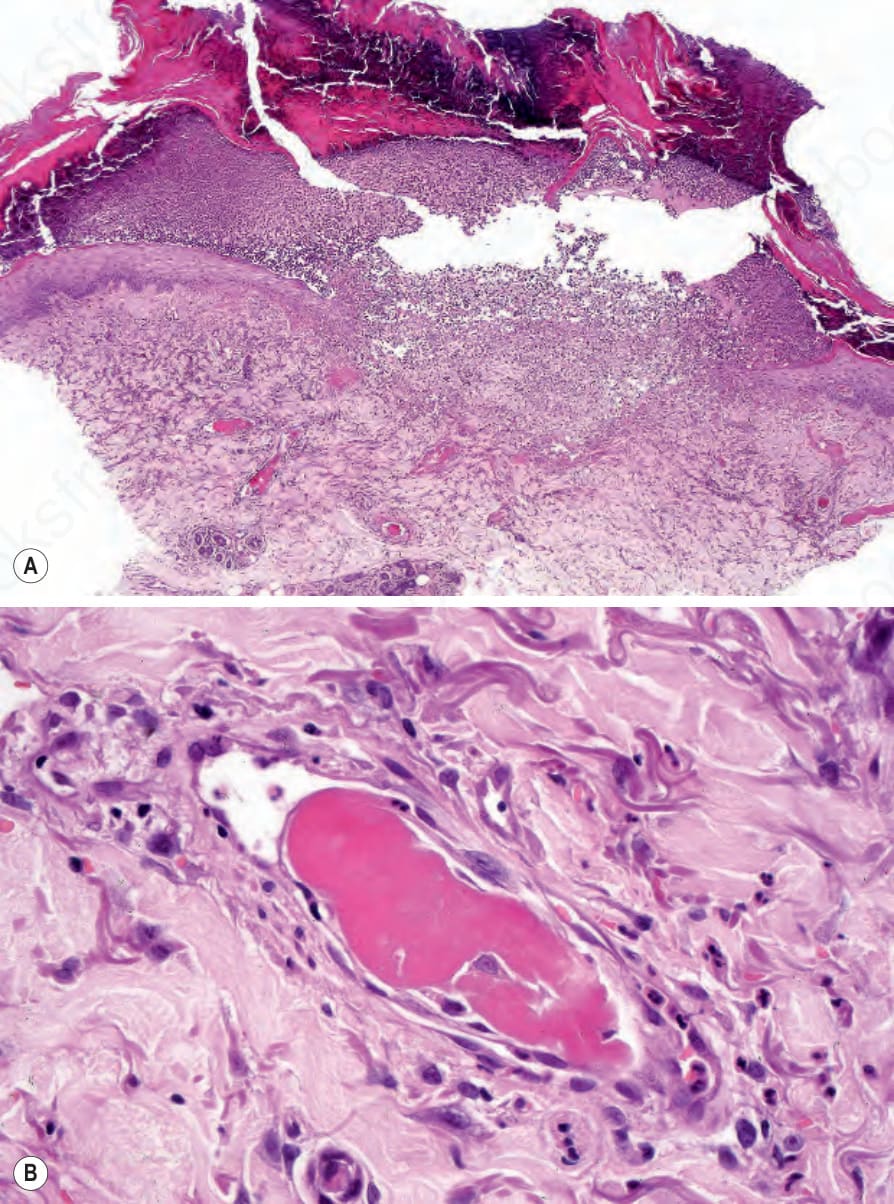
Fig. 16.125 Monoclonal cryoglobulinemia: (A) crusted ulcer with occluded vessels at its base; (B) high-power view of a hyaline thrombus.
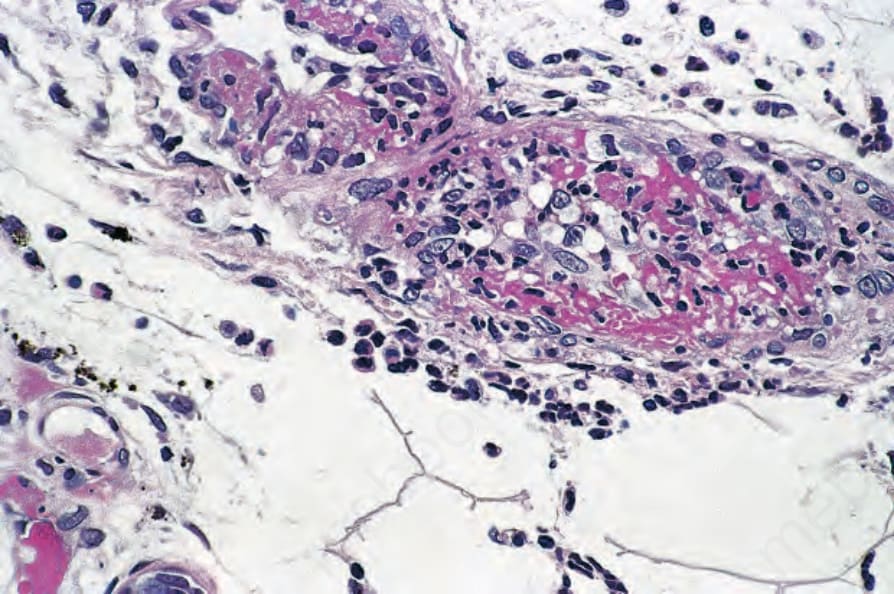
Fig. 16.126 Mixed cryoglobulinemia: in this example, the features of acute leukocytoclastic vasculitis are evident.