Disseminated intravascular coagulation
Disseminated intravascular coagulation
Clinical features Disseminated intravascular coagulation (DIC) is a consumptive coagulopathy that is associated with a wide variety of underlying disorders, many of them life threatening. It is not uncommonly seen in very ill patients and may be acute, subacute, or chronic. Purpura fulminans is a term that has been applied to infection-associated DIC in children. Some authors have applied the term less restrictively to a severe form of DIC associated with high morbidity and mortality.1,2 Purpura fulminans is characterized by an acute syndrome of rapidly progressive and extensive hemorrhagic skin necrosis associated with dermal vascular thrombosis and vascular collapse due to DIC.3,4 A common presentation is symmetrical purpura of the fingers and toes.
Cardiac myxomas are rare but represent the most frequent primary cardiac tumor. Although benign, they are a marker of Carney complex and early recognition is imperative as distant embolization is an important complication associated with high mortality. Cutaneous symptoms include erythematous macules and papules predominantly of acral sites, digital cyanosis, petechiae, splinter hemorrhages, telangiectasia, and livedo reticularis.8–16
DIC is commonly associated with complications of pregnancy and delivery, such as abruptio placentae, sepsis, and amniotic fluid embolism. A wide variety of infections, including bacterial sepsis, meningococcemia, and fungal infections, may also be associated. Massive trauma, heat stroke, shock, snakebite, poisoning, and burns can cause DIC. Malignant neoplasms (including carcinoma of the stomach, breast and colon, small cell carcinoma of the lung, brain, and pancreas) and hematological malignancies have also been associated with this condition.5–14
Pathogenesis and histologic features Cholesterol emboli are found in the small to large arteries and arterioles of the deep dermis or subcutaneous fat (Figs 16.117 and 16.118). Diagnosis depends upon the identification of typical biconvex cleft- or needle-shaped empty spaces (representing evanescent cholesterol crystals dissolved during tissue processing) often associated with atheromatous debris or luminal thrombosis. It is essential, therefore, that deep biopsies are taken. Multiple levels should also be examined because emboli tend to be patchily distributed and are often difficult to detect. The skin supplied by the occluded vessel may be infarcted.
Emboli from atrial myxomas are characterized by the presence of myxoid material within medium-sized vessels. Due to vascular occlusion, this is accompanied by fibrin deposition and a reactive vascular proliferation. Demonstration of the myxoid substance is often difficult and commonly requires examination of multiple levels.
Purpura fulminans occurs predominantly in children and has an equal incidence in males and females. It develops as a complication of a prodromal infectious illness, most commonly meningococcemia, scarlet fever, viral upper respiratory tract infection, chickenpox, rubella, and other exanthemata.15 The disease shows some seasonal variation, being more common in winter and spring. Children develop large confluent ecchymoses, which particularly affect the buttocks, legs, and feet, and commonly appear on the upper limbs and abdomen (Fig. 16.119). The ecchymoses frequently become necrotic, and blood-filled blisters are often found. On occasion the limbs become gangrenous (Fig. 16.120). Fever and hypotension accompany the cutaneous lesions.
761 Disseminated intravascular coagulation
A
B
Hematological studies reveal thrombocytopenia, anemia, and often a leukocytosis. The prothrombin and bleeding times are prolonged. Fibrinogen levels are low and fibrin-fibrinogen degradation products elevated.
Pathogenesis and histologic features As stated above, DIC is not a disease sui generis but represents a coagulopathy resulting from a large number of disorders. These conditions trigger DIC either by causing direct injury to endothelial cells, which causes platelet aggregation, or by increasing circulating procoagulant factors, often tissue
factor. The consequences are thrombosis, fibrinolysis leading to depletion of fibrin, clotting factors and platelets, vascular occlusion, tissue ischemia, and hemorrhage. Clotting factors may be consumed at a rate that exceeds the ability of the liver for synthesis. The coagulopathy, in turn, causes a hemolytic anemia by damaging red blood cells.
762 Vascular diseases
A
Purpura fulminans is sometimes a manifestation of hereditary protein C deficiency, protein S deficiency, Coumadin therapy, and antiphospholipid antibodies.3,16
Biopsy of skin lesions in patients with DIC is characterized by fibrin, platelet, or mixed thrombi in the capillaries and venules, particularly of the skin, but also commonly affecting the internal viscera, including the kidneys, bowel, bladder, and brain (Figs 16.121 and 16.122).3 The number of vessels containing thrombi ranges from scattered to nearly all vessels being involved. Variable numbers of extravasated red blood cells are seen. In patients with purpura fulminans, the thrombi are associated with diffuse and extensive hemorrhage. Early lesions usually show few or no perivascular inflammatory cells. Older lesions are often characterized by epidermal necrosis and subepidermal blood-filled bullae. A mild perivascular inflammatory cell infiltrate of lymphocytes and polymorphs may be present. Infective DIC or purpura fulminans sometimes shows features of a leukocytoclastic vasculitis. Immunofluorescence studies for immunoglobulins and complement are uniformly negative.
Differential diagnosis The differential diagnosis includes other causes of coagulopathy or leukocytoclastic vasculitis. Serological evaluation for disorders of coagulation is
B
required to support the diagnosis. Finally, since successful treatment is both supportive and aimed at the underlying disorder, patients must be evaluated to determine the underlying causes of the DIC.
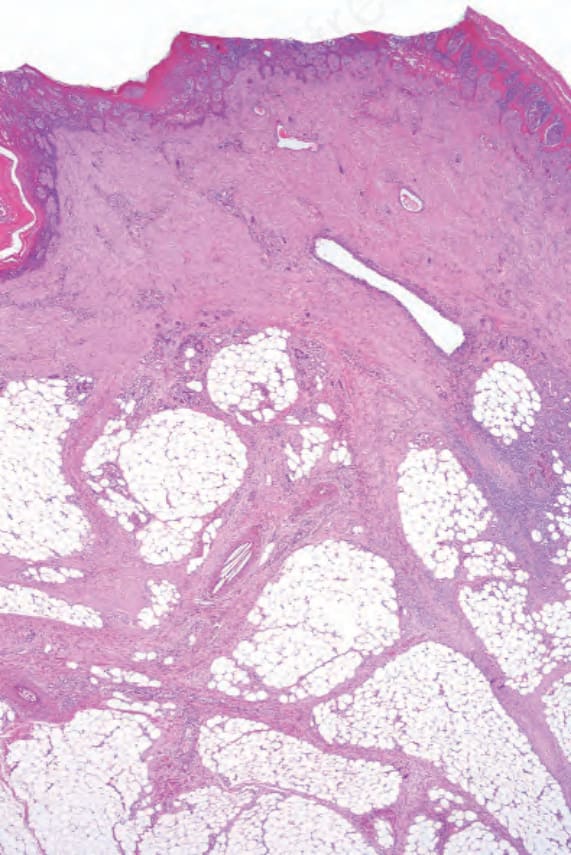
Fig. 16.117 Cholesterol emboli: there is ulceration and dermal scar tissue extending into the septa of the subcutaneous fat. Needle-shaped crystals are present in the lumen of an artery in the middle of the field.
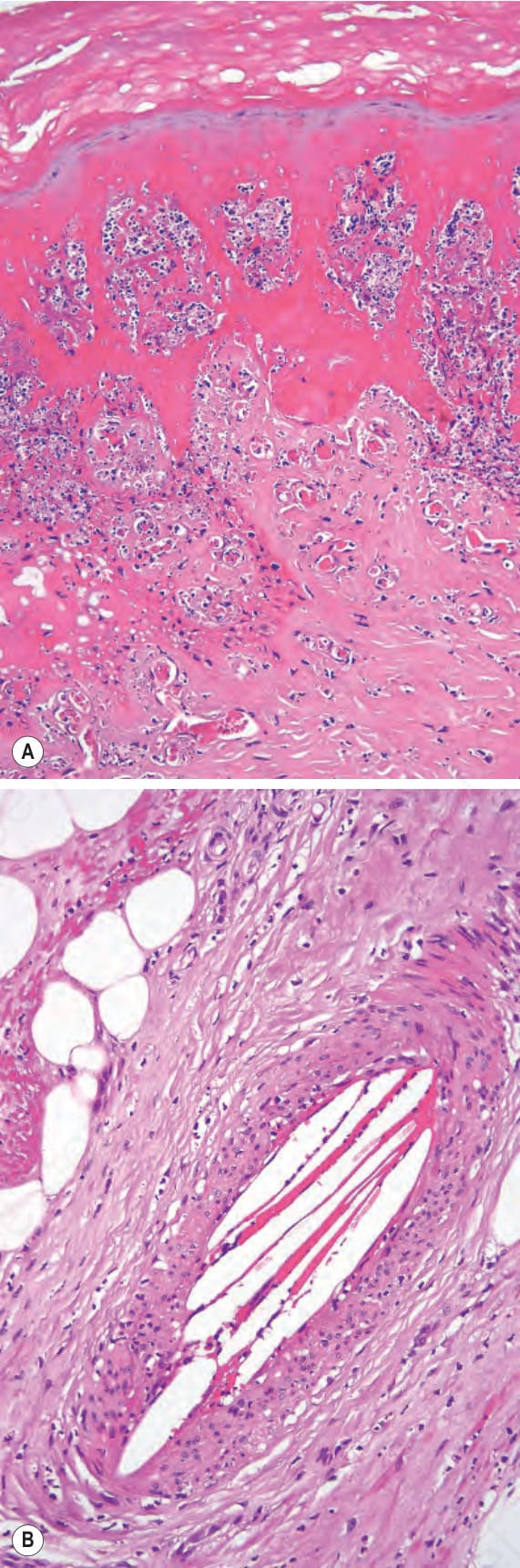
Fig. 16.118 Cholesterol embolism: (A) the overlying epidermis shows full-thickness infarction; (B) high-power view of cholesterol clefts.

Fig. 16.119 Purpura fulminans: bilateral extensive ecchymoses are present on this child’s legs. By courtesy of D. McGibbon, MD, St Thomas’ Hospital, London, UK.

Fig. 16.120 Purpura fulminans: there is complete gangrene of the skin. By courtesy of D. McGibbon, MD, St Thomas’ Hospital, London, UK.
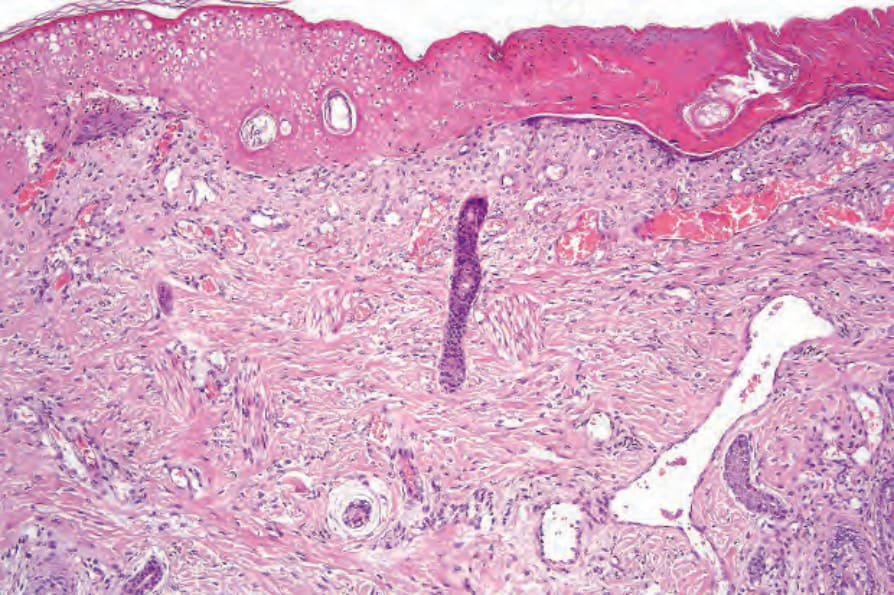
Fig. 16.121 Purpura fulminans: there is epidermal infarction.
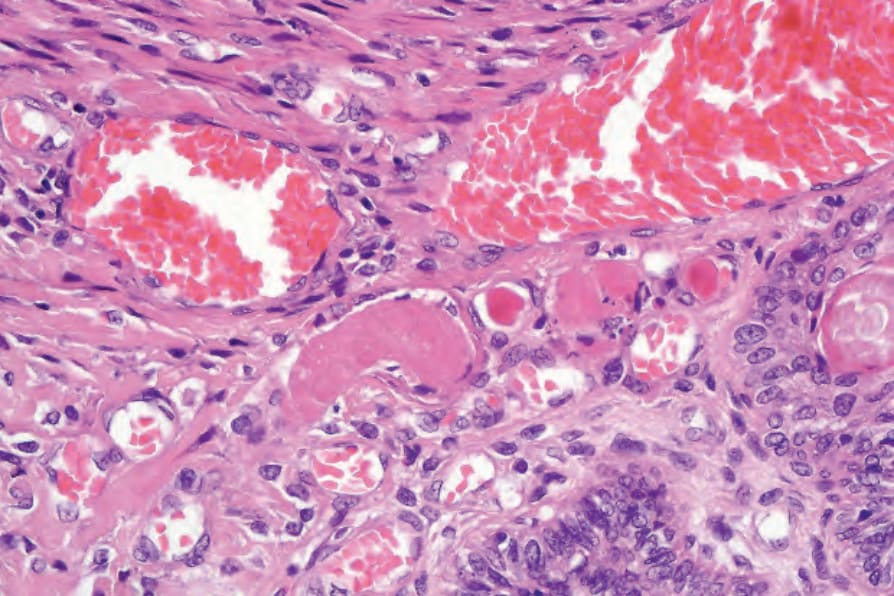
Fig. 16.122 Purpura fulminans: numerous small thrombi are seen in the superficial vessels.
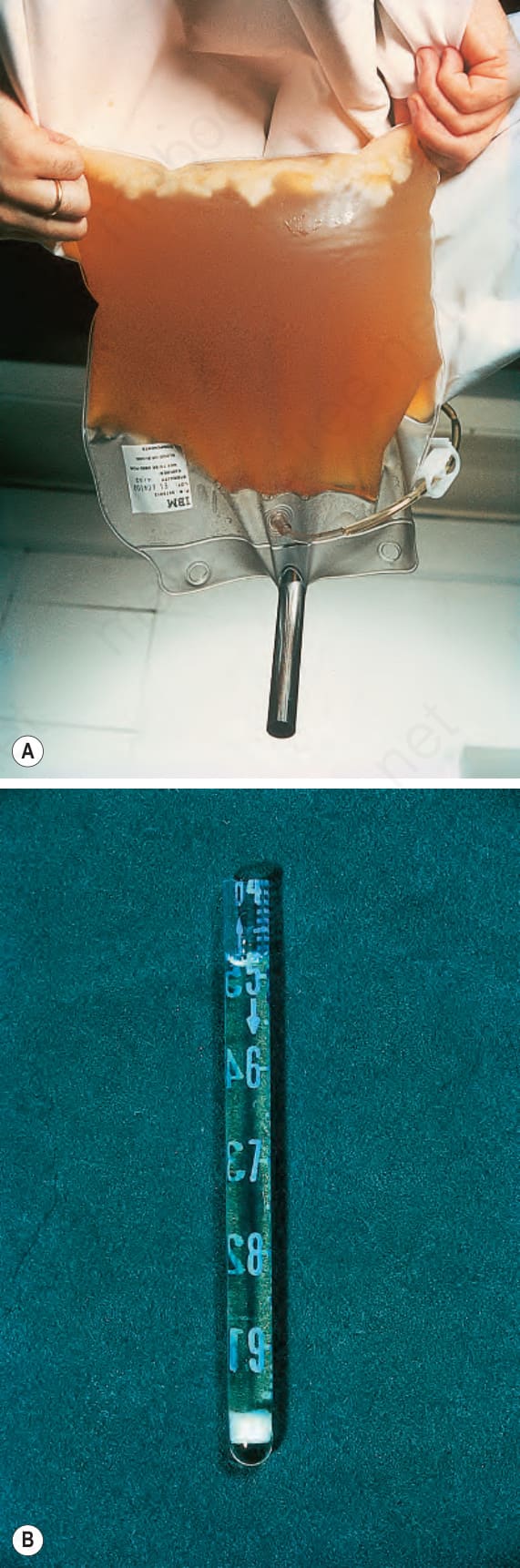
Fig. 16.123 Cryoglobulinemia: (A) there is a large quantity of precipitated cryoglobulin in this plasmapheresis specimen; (B) a cryoprecipitate. By courtesy of N. Slater, MD, St Thomas’ Hospital, London, UK.