Lymphocytic vasculitis
Lymphocytic vasculitis
Pathogenesis and histologic features The pathogenesis of paraneoplastic vasculitis has not been well studied, but could include immune complexes, cross-reacting antigens, and direct tumor (leukemic blast) infiltration of blood vessel walls.
Leukocytoclastic, polyarteritis nodosa-like, and lymphocytic forms of paraneoplastic vasculitis have all been described and show histologic features similar to their nonparaneoplastic counterparts.22
Cases of vasculitis in the setting of myelomonocytic or monocytic leukemia cutis have been described in which the vascular injury was mediated by leukemic blasts.23,24 The term ‘leukemic vasculitis’ has been proposed for this form of vasculitis.23 In these cases, the vasculitis ranged from mild microvascular injury to frank necrotizing vasculitis.23–25 The former was characterized by low-grade vascular injury with endothelial cell swelling and focal fibrin deposition. Frank necrotizing vasculitis shows infiltration of the vessel wall by neoplastic cells associated with necrosis and fibrin deposition in a pattern that resembles polyarteritis nodosa. Hairy cell leukemia may also show infiltration of vessel walls by leukemic cells.4,5
Lymphocytic vasculitis is sometimes diagnosed in cases in which a perivascular lymphocytic infiltrate is associated with vascular damage (Fig. 16.100). In many cases, the vascular changes are subtle and minimal, including only endothelial swelling and extravasated blood cells and sometimes focal fibrin deposition. Not surprisingly, the concept of lymphocytic vasculitis is somewhat controversial.1–5 This category of vasculitis has been embraced by some authors and rejected by others. To a large extent, the controversy is the result of a lack of precisely defined criteria for diagnosis. Kossard has defined lymphocytic vasculitis as an overlapping spectrum of changes varying from angiodestruction to endovasculitis and including a pattern defined as lichenoid lymphocytic vasculitis.6
It is arguable that the term ‘vasculitis’ should not be applied to lesions with minimal vascular damage. Regardless of terminology, it is important for the pathologist to render a report that distinguishes cases of low-grade vascular injury associated with a lymphocytic infiltrate from frank necrotizing
Vasculitis associated with palisaded neutrophilic and granulomatous dermatitis
Clinical features Occasionally, granuloma annulare, necrobiosis lipoidica, and rheumatoid nodule-like lesions associated with vasculitis are encountered.1,2 This group of disorders, which is almost always associated with systemic disease, is also discussed in Chapter 9. A number of different terms have been applied, including palisaded neutrophilic and granulomatous dermatitis (of immune complex disease), interstitial granulomatous dermatitis with arthritis, rheumatoid papules, superficial ulcerating rheumatoid necrobiosis, cutaneous extravascular necrotizing granuloma, and Churg-Strauss granuloma.1–6 Many types of underlying systemic disease have been reported in association with these lesions, including rheumatoid arthritis, lupus erythematosus, Sjögren syndrome, thyroiditis, Raynaud syndrome, hepatitis, inflammatory bowel disease, lymphoproliferative disorders, myelodysplastic syndrome, vasculitis (granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis, Takayasu arteritis, periarteritis nodosa), hemolytic uremic syndrome (HUS), thrombotic thrombocytopenic purpura (TTP), mixed cryoglobulinemia, drug reactions, carcinoma, diabetes mellitus, and infection (streptococcal, HIV, Epstein-Barr virus, erythrovirus).1–4 Patients without underlying systemic disease have also been reported.7
A
The lesions are usually papules and nodules, or plaques with a predilection for the extremities or trunk in an adult.2,6,7,8 They are often arranged in a linear pattern, which may be confluent linear bands or cords that are said to have a ‘ropelike’ quality.
Pathogenesis and histologic features The pathogenesis of palisaded neutrophilic and granulomatous dermatitis likely depends on the associated/underlying disease. An autoimmune-mediated vasculitis probably plays an important role in at least a subset of cases.
As noted above, this is not a single disease but rather a group of disorders showing a broad spectrum of histology sharing the common denominator of a prominent neutrophilic infiltrate with or without vasculitis in a background of palisading granulomatous inflammation. When present, vasculitis usually shows the features of leukocytoclastic vasculitis.
B
• Behçet disease
• Connective tissue disease
• Malignant atrophic papulosis
• Drug eruptions
• ‘Gyrate erythemas’ (e.g., erythema annulare centrifugum)
• Infection (especially viral and rickettsial)
• Insect bite reactions
• Kawasaki syndrome
• Livedoid vasculopathy/atrophie blanche
• Lymphomatoid papulosis
• Perniosis (chilblains)
• Pityriasis lichenoides
• Pigmented purpuric dermatoses
• Polymorphic eruption of pregnancy
• Polymorphous light eruption
• Prurigo of pregnancy
755 Malignant atrophic papulosis
vasculitis. Furthermore, it is important to distinguish lymphocytic from neutrophilic vasculitides.
To avoid any ambiguity, in cases with low-grade vascular injury, we often apply the term low-grade lymphocytic vasculitis and mention in our report that frank necrotizing vasculitis is not present. If strict criteria are used – requiring vascular necrosis or significant fibrinoid change for a diagnosis of vasculitis – frank necrotizing lymphocytic vasculitis is an uncommon condition. The differential diagnosis of lymphocytic vasculitis is broad and many entities associated with a perivascular lymphocytic infiltrate may, on occasion, cause vascular changes that warrant a diagnosis of non-necrotizing lymphocytic vasculitis (Table 16.14). Entities that exceptionally show features of lymphocytic vasculitis are discussed in their appropriate chapters. Diseases commonly associated with lymphocytic vasculitis include Degos disease, perniosis, Behçet disease, livedo vasculitis, and Kawasaki disease. Other rare associations of lymphocytic vasculitis include leukemia and the tumor necrosis factor receptor-associated periodic syndrome. The latter is a periodic fever syndrome associated with a skin eruption presenting with macules and plaques in early life. It results from mutations in the TNFRS- FIA, the gene encoding the tumor necrosis factor receptor.7,8
A
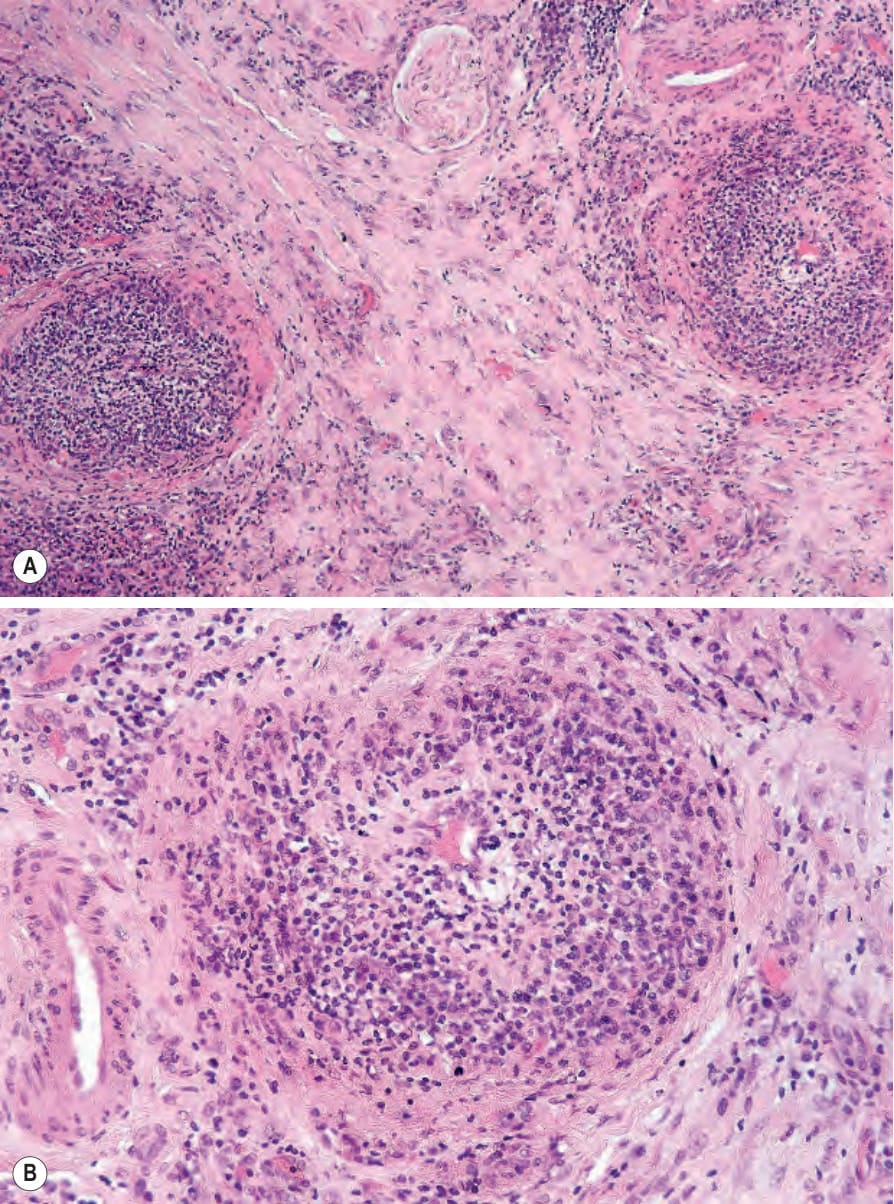
Fig. 16.100 (A, B) Lymphocytic vasculitis: there is mural fibrinoid necrosis accompanied by a dense lymphocytic infiltrate. These images come from a patient with very severe perniosis.
Table 16.14 Causes of lymphocytic vasculitis