Infection-related vasculitis
Infection-related vasculitis
Infection must be considered in the evaluation of many forms of vasculitis, particularly leukocytoclastic vasculitis. Infective vasculitis is caused by a wide variety of agents including bacteria, fungi, protozoa, viruses, spirochetes, and rickettsiae (Table 16.11). The relationship between particular microorganisms and vascular lesions is covered under the specific infection in Chapter 18. In general terms, vessel wall damage may occur as a consequence of direct microbial toxic damage or else develop as a complication of an immunologically mediated injury (Table 16.12).1
B
Bacterial arteritis can develop as a result of embolization from valvular lesions in patients with infective endocarditis. Although many different organisms are of etiological importance in the latter condition, staphylococcal and streptococcal infections remain the most important.2 It may also occur by direct spread from an adjacent septic focus, by lymphatic spread, or represent a manifestation of underlying bacteremia or septicemia. There also appears to be a significant relationship between group A streptococci and childhood polyarteritis nodosa, both cutaneous and generalized.3 In
752 Vascular diseases
Vasculitic syndrome Infective agent
Leukocytoclastic vasculitis (including IgA vasculitis)
Bacterial
Streptococcus Staphylococcus Salmonella Yersinia Mycobacterium Viral
A
varicella-zoster hepatitis B cytomegalovirus influenza
Polyarteritis nodosa Bacterial
Streptococcus Viral
hepatitis A, B, C human immunodeficiency virus cytomegalovirus human T-cell leukemia erythrovirus
Isolated granulomatous vasculitis of the central nervous system
Treponema pallidum Mycobacterium tuberculosis Fungal
B
Coccidioides Actinomyces Cryptococcus Histoplasma Nocardia Aspergillus Borrelia burgorferi (Lyme) Varicella-zoster
Kawasaki disease Bacterial
Streptococcus Salmonella Yersinia Mycoplasma Viral
parainfluenza rotavirus
Reproduced with permission from Mader, R. and Keystone, E.C. (1992) Current Opinion in Rheumatology, 4, 35–38.
• Direct microbial toxicity – direct endothelial infection – effect of microbial toxins
• Immune mediated – humoral: soluble immune complexes; in situ complex formation – cellular: cytotoxic cell reaction (T cell, NK cell, other); polyclonal T- or
B-cell response; monoclonal T- or B-cell response
NK, natural killer. Reproduced with permission from Calabrese, L.H. (1991) Rheumatic Disease Clinics of North America, 17, 131–147.
addition, Kawasaki disease has been reported in association with group A streptococci, possibly as a result of superantigen stimulation.4 Gonococcal bacteremia due to Neisseria gonorrhea is another important cause of vasculitis. Neisseria meningitis infection may result in vasculitis associated with considerable morbidity and mortality.
The histologic features of small-vessel involvement are variable and depend to some extent on the nature of the causative organism. Suppurative features are most likely to be due to staphylococcal, streptococcal, Pseudomonas or Klebsiella infection.2 A Gram stain is advisable in all suspected cases.
Obviously, in the context of immunosuppressed patients, the range of bacteria and fungi that can be implicated is very broad. In cases of suspected cutaneous infective vasculitis, especially in immunosuppressed patients, a detailed clinical history is essential and the judicious use of special stains is highly advisable.
Candidiasis, aspergillosis, cryptococcosis, and mucormycosis are of special importance. M. tuberculosis is also sometimes a cause of vascular damage. It tends to affect veins rather than arteries.2 The features are usually those of a granulomatous thrombophlebitis, usually in the absence of caseation necrosis, although sometimes this is a feature. Occasionally, however, arteries are primarily affected (Fig. 16.99).
753 Paraneoplastic vasculitis
The best known viral association with vasculitis is hepatitis B, which has been described in association with polyarteritis nodosa, leukocytoclastic vasculitis, and mixed cryoglobulinemia, and hepatitis C associated mixed cryoglobulinemia and leukocytoclastic vasculitis.1,9–12 Evidence of hepatitis B infection is found in approximately 35% of all patients with polyarteritis nodosa.1
HIV may be present in a very wide spectrum of vasculitic lesions including polyarteritis nodosa, eosinophilic granulomatosis with polyangiitis, leukocytoclastic vasculitis, IgA vasculitis, lymphomatoid granulomatosis, and primary angiitis of the central nervous system.13–15 Whether these represent a direct effect of HIV, or are a consequence of coexisting viral infections known to cause vasculitis (e.g., cytomegalovirus, HBV or Epstein-Barr virus), is unknown.10 The identification of HIV within endothelial cells adds some support to the former possibility.16
Lepra bacilli are very commonly seen in endothelial and vascular smooth muscle cells in lepromatous leprosy. Vasculitis in the setting of leprosy (erythema nodosum leprosum) is a common cause of vasculitis in regions of the world where this disease is endemic.
Vascular lesions in the skin accompany a variety of rickettsial infections including epidemic typhus, scrub typhus, and Rocky Mountain spotted fever.2,5 The histologic features include endothelial swelling and a mixed inflammatory cell infiltrate of T lymphocytes, macrophages, and occasionally neutrophils.2 Thrombosis is sometimes present.
Small-vessel vasculitis may be seen in all three stages of syphilis. The features vary from a non-specific lymphocytic inflammation through to necrotizing granulomatous angiitis.6–8 Treponema pallidum, however, is very rarely identified.2 Cutaneous vasculitis is an occasional feature of Lyme disease.2

Fig. 16.96 Takayasu arteritis: (A) this patient presented with multiple lesions as seen here on the lower legs; (B) a large ulcerated inflammatory nodule is present on the left thigh. By courtesy of P. Godeau, MD, and C. Francès, MD, Groupe Hospitalier, Pitié-Salpêtrière, Paris, France.
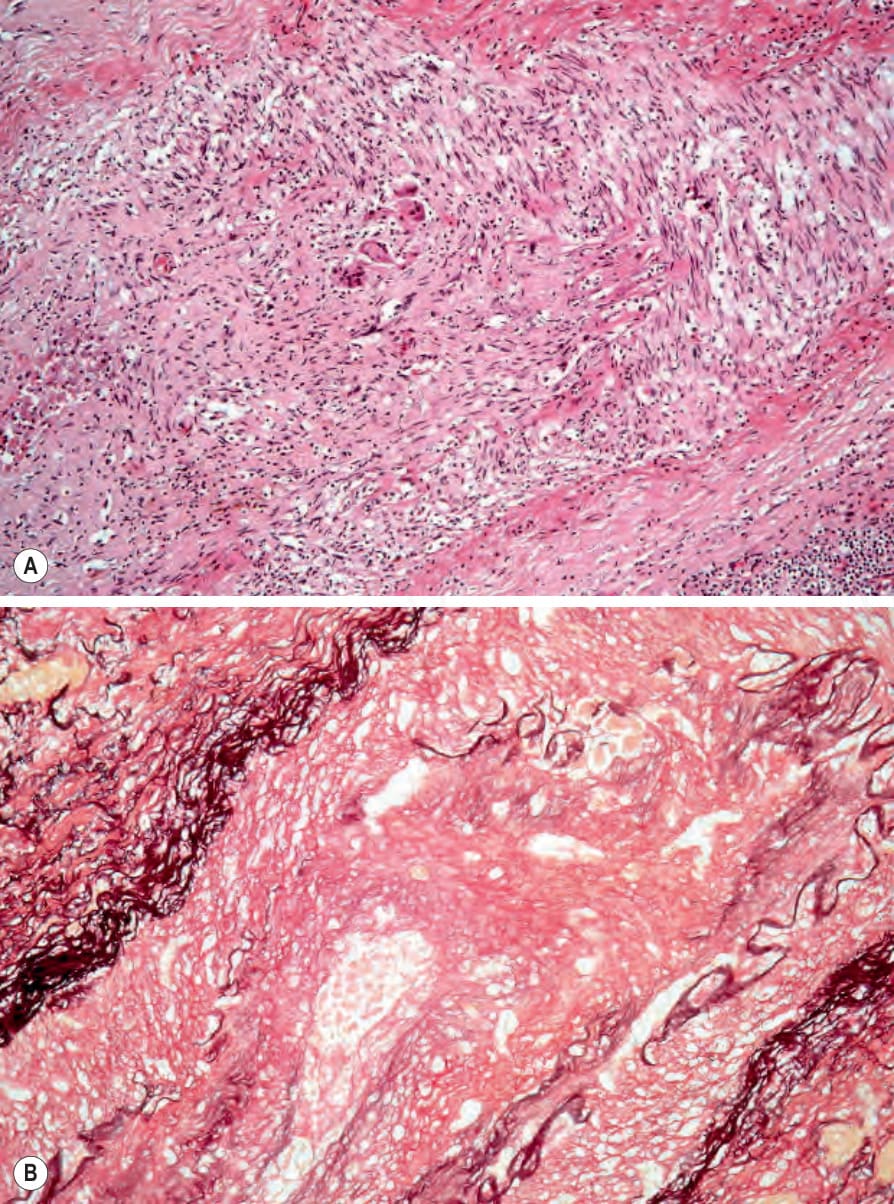
Fig. 16.97 (A, B) Takayasu arteritis: this occluded artery was present with a thickened septum of the subcutaneous fat from the thigh of a young woman.
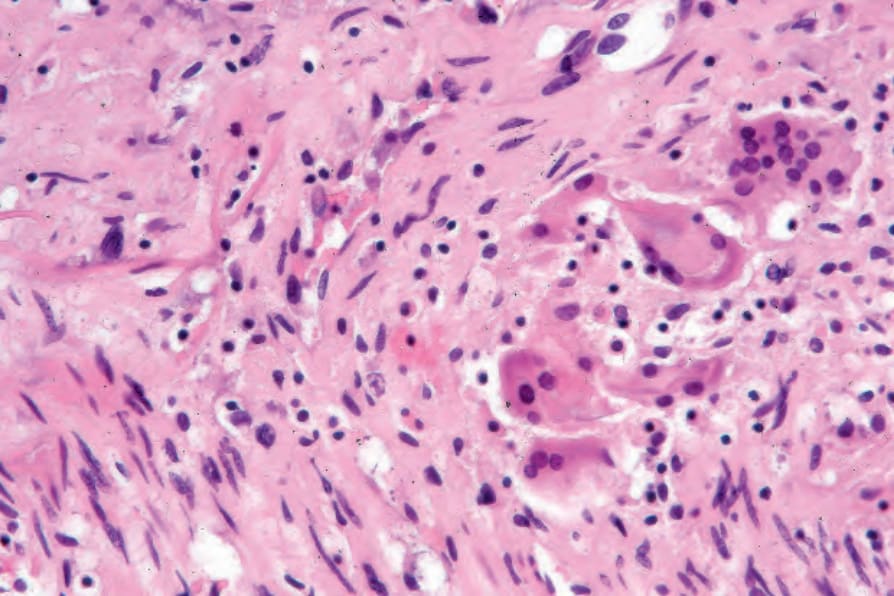
Fig. 16.98 Takayasu arteritis: high-power view showing granulomatous inflammation. The features are indistinguishable from giant cell arteritis.
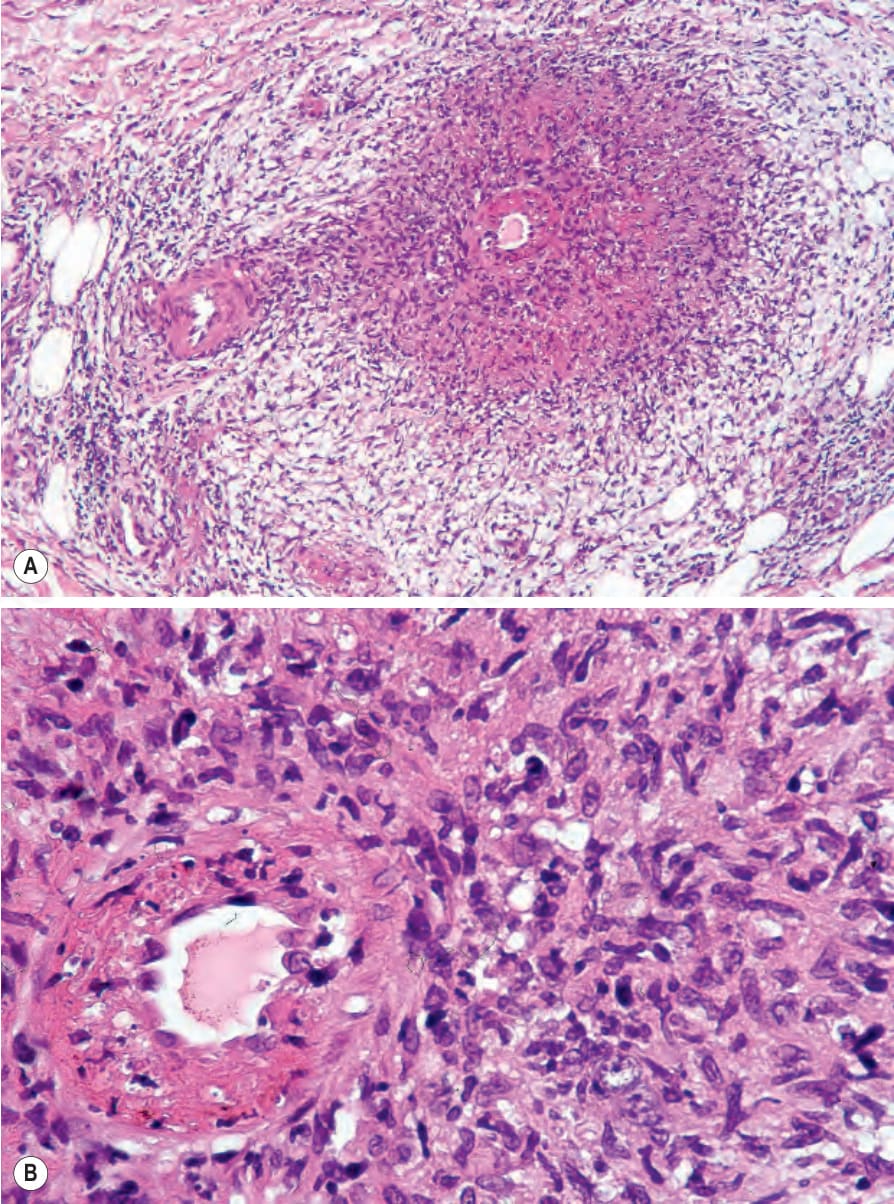
Fig. 16.99 (A, B) Tuberculous vasculitis: this patient with miliary tuberculosis presented with ischemic cutaneous lesions. Note the granulomatous inflammation.
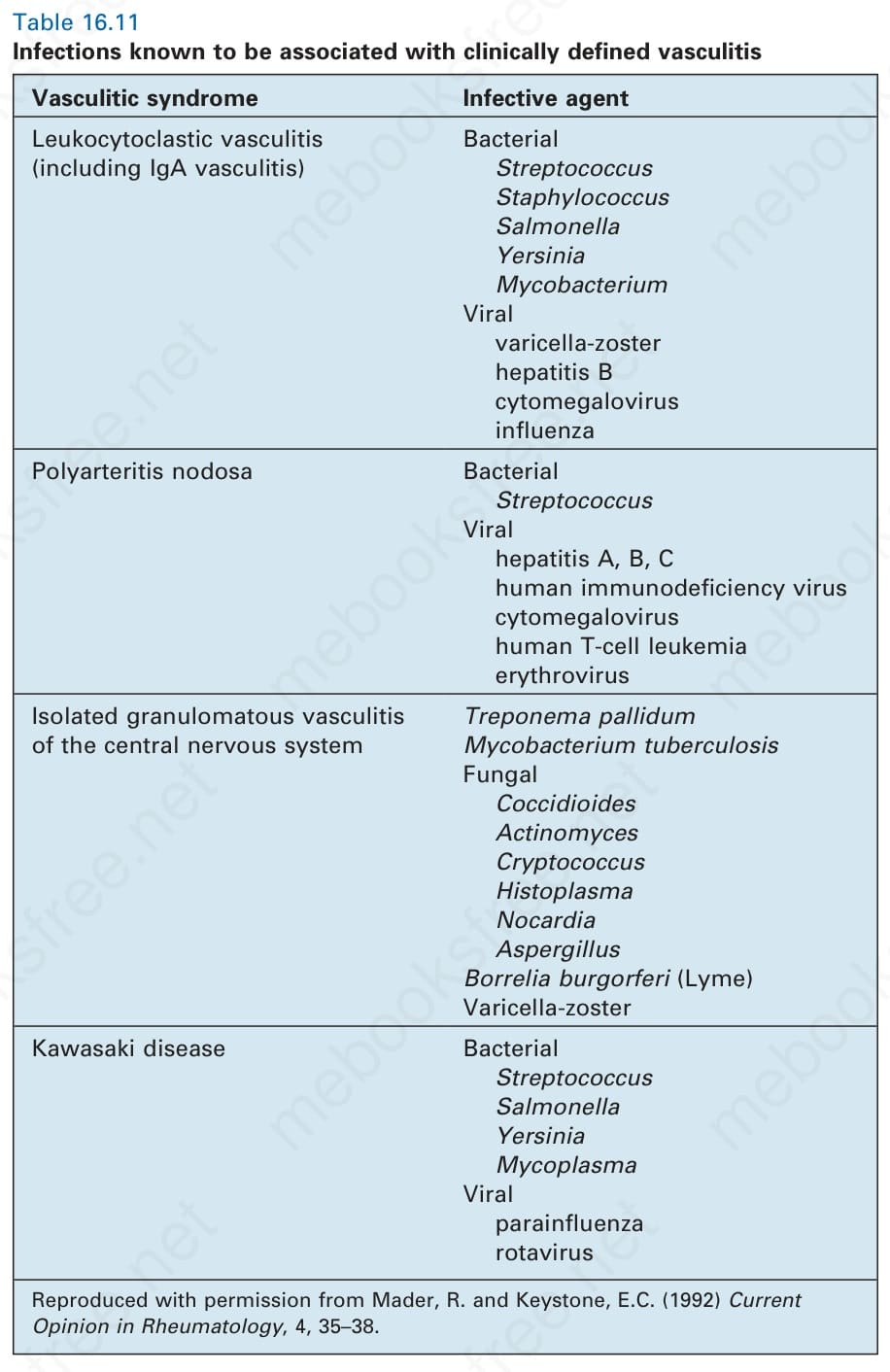
Table 16.11 Infections known to be associated with clinically defined vasculitis
Table 16.12 Mechanisms for infection-associated vasculitis