Takayasu arteritis
Takayasu arteritis
Clinical features Takayasu arteritis (pulseless disease, giant cell arteritis) is a rare granulomatous disease that predominantly affects the aorta and its major branches and results in vascular stenoses with bruits and diminished or absent pulses (hence the term ‘pulseless disease’).1,2 Aneurysm formation may be an additional feature. It predominantly affects females (7 : 1), most often involves the upper limbs, and usually presents in the second or third decade. Although most patients are young adults, the disease is also seen in children.3–7 It is rare in Europe and the United States, occurring more often in Japan, China, Korea, Southeast Asia, India, and Mexico.2 It appears to have two stages:
• an acute systemic illness characterized by fever, malaise, arthralgias, myalgias, and ocular lesions including uveitis and episcleritis,
• a chronic stage of large-vessel involvement.8
It is crucial to note that patients with classic symptoms of giant cell arteritis may have a negative biopsy, most likely due to the multifocal nature of the arteritis and sampling bias. Negative biopsies may be seen in 15% to 44% of patients with clinical manifestations of giant cell arteritis.40,41 Therefore, a negative biopsy does not necessarily exclude this disease. Given the consequences of delayed or no treatment, it is often necessary to treat selected patients even without definitive biopsy diagnosis. One study found that patients with giant cell arteritis who have constitutional symptoms or an abnormal temporal artery detected by physical examination are more likely to have a positive biopsy.42 Doppler flow studies may be used to improve the sensitivity of biopsy.43 Magnetic resonance imaging can also be useful in biopsy negative cases, but they need to be done promptly, as corticosteroid therapy can reduce the sensitivity of the test.44 Given the multifocal nature of giant cell arteritis, the diagnostic yield, not surprisingly, is likely improved with longer artery length biopsied and increased number of sections examined.45
Current diagnostic criteria are shown in Table 16.10. In addition to the obligatory criterion, the presence of two major criteria, one major plus two or more minor, or four or more minor criteria, is associated with a high probability of Takayasu arteritis.9
Cutaneous manifestations have been described in up to 50% of patients and include Raynaud syndrome (due to large-vessel involvement), acute inflammatory nodules and erythema nodosum-like features (particularly in Europe and North America), pyoderma gangrenosum-like lesions (especially in the Japanese), pseudoerythema induratum, superficial phlebitis, tuberculid eruptions, and purpura (Fig. 16.96).8,10,11 Patients may present with cutaneous necrotizing vasculitis.11 Rare associations with Sweet syndrome, pyoderma gangrenosum, and ulcerative cutaneous sarcoidosis have been reported.12,13
• Obligatory criterion – age < 40 years
• Major criteria – left mid subclavian artery lesion – right mid subclavian artery lesion
• Minor criteria – high ESR – carotid artery tenderness – hypertension – aortic regurgitation or annuloaortic ectasia – pulmonary artery lesion – left mid common carotid lesion – distal brachiocephalic trunk lesion – descending thoracic aorta lesion – abdominal aorta lesion
751 Infection-related vasculitis
Reproduced with permission from Bentsson, B.A. and Anderson, T. (1991) Current Opinion in Rheumatology, 3, 15–22.
Cases have been reported describing an overlap between Takayasu arteritis and polyarteritis nodosa.9 Rare patients with a lupus-like malar flush and an urticarial reaction with livedo reticularis have been documented.10 Renal artery involvement with stenosis causes severe hypertension secondary to renin secretion. Stroke due to severe hypertension is a serious complication in some patients. Patients with Takayasu arteritis also have an increased incidence of associated Crohn disease.15
Pathogenesis and histologic features The etiology and pathogenesis of Takayasu arteritis is poorly understood. Occasionally, other diseases are seen in association with Takayasu arteritis including tuberculosis, inflammatory bowel disease, polymyositis, sarcoidosis, and rheumatoid arthritis.1,8,14,16–18 Coexpression with polyarteritis nodosa raises the possibility of an autoimmune phenomenon.19
A genetic component may also be present. Takayasu arteritis is associated with HLA-B52, HLA-B39, HLA-DRB11502, HLA-DRB10405, HLA-B/MICA, and HLA-DQB1/HLA-DRB1.20 There is also an association with genes for FC-gamma receptor IIA and FC-gamma receptor IIIA.20 The latter two haplotypes have also been associated with giant cell arteritis.21
A
The diagnosis is usually made by clinical and radiological correlation; however, in some cases tissue is sent to the pathologist. The histologic features are variable and include granulomatous vasculitis indistinguishable from giant cell arteritis, leukocytoclastic vasculitis, lymphocytic vasculitis, and polyarteritis nodosa-like features (Figs 16.97 and 16.98).8–10,19,22
Septal and lobular panniculitis with granulomatous vasculitis may be the underlying histology of erythematous nodules and erythema nodosum-like lesions.10 Features of Churg-Strauss granulomata have also been reported.8
Differential diagnosis As can be seen from the above discussion, several different patterns of vasculitis may be encountered in Takayasu arteritis. Furthermore, the histologic findings seen in this disease may be identical to other forms of vasculitis. Therefore, careful clinical and radiological correlation is necessary to establish the correct diagnosis.

Fig. 16.96 Takayasu arteritis: (A) this patient presented with multiple lesions as seen here on the lower legs; (B) a large ulcerated inflammatory nodule is present on the left thigh. By courtesy of P. Godeau, MD, and C. Francès, MD, Groupe Hospitalier, Pitié-Salpêtrière, Paris, France.
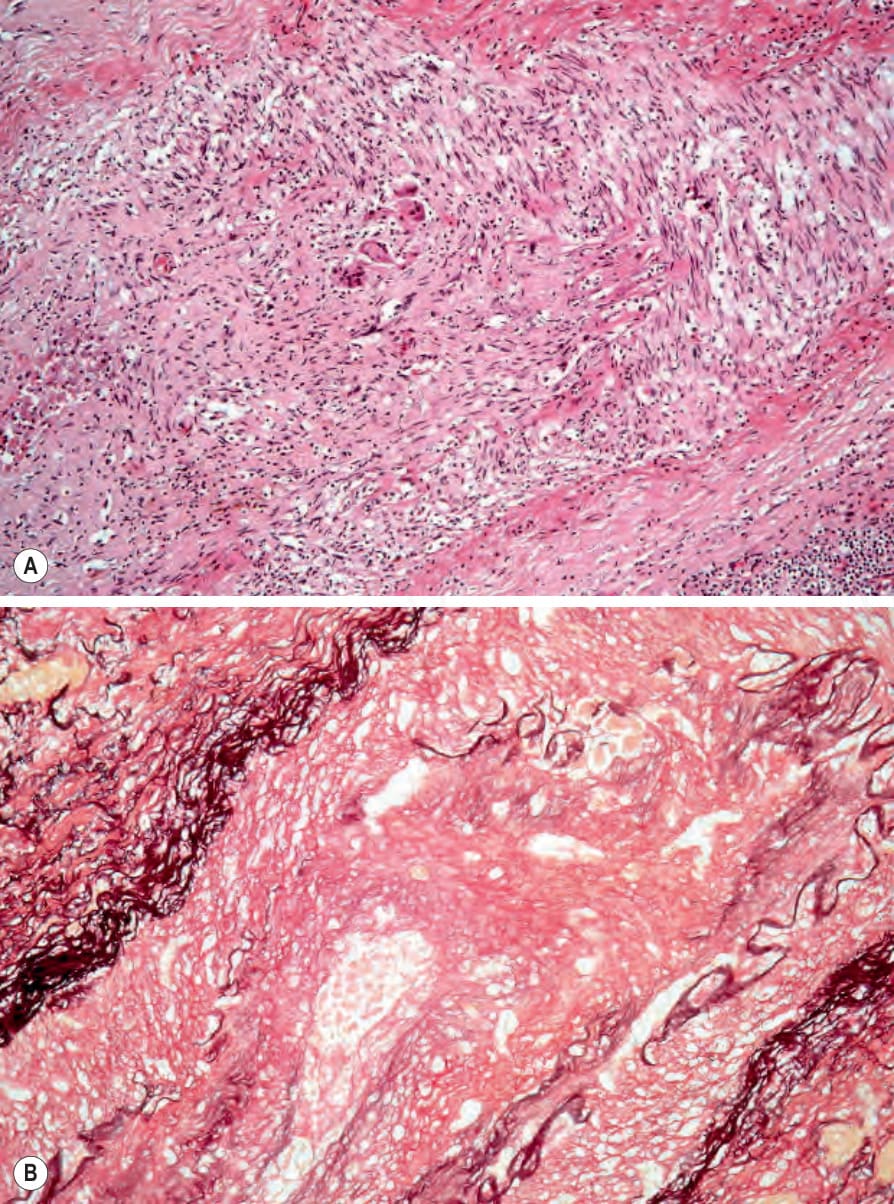
Fig. 16.97 (A, B) Takayasu arteritis: this occluded artery was present with a thickened septum of the subcutaneous fat from the thigh of a young woman.
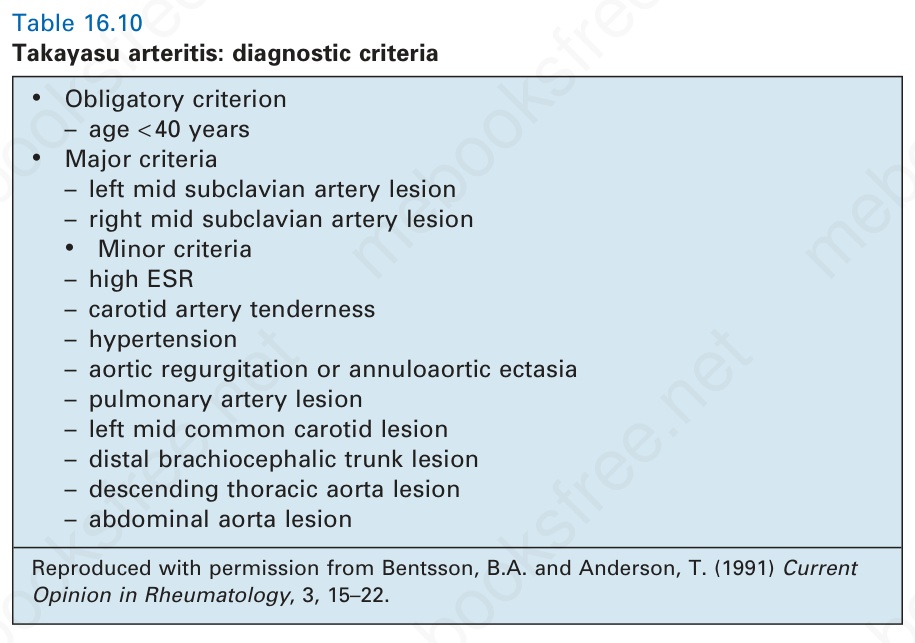
Table 16.10 Takayasu arteritis: diagnostic criteria