Juvenile temporal arteritis
Juvenile temporal arteritis
Clinical features Juvenile temporal arteritis is a rare and poorly defined entity first reported in 1975.1 Thus far, only approximately 20 cases have been reported in the literature.2–10 The disease is unrelated to classic temporal arteritis and is not associated with abnormal ESR or signs of systemic involvement. It occurs in patients under the age of 40, most commonly manifesting as a unilateral painless nodule or swelling of a few centimeters in the temporal area.1–10 Painful presentation and bilateral involvement are rare features.2–4 The disease may be accompanied by blood eosinophilia and it may be related to or associated with Kimura disease.4,5,7,9–11
Histologic features Juvenile temporal arteritis is characterized by intimal proliferation and disruption of the media of the temporal artery associated with a heavy chronic inflammatory infiltrate composed predominantly of lymphocytes and eosinophils.10 Endothelial proliferation is an additional finding and formation of lymphoid follicles and germinal centers may be present.12 Giant cells as seen in classical temporal arteritis are not a feature.
circumferential defects in the elastic lamina, and there is a mantle of lymphocytes and epithelioid histiocytes between the outer muscular layer and the adventitia.39 These changes can be noted as early as 1 week following steroid treatment.39
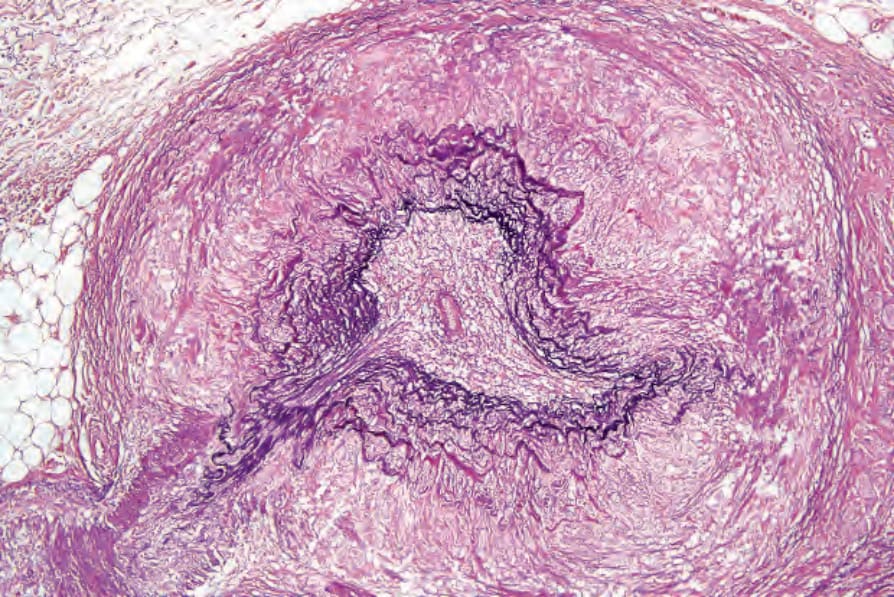
Fig. 16.95 Giant cell arteritis: there is fragmentation of the internal elastic lamina. By courtesy of P.A. Burton, MD, Southmead Hospital, Bristol, UK.