Giant cell arteritis (temporal arteritis)
Giant cell arteritis (temporal arteritis)
Clinical features Giant cell arteritis, formerly also called temporal arteritis, is a disease of the elderly that shows a marked female predominance (3 : 1).1,2 It is a generalized vasculitis that predominantly affects large and medium-sized arteries.3 It is mainly seen in Caucasians and its etiology is unknown.2,3
Five of the American College of Rheumatology 1990 criteria are outlined in Table 16.9.1 Classically, the temporal arteries are primarily affected, but giant cell arteritis may also affect the occipital or facial arteries and, in fact, has the potential to involve virtually any medium-sized or large vessel, including the aorta and its branches.3 Given that temporal arteries may be uninvolved, giant cell arteritis is the preferred terminology in the current Chapel Hill Consensus conference classification.4 Patients with giant cell arteritis classically present with severe headache, pyrexia, and throbbing scalp pain. Clinical examination may reveal scalp tenderness and the skin overlying the affected vessel may be erythematous, edematous, or appear bruised.5,6 Palpation often reveals a cordlike and nodular vessel. Pulsation can be diminished or absent.
Visual disturbance, present in 25% to 50% of patients, due to involvement of the ophthalmic or retinal vessels is an important complication which sometimes results in blindness.6 Lesions of the CNS may result in
748 Vascular diseases
A
A
B
B
stroke, subarachnoid hemorrhage, or mental confusion, and aural involvement can cause deafness. In one large study, neurological problems were present in nearly one-third of patients.7 Peripheral neuropathic syndromes are evident in 14% of patients.5 Often the associated lymph nodes are enlarged and tender. Symptoms of polymyalgia rheumatica (i.e., stiffness, weakness, aching and pain in the muscles of the neck, limb girdles, and upper limbs) are extremely common, occurring in 40% to 75% of patients with giant cell arteritis.8,9 Giant cell arteritis, however, is present in approximately 20% of patients with polymyalgia rheumatica.9 Laboratory investigations typically reveal mild anemia, neutrophilia, and a very high ESR. Elevated levels of von Willebrand factor are characteristic.10 Patients may also have hyperthyroidism and abnormal liver function tests with elevated alkaline phosphatase and transaminases.6
Criterion Definition
Age at disease onset ≥ 50 years
Development of symptoms or findings beginning at age 50 or older
Cutaneous lesions other than those mentioned above are uncommon, presumably reflecting the vast collateral circulation of the integument.11–12 Patients may occasionally manifest ulcers (sometimes quite widespread), massive necrosis, bullae, and gangrene (Fig. 16.92).13,14 Involvement of the lingual artery can cause glossitis or gangrene of the tongue.15,16 Masticatory claudication is an additional feature.6
Rare patients with disseminated visceral arteritis with giant cell arteritis-like histologic features have been described.17 The heart, lungs, kidneys, stomach, pancreas, and liver may be involved.17 It is debatable what terminology should be applied to such rare and unusual cases.
Life expectancy does not seem to be adversely affected by having temporal arteritis.18
New headache New onset of, or new type of, localized pain in the head
Temporal artery abnormality
Temporal artery tenderness to palpation or decreased pulsation, unrelated to arteriosclerosis of cervical arteries
Elevated ESR ESR ≥ 50 mm/h by the Westergren method
Abnormal artery biopsy
Biopsy specimen with artery showing vasculitis characterized by a predominance of mononuclear cell infiltration or granulomatous inflammation, usually with multinucleated giant cells
*For purposes of classification, a patient shall be said to have giant cell (temporal) arteritis if at least three of these five criteria are present. The presence of any three or more criteria yields a sensitivity of 93.5% and a specificity of 91.2%. Reproduced with permission from Hunder, G.G. (1990) Arthritis & Rheumatism, 33, 1122–1128.
749 Giant cell arteritis (temporal arteritis)
A
The vast majority of patients have an elevated ESR.19 C-reactive protein is also typically elevated.19 Elevated levels of anticardiolipin antibodies are frequently present.20–23 Some studies suggest that the presence of anticardiolipin antibodies correlates with more severe vascular damage.22,23 In most patients, anticardiolipin antibody titers return to normal range with steroid therapy.21
Pathogenesis and histologic features The pathogenesis of giant cell arteritis is poorly understood. Although an immunological mechanism has been suggested, it has not been proven. Evidence of familial aggregation and an increased incidence of the HLA-DR4 antigen have raised the possibility of a genetic influence.3 However, consistent reproducible HLA associations have not been demonstrated in all populations.
B
It has been suggested that giant cell arteritis is an autoimmune disease perhaps directed, at least in part, against the vascular elastic lamina.3 T cells in the infiltrate are predominantly of the helper subclass and expression of HLA-DR has been recorded, thereby suggesting that they are activated.3 The lymphocytes have been shown to respond to antibodies against transferrin and IL-2 receptors.24 Proliferation of mononuclear cells following incubation in cultures containing elastin-derived peptides is increased compared with control subjects.25 This finding suggests elastin-derived peptides are the targets of T cells in giant cell arteritis.25 Disease activity has been shown to correlate with plasma concentrations of IL-6.26 It has also been shown that CD4-positive T-cell expressing CD161 are present in the arterial wall. These cells then polarize into Th1 and Th17 cells, resulting in IFN-γ production that activates macrophages, giant cells, and vascular smooth muscle cells.27 This could account for the vascular damage and resulting ischemia.
sun damage-related changes.35–37 Despite these observations, the precise triggering factors and the pathogenesis of giant cell arteritis remain unclear.
The lesions of giant cell arteritis are typically focal in distribution; therefore, the vessel should be carefully palpated to find an obviously affected segment before a biopsy is undertaken. Even then, false negatives are not uncommon (see below). The lesion is granulomatous in nature and may affect only part or the whole circumference of the vessel wall (Fig. 16.93).38 The infiltrate, which particularly affects the intima and media, is composed of lymphocytes, plasma cells, histiocytes, and variable numbers of giant cells of both foreign body and Langhans type (Fig. 16.94). Giant cells are sometimes relatively sparse and multiple levels have to be examined before they are identified. On occasion, they are absent. Typical of giant cell arteritis is damage to the internal elastic lamina, which appears swollen and fragmented, and portions may be identified within the cytoplasm of giant cells (Fig. 16.95).5
The demonstration by some authors of a fluctuating cyclical pattern of incidence has raised the possibility of an infectious agent or other triggering factor playing a significant pathogenetic role.28–30 A study from the Mayo Clinic showed a variation in incidence with peak periods occurring approximately every 7 years.28 Similarly, a study from Denmark demonstrated marked variation in the incidence of temporal arteritis with five peak periods.30 Of these, there appeared to be association with two epidemics of M. pneumoniae infection, two possibly related to erythrovirus (parvovirus) B19 epidemics, and one peak that may have been related to an epidemic of Chlamydia pneumoniae.30 Another study showed a threefold increased likelihood of infection in patients with giant cell arteritis compared with control subjects.31 An association between giant cell arteritis and antibodies to parainfluenza type 1 has been demonstrated.32,33 Other large studies have found no seasonal variation, casting some doubt on the infectious hypothesis.34 A different hypothesis implicated altered endogenous material due to age- or
A second, less common form consists of a panarteritis composed of lymphocytes, macrophages, neutrophils, and eosinophils but giant cells are absent. Varying degrees of vessel wall necrosis are evident and the vessel is often thrombosed.
In the late stages of the disease, fibrous scarring takes place and a reconstituted, often multilayered, internal elastic lamina may be identified. In cases of doubt, an elastic tissue stain can prove invaluable. The thrombus is on occasions recanalized.
Initiation of corticosteroid treatment before biopsy influences the histologic appearances.39 Giant cells are rare or entirely absent, there are large
750 Vascular diseases
Differential diagnosis The histologic findings are identical to those seen in some patients with Takayasu arteritis, another form of giant cell arteritis. Careful clinical correlation is required to distinguish these conditions and, since overlap exists, many cases are not easily subclassified. Some authors consider these diseases part of a continuum of giant cell vasculitis, with patient age being an important discriminator: patients under age 40 are more likely to have Takayasu arteritis; those over 50 are more likely to have giant cell arteritis.
It should be noted that fragmentation of the internal elastic lamina may result from either age-related changes or atherosclerosis and these conditions may be difficult to distinguish from healed arteritis. The presence of medial scarring is suggestive of giant cell arteritis. The extent of destruction, particularly confluent loss of the internal elastic lamina, is said to correlate with probability of healed arteritis.8

Fig. 16.89 Thromboangiitis obliterans: digital gangrene is present in this amputation specimen.
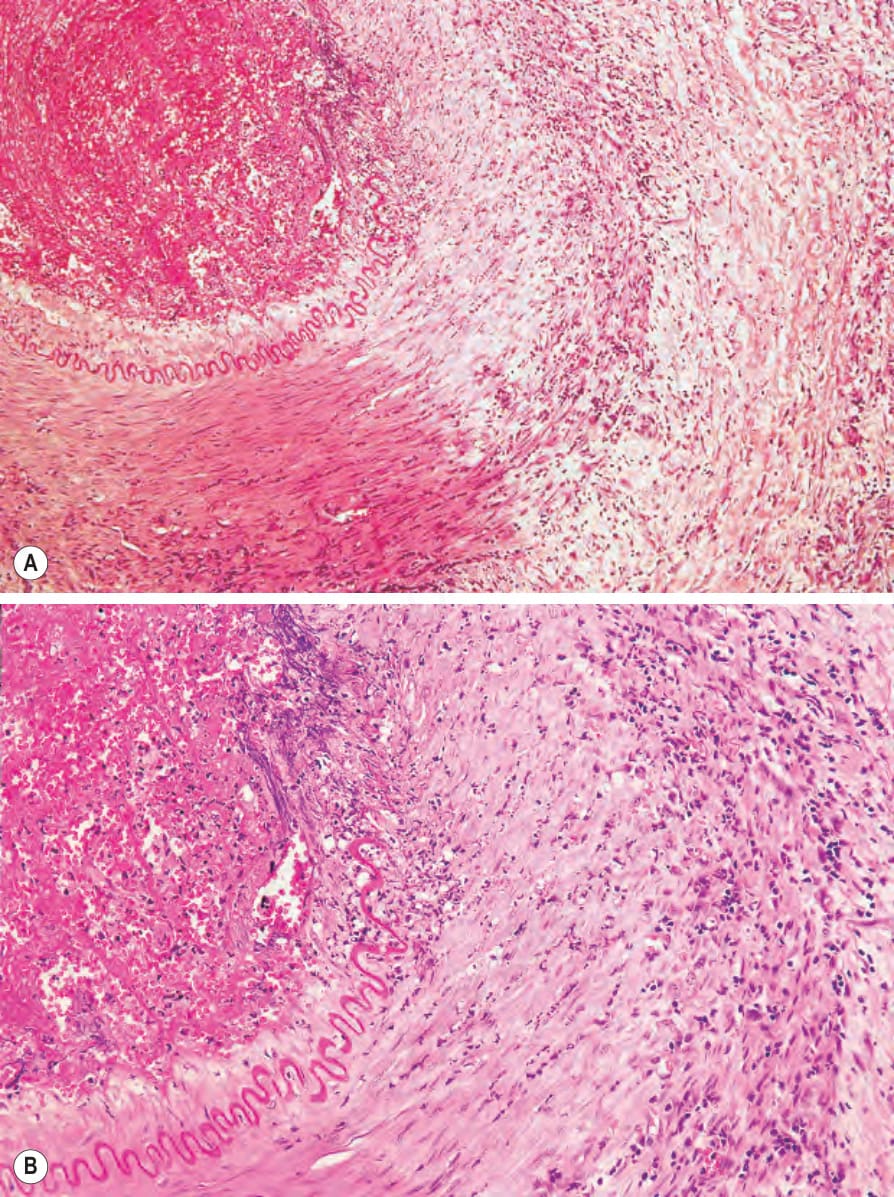
Fig. 16.90 (A, B) Thromboangiitis obliterans: this acute lesion shows pan-mural inflammation with abscess formation and thrombosis.
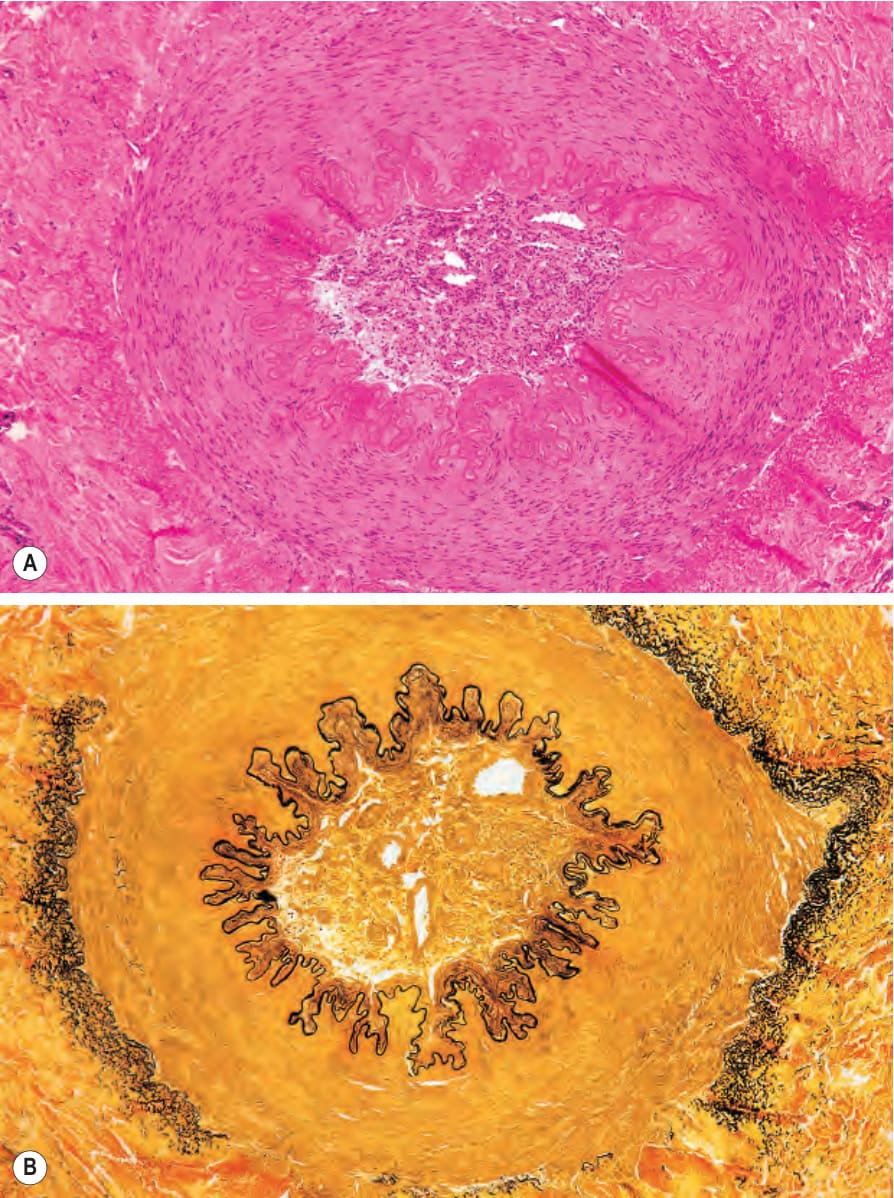
Fig. 16.91 (A, B) Thromboangiitis obliterans: old lesion showing luminal obliteration and recanalization. Note the intact elastic lamina.

Fig. 16.92 Giant cell arteritis: severe ischemic necrosis with ulceration has destroyed most of this patient’s scalp. By courtesy of D. McGibbon, MD, St Thomas’ Hospital, London, UK.
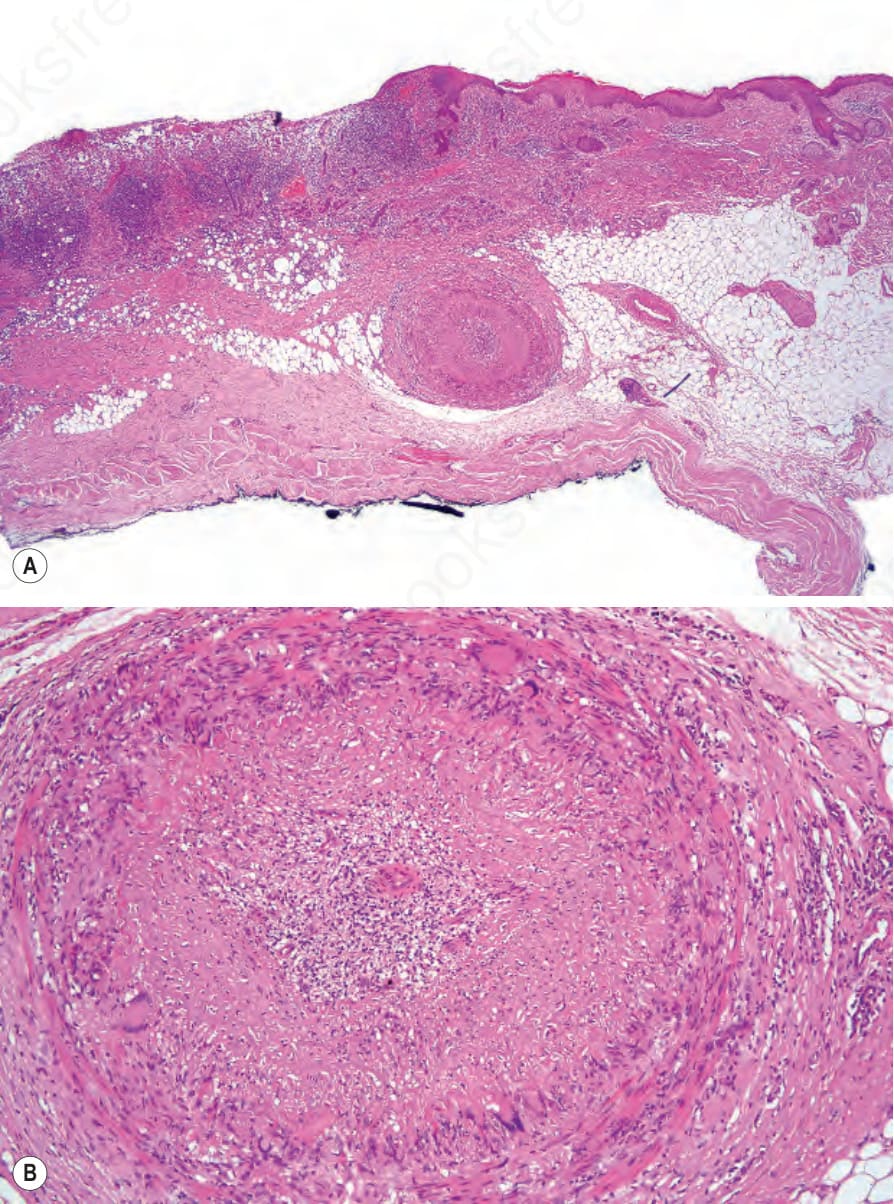
Fig. 16.93 (A, B) Giant cell arteritis: this scalp biopsy showed multiple affected vessels. By courtesy of P.A. Burton, MD, Southmead Hospital, Bristol, UK.
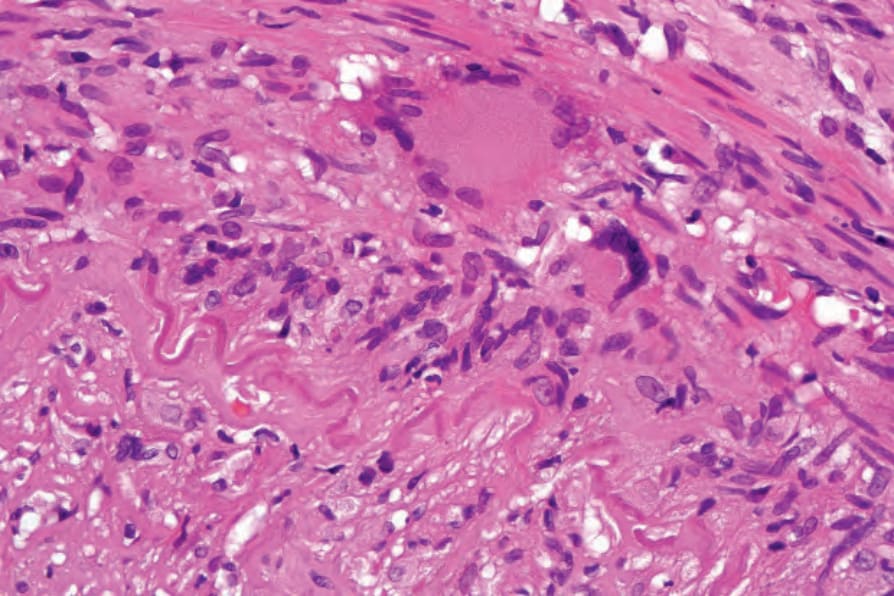
Fig. 16.94 Giant cell arteritis: the intima and media are infiltrated by a dense chronic inflammatory cell infiltrate containing conspicuous Langhans giant cells. By courtesy of P.A. Burton, MD, Southmead Hospital, Bristol, UK.
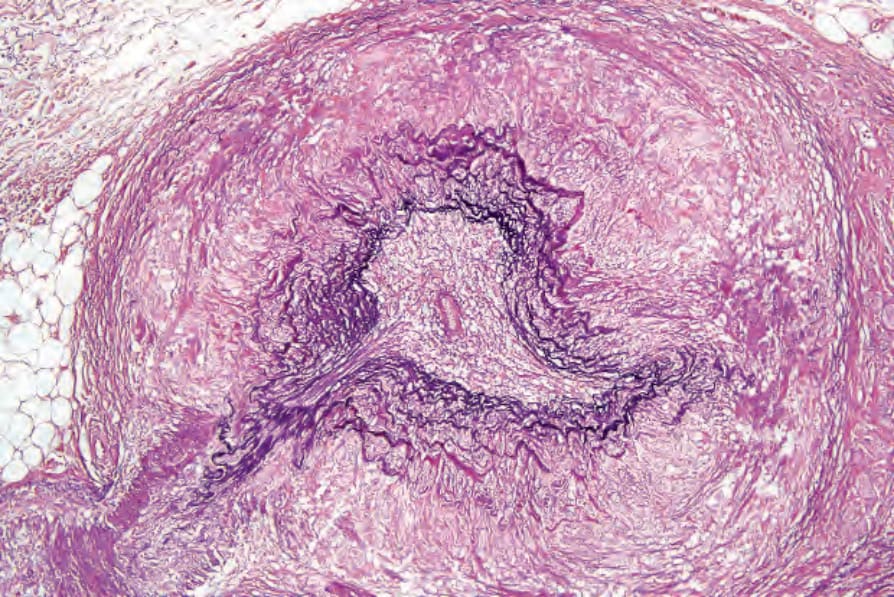
Fig. 16.95 Giant cell arteritis: there is fragmentation of the internal elastic lamina. By courtesy of P.A. Burton, MD, Southmead Hospital, Bristol, UK.
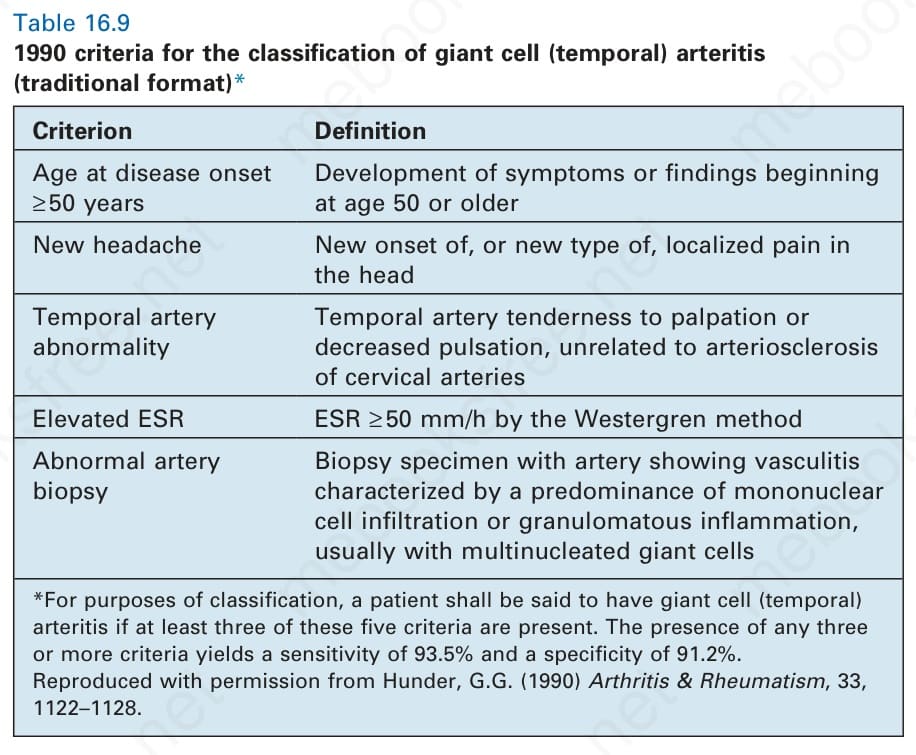
Table 16.9 1990 criteria for the classification of giant cell (temporal) arteritis (traditional format)*