Thromboangiitis obliterans
Thromboangiitis obliterans
Clinical features Thromboangiitis obliterans (Buerger disease) is most often seen in young adults and is much more common in males than in females.1 However, the ratio of men to women is shifting, with the disease becoming more common in women.2,3 In one large study, 23% of patients were female.2 In addition, the disease is seen more frequently in older patients.2 Buerger disease occurs almost exclusively in smokers. Although most patients are considered ‘heavy’ smokers, some smoke less than a pack of cigarettes a day.4 In fact, some authors view a history of smoking a necessary criterion for diagnosis. In one study from Japan, nonsmokers with Buerger disease were more likely to be women.5 In Bangladesh, smoking bidis (a hand-rolled, additive-free, unprocessed form of tobacco) is particularly associated with this disease.6
Injury to endothelial cells may play an initiating role. Endothelial cells in lesional tissue have increased expression of adhesion molecules VCAM-1, ICAM-1, and E-selectin, which allows for attachment of inflammatory cells and triggering the inflammatory response.24
Thromboangiitis obliterans patients also have higher levels of TNF-α, IL-1β, IL-4, IL-17, and IL-23 compared with matched controls.24 This could contribute to a proinflammatory and autoimmunity environment.
Lesions are characterized by thrombosis of small or medium-sized arteries and, less commonly, veins associated with a variable inflammatory infiltrate composed of a mixture of neutrophils, lymphocytes, eosinophils, histiocytes, and giant cells.19,25 Immunohistochemical studies have confirmed the heterogeneous nature of the infiltrate. T cells, B cells, macrophages, and dendritic cells may all be present.23 CD4-positive T cells outnumber CD8-positive cells and T-cell-mediated inflammation appears to be of significance in the development of the disease.24,26 A characteristic finding is the presence of a microabscess associated with an intraluminal thrombus. Inflammatory cells may be seen in all layers of the vessel wall (Fig. 16.90). Preservation of the internal elastic lamina is a typical feature.19
The worldwide incidence of Buerger disease differs dramatically from region to region. For example, the incidence is 50-fold greater in Nepal compared with North America.7 This disease has its highest prevalence in Eastern Europe, the Middle East, and Asia. Patients most often present with painful cyanotic lesions of the extremities, especially the fingers or toes, which may ulcerate and become gangrenous (Fig. 16.89). Sensitivity to cold is a common complaint.
Resolution of disease usually follows cessation of smoking.8,9 Patients who continue to smoke suffer autoamputation of digits and distal extremities. In one study, only 2% of patients who quit smoking had amputations. In contrast, 42% of those that continued to smoke required amputation.2
In most patients, the disease is limited to the extremities; however, some patients develop visceral involvement,10–13 and this can prove fatal.10 The vessels of the brain, intestine, heart, kidney, and lung may therefore be affected.14–17 Occasional patients have involvement of multiple organs.18
As lesions age, thrombi become organized and are replaced by fibrosis, and eventually the vessel is recanalized (Fig. 16.91). A definitive diagnosis based on biopsy findings is not possible during the later stages of organization.
Differential diagnosis The histopathological features are probably not specific for thromboangiitis obliterans (Buerger disease), and differential diagnosis includes other thrombotic vasculopathies. Clinical correlation is advised before rendering a definitive diagnosis. Preservation of the internal elastic lamina is a characteristic feature and is said to help in distinction from other vasculitides.19,27

Fig. 16.89 Thromboangiitis obliterans: digital gangrene is present in this amputation specimen.
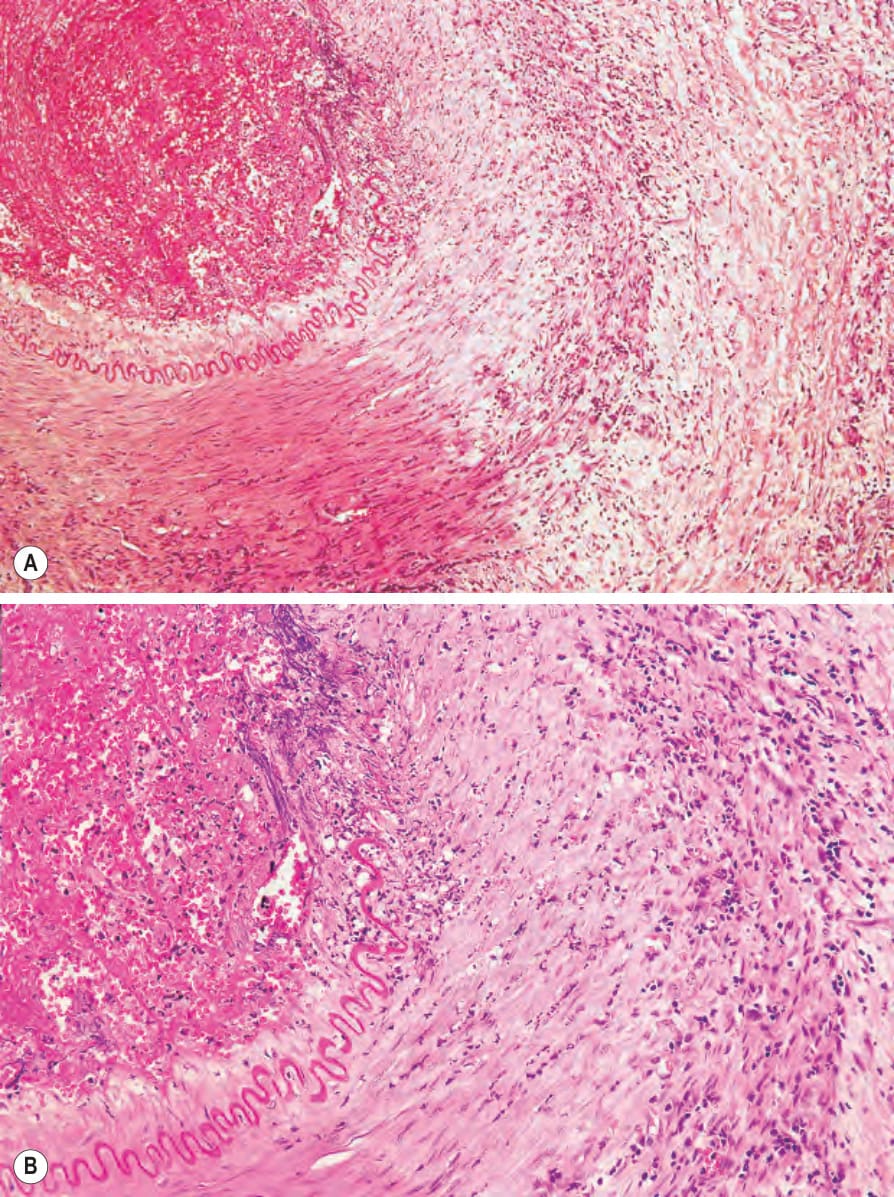
Fig. 16.90 (A, B) Thromboangiitis obliterans: this acute lesion shows pan-mural inflammation with abscess formation and thrombosis.
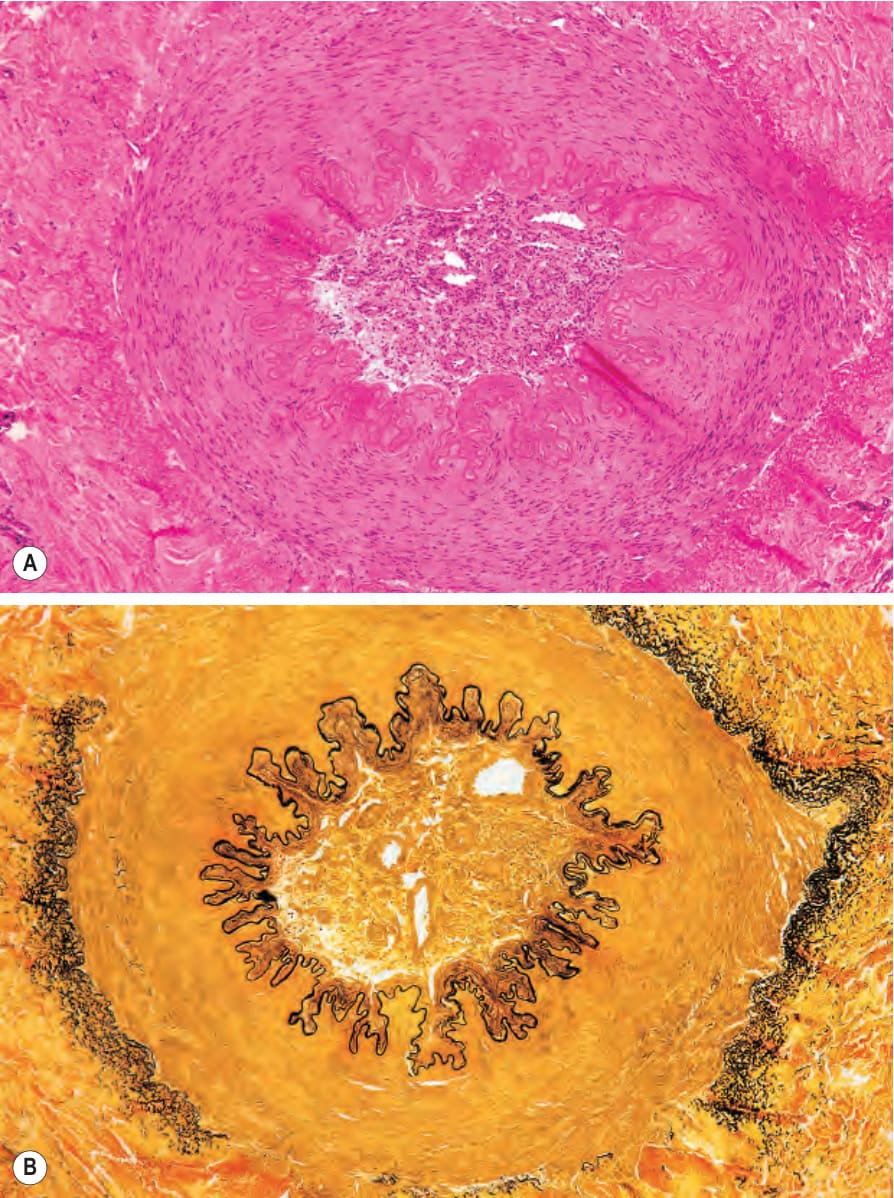
Fig. 16.91 (A, B) Thromboangiitis obliterans: old lesion showing luminal obliteration and recanalization. Note the intact elastic lamina.