Behçet disease
Behçet disease
Clinical features This rare disease was originally described as a combination of recurrent oral and genital ulceration associated with uveitis. However, it is now known to represent a systemic illness with lesions involving the joints and central nervous, vascular, respiratory, gastrointestinal, and urogenital systems, in
addition to mucous membranes and integument (Table 16.7).1–13 Although it is seen worldwide, it has a high incidence in Japan, Southeast Asia, the Middle East, Turkey, and some countries bordering the Mediterranean. Behçet disease shows a male predominance and most commonly presents in young adults with a peak incidence of onset in the third decade.14 Children may also be affected with an approximately equal sex incidence.15 One study has suggested that the disease is less aggressive in children.16 Some data appear to indicate that males have a higher mortality rate.17
The International Study Group established diagnostic criteria for Behçet disease in 1990 and these are summarized in Table 16.8.4 It should be kept in mind that these criteria are somewhat controversial.18 More research is necessary before we can fully understand this complex disease.
Recurrent oral ulceration is an invariable feature. Some patients have a long history of oral ulceration before developing other features that allow for a definitive diagnosis of Behçet disease. Ulcers typically measure up to 1 cm across but may be larger. They develop anywhere in the oral cavity,
744 Vascular diseases
Sign or symptom Incidence (%)
Oral ulcers 90–100
Genital ulcers 64–88
Ocular lesions 27–90
Cutaneous lesions 48–88
Joint manifestations 18–64
in the pharynx, and even in the larynx (Fig. 16.81).19 They are exquisitely painful, and usually regress spontaneously within 14 days although they can persist for much longer. A yellow, necrotic crust covers the ulcer floor. Some patients develop ulcerations in a herpetiform configuration.20 Patients with larger ulcers tend to have greater severity of oral disease with more frequent relapses.20
Cutaneous lesions are common, recurrent, and comprise a wide variety of manifestations including erythema nodosum-like lesions, usually on the lower extremities.21,22 Patients may also develop acneiform papules and pustules, furuncles, pyoderma, and thrombophlebitis (Fig. 16.82). In one very large study, papulopustular lesions (followed by erythema nodosum-like nodules) were the most commonly encountered skin manifestation.7 Patients have also been described with Sweet syndrome-like features.23
Neurological features 10–29
Intestinal manifestations 0–59
Thrombophlebitis 10–37
Reproduced with permission from Arbesfield, S.J. and Kurban, A.K. (1988) Journal of the American Academy of Dermatology, 19, 767–779. Copyright © The American Academy of Dermatology, Inc.
Criterion Definition
Typical of Behçet disease, and an important diagnostic clue, is development of sterile pustules at sites of mild skin trauma such as injection sites (pathergic response) (Fig. 16.83).24,25 Paradoxically, some authors have found that wound healing after 4 mm punch biopsy does not seem to differ compared with control subjects.26
Genital lesions, similar in appearance to those of the oral mucosa, occur on the scrotum, penis, vagina, and vulva (Figs 16.84 and 16.85).7
Recurrent oral ulceration
Minor aphthous, major aphthous, or herpetiform ulceration observed by physician or patient, and recurrent at least three times in one 12-month period
Plus two of:
Recurrent genital ulceration
Aphthous ulceration or scarring, observed by physician or patient
Eye lesions Anterior uveitis, posterior uveitis, or cells in vitreous on slit lamp examination or Retinal vasculitis observed by ophthalmologist
Skin lesions Erythema nodosum observed by physician or patient, pseudofolliculitis or papulopustular lesions; or acneiform nodules observed by physician, patient not on corticosteroid treatment
Positive pathergy test
Read by physician at 24–48 hours
*Findings applicable only in the absence of other clinical explanations. Reprinted with permission from Elsevier (International Study Group for Behçet’s Disease (1990) Lancet, 335, 1078–1080).
745 Behçet disease
is associated with a more severe clinical course in males, potentially leading to loss of vision.28 Conjunctivitis, corneal ulceration, choroiditis, and retinal vessel involvement (arterial and venous vasculitis) are sometimes additional features.
Joint involvement is not uncommon and usually affects the knees, ankles, elbows, and wrists.29 A mono- or oligoarticular pattern is typical. The affected joints are swollen, red, tender, and painful. It is of interest that despite many years of arthritic symptoms, joint deformities do not develop.
Vascular disease in Behçet disease takes the form of both thrombo-occlusive disease and frank vasculitis. Vascular involvement is an important cause of both morbidity and mortality and is seen in approximately one-third of patients.30,31 Males appear to be at an increased risk.31 Thrombophlebitis is common and can affect both superficial and deep veins of the limbs. Superior and inferior vena caval obstruction are not uncommon complications. A particularly perilous form of vascular involvement is hepatic vein occlusion (Budd-Chiari syndrome), which is associated with a high mortality.13,32 Pulmonary artery aneurysm occurs in approximately 1% of patients and is associated with a 50% mortality rate.33,34
The inflammation may affect virtually any artery and the development of an aneurysm with subsequent rupture is an important cause of death.
Respiratory involvement presents as dyspnea, cough, pleuritic chest pain, and hemoptysis.36 The last, due to pulmonary artery–bronchial fistula formation, is an important cause of death. Lung involvement occurs in up to 5% of patients.35
Intestinal involvement particularly affects the ileocecal region; ulcers may be complicated by perforation, presenting as an intra-abdominal emergency necessitating surgical intervention.36–38 Interestingly, one group has reported seasonal variation in Behçet disease flares suggesting an exogenous component or trigger.39 The esophagus is uncommonly affected by ulcers and erosion, stenosis or esophagitis.40
Involvement of the nervous system, which is associated with a poor prognosis, occurs in up to 25% of patients.12,41 Lesions develop anywhere in the central and peripheral components and, therefore, virtually any neurological sign or symptom may be seen, including sensory losses, strokes, and spinal cord, cranial and peripheral nerve lesions. Dural sinus thrombosis is a well-recognized complication.41
The kidney is affected in up to 55% of patients and manifestations include amyloidosis, glomerulonephritis, interstitial nephritis, vasculitis, and IgA nephropathy.42–46
A study of relative organ system involvement has led to a subclassification of a spectrum of Behçet disease.47,48 The mortality of Behçet disease is, however, surprisingly low, of the order of 2% to 4%.
Pathogenesis and histologic features Although the precise etiology and pathogenesis are unknown. It is likely that there is an altered immune response in patients with Behçet disease. It has been suggested that heat shock proteins may play an important role in its pathogenesis.49,50 They have been found to be elevated in serum together with increased levels of vascular endothelial growth factor (VEGF) and antiphospholipid antibodies independent of disease activity.51 Heat shock proteins reactive in Behçet patients induce uveitis in rats.50 Increased VEGF levels correlate significantly with the presence of vascular or ocular disease.51 Oligoclonal expansion of T cells in some patients with Behçet disease has been documented.52 In one study, serum IL-12 and peripheral Th1 lymphocyte levels correlated with disease activity.53
Ocular involvement is important because, if left untreated, it may progress to cataracts and blindness. Both eyes are affected in the majority of patients. Almost any part of the eye is affected and bilateral inflammation of the anterior segment (anterior uveitis), posterior uveitis with hypopyon, and vitreitis are said to be pathognomonic.27,28 Uveitis is more common and
The increased peripheral Th1 lymphocyte levels would seem to correlate with molecular findings. Genome wide association studies have identified associations with the IL23R-IL12RB2, IL10, STAT4, CCR1-CCR3, KLRC4, ERAP1, TNFAIP3, and FUT2 loci. These genes are associated with polarization toward a Th1 phenotype.54
Complement components C3 and C9 have been identified in blood vessel walls in oral biopsies.48 Increased interleukin levels associated with increased B-cell activity have also been described.55 Of possible importance in the pathogenesis is the frequent presence of high levels of circulating immune complexes and the common detection of immunoglobulins (particularly IgM) and complement in blood vessel walls.56–58 Behçet disease is associated with human leukocyte antigen (HLA)-B5, -B12, -B15, -B27,
746 Vascular diseases
A
B
-A26, and particularly with HLA-BW51.30,54 Anticardiolipin antibodies have been described.30
Despite the accumulation of considerable immunological and genetic data, the underlying antigen or other stimulus that drives these changes, and is ultimately responsible for the disease, remains elusive.
The histologic features are in themselves largely non-specific.48,55,59,60 The diagnosis of Behçet disease is essentially clinical. The pathological features that may be detected include both lymphocytic and necrotizing vasculitis affecting the superficial postcapillary venules with associated fibrinoid necrosis (Fig. 16.86).59 In one study, nearly 50% of patients had evidence of vasculitis.61 Often, however, such vasculitic changes appear to be a consequence, rather than a cause, of the dermal or mucosal inflammatory changes.60 Endothelial swelling may be a feature and there is often an associated lymphocytic perivascular infiltrate, although sometimes neutrophils are abundant.62 Venulitis and phlebitis were the most common forms of vasculitis seen in one series of patients.18 In this study, phlebitis/venulitis was seen in 48% of patients while leukocytoclastic vasculitis and lymphocytic vasculitis were seen in 17% and 31% of patients, respectively.61
a neutrophilic infiltrate with intraepidermal pustules. Vasculitis was not seen in pathergic lesions in this study.65 Other authors have found that the pathergic lesions may show leukocytoclastic vasculitis or Sweet syndrome-like features.24

Fig. 16.81 Behçet disease: superficial ulcers are present on the inner aspect of both lips. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 16.82 Behçet disease: typical pustules on the lower leg. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 16.83 Behçet disease: this ruptured pustule developed at the site of a previous venipuncture. Such a positive provocation test is virtually pathognomonic for Behçet disease. By courtesy of D.A.H. Yates, MD, St Thomas’ Hospital, London, UK.

Fig. 16.84 Behçet disease: there is a typical scrotal ulcer with central slough. By courtesy of D.A.H. Yates, MD, St Thomas’ Hospital, London, UK.

Fig. 16.85 Behçet disease: multiple superficial vulval ulcers are present. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
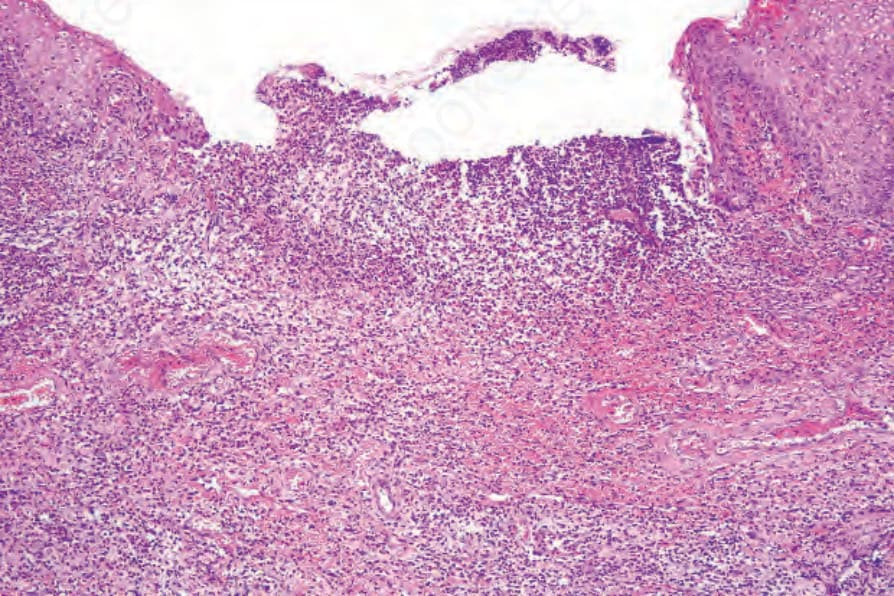
Fig. 16.86 Behçet disease: this field shows a superficial vulval ulcer with an intense neutrophilic infiltrate and changes of acute vasculitis.
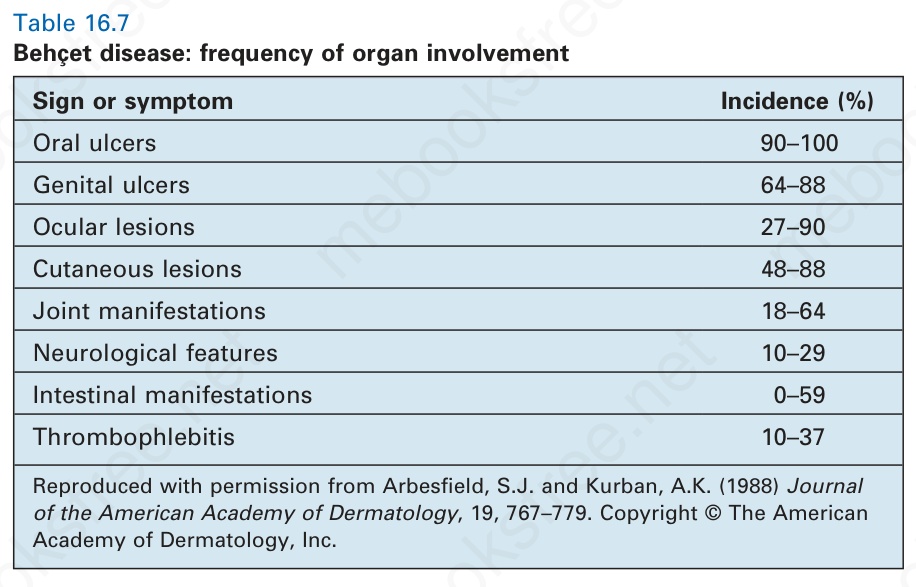
Table 16.7 Behçet disease: frequency of organ involvement
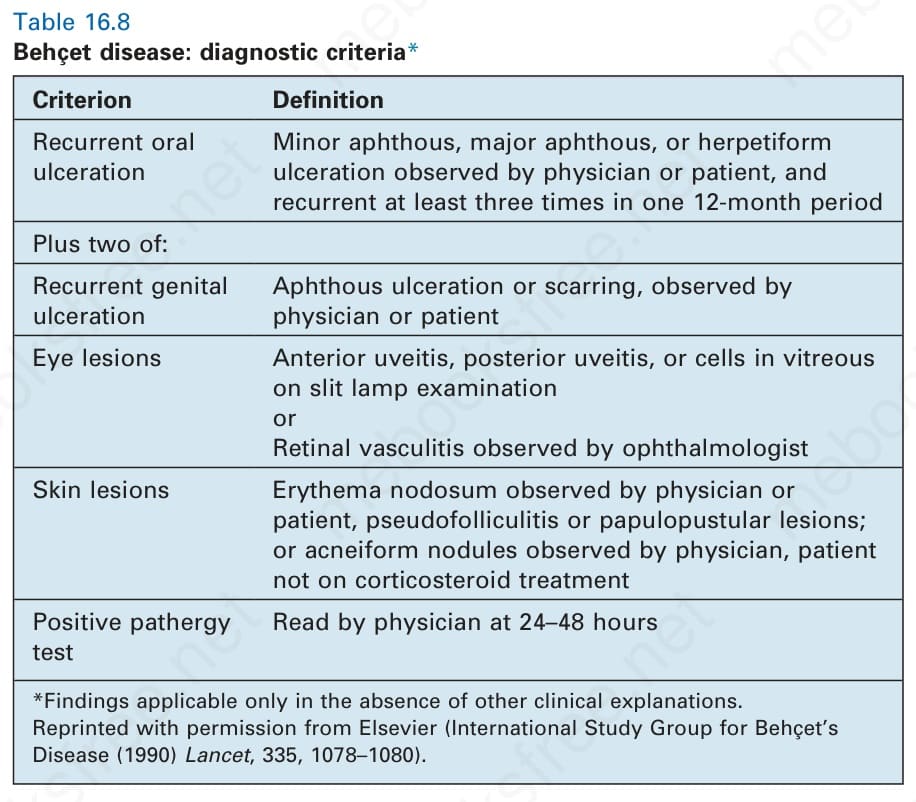
Table 16.8 Behçet disease: diagnostic criteria*
The erythema nodosum-like lesions correspond to necrotizing vasculitis of the subcutaneous vessels, usually associated with thrombosis. Septal and lobular panniculitis have also been described.19 Superficial thrombophlebitis is present in up to 30% of patients (Fig. 16.88).47 Oral lesions and genital ulcers show non-specific ulceration, accompanied in some instances by leukocytoclastic or lymphocytic vasculitis.
Non-specific features include a diffuse neutrophil polymorph dermal infiltrate with or without abscess formation, corresponding clinically to pustular lesions, acute folliculitis, and acneiform folliculocentric pustular changes (Fig. 16.87).18,63,64 Biopsy after needle trauma in one study showed
Pulmonary involvement is characterized by pulmonary artery vasculitis, sometimes also affecting the veins and capillaries.35 Thrombosis, infarction, hemorrhage, and the development of aneurysm are important sequelae. The inflammation is usually transmural and may be associated with damage to the associated elastic tissue. Older destructive vascular lesions are characterized by fibrous scarring.
Cerebral lesions in the early stage are characterized by a perivenular lymphocytic infiltrate. In the more advanced lesions there is extensive demyelination resembling multiple sclerosis.30
Differential diagnosis Given the myriad non-specific histologic manifestations that Behçet disease may produce, it comes as no surprise that the histologic differential diagnosis is usually broad. The authors of one large study stated that clinical data are most important in establishing a diagnosis and suggested that the role
of biopsy is to confirm the clinical impression.7 Others propose that biopsy is critical to evaluate for vessel-based pathology as clinical distinction from pustular (non-vascular) lesions may be important.18 It is likely that the criteria for diagnosis of Behçet disease will continue to be refined.
The differential diagnosis includes other causes of folliculitis, infection, erythema nodosum, connective tissue disease, neutrophilic and lymphocytic vasculitis, and neutrophilic dermatoses. There are no pathognomonic histologic changes. Both clinical and pathological data must be considered before arriving at a final diagnosis.7
747 Giant cell arteritis (temporal arteritis)
Pathogenesis and histologic features The pathogenesis of thromboangiitis obliterans is poorly understood. Clearly, the strong association with smoking suggests that this habit plays an important role in eliciting thrombosis and resultant ischemia.19 It is unclear if tobacco products are toxic to endothelial cells or elicit immune reactions that damage vessels. Of interest, the disease has been described in patients who use smokeless tobacco.20 Antiendothelial antibodies are elevated in a subset of patients with Buerger disease.21 Furthermore, disease activity correlates with antiendothelial cell antibody titers.21 Response to acetylcholine, an endothelium-dependent vasodilator, is diminished in ‘nondiseased’ extremities of thromboangiitis obliterans patients compared with control subjects.22 IgG, IgM, and IgA are present along the internal elastic lamina.23
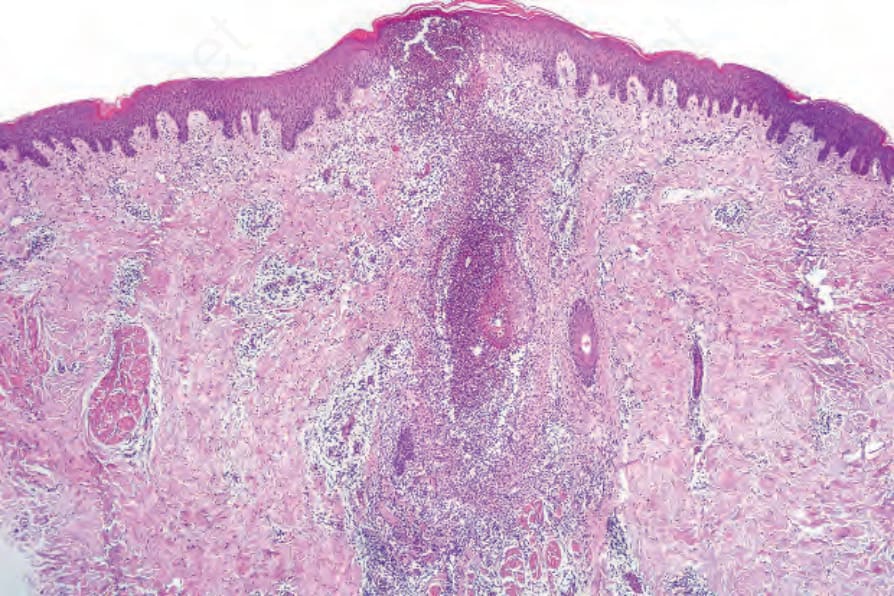
Fig. 16.87 Behçet disease: there is florid suppurative acute folliculitis.
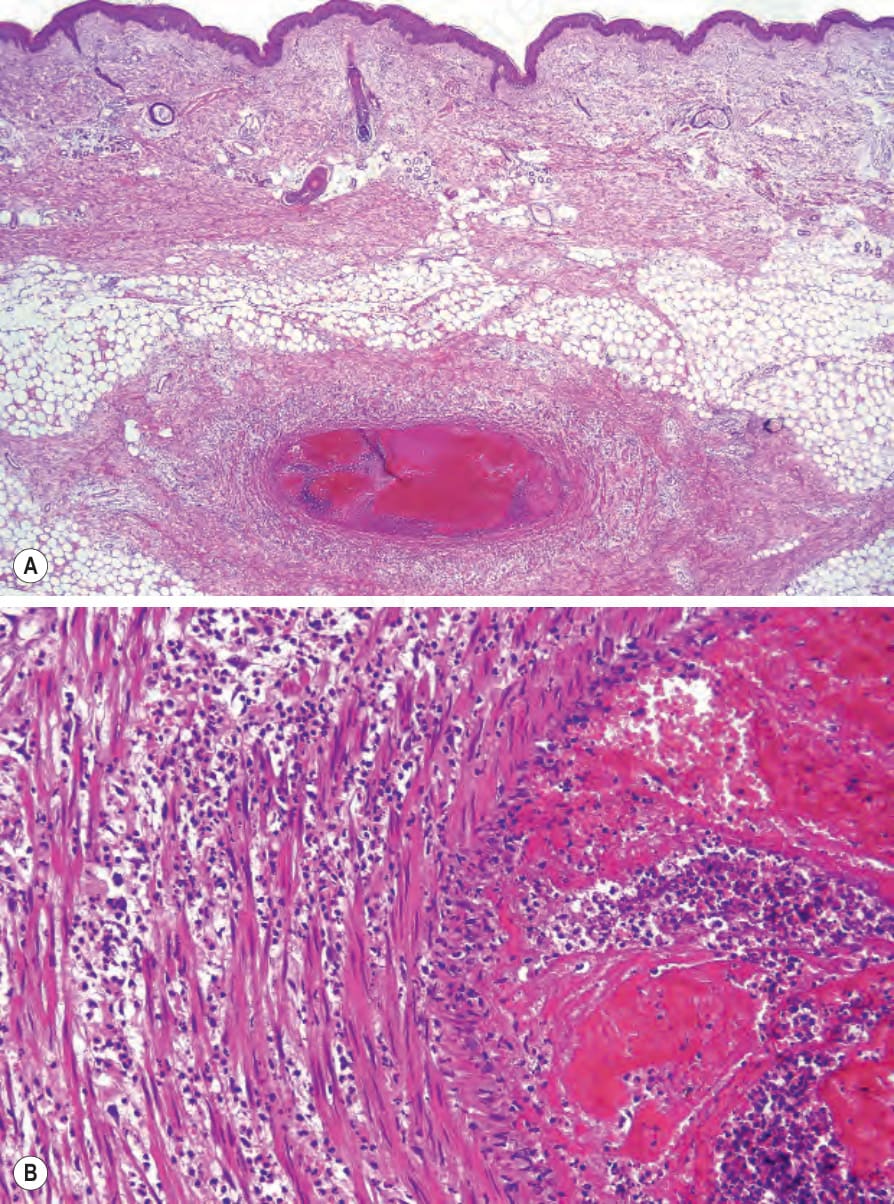
Fig. 16.88 (A, B) Behçet disease: this section shows thrombophlebitis involving a vein in the subcutaneous fat. The vessel is infiltrated by large numbers of lymphocytes.