Erythema elevatum diutinum
Erythema elevatum diutinum
Clinical features This uncommon disease represents a localized variant of leukocytoclastic vasculitis.1–3 Although it can occur in any age group, patients are usually in their third to fifth decade.4 Incidence is equal in men and women. Patients present with papules and nodules measuring up to about 1 cm in diameter; they may also develop round or oval, indurated, elevated plaques 5–6 cm in diameter. Lesions are red or purple, although some have a yellowish tinge, which may be confused with a xanthomatous process. Bullous lesions are occasionally present and an annular distribution has been reported.1,5,6 The disease is characteristically persistent and the distribution of the lesions often symmetrical. Large nodules resembling keloids or tumors are sometimes found.7,8
An ultrastructural study of a case of granuloma faciale has shown that the cytoplasmic granules in the eosinophils display alterations and Langerhans cells are absent.32
Differential diagnosis The morphological features of granuloma faciale are distinctive. The presence of a mixed infiltrate with a grenz zone distinguishes it from neutrophilic dermatoses and leukocytoclastic vasculitis. Erythema elevatum diutinum, another form of localized vasculitis, tends to be located on the extensor surfaces of the extremities and shows more sclerosis, more neutrophils, and fewer eosinophils. The presence of large numbers of eosinophils may
Lesions are located particularly in relation to the extensor surfaces of the joints and are, therefore, seen on the backs of the hands and fingers, wrists, elbows, knees, ankles, and toes (Figs 16.76 and 16.77). The buttocks may also be affected, but the trunk is usually spared.9 We have observed a case with oral involvement. Although lesions are often asymptomatic, some patients complain of itching and pain, and symptoms are frequently made worse in a cold environment. Patients sometimes also have arthralgia. Eye involvement includes keratolysis and ulcerative keratitis with positive rheumatoid factor.10–13 Although the disease is chronic and progressive, resolution usually occurs by 5–10 years. The disease characteristically responds to dapsone.
742 Vascular diseases
Inflammatory bowel disease – both Crohn disease and ulcerative colitis – has also been associated with erythema elevatum diutinum.29–31 Interestingly, in one patient with Crohn disease, skin lesions seemed to appear during exacerbation of bowel symptoms.29 In another patient with ulcerative colitis, onset of erythema elevatum diutinum lesions coincided with presentation of bowel disease, and skin lesions resolved following colectomy.30 Erythema elevatum diutinum has also been reported in association with celiac disease.32–34 In one patient with celiac disease, skin lesions resolved with the introduction of a gluten-free diet.33
Rheumatoid arthritis has been described in conjunction with erythema elevatum diutinum.35–37 Other reported associations include granulomatosis with polyangiitis, relapsing polychondritis, pyoderma gangrenosum, Sweet syndrome, cutaneous lupus erythematosus, nodular scleritis and panuveitis, Hashimoto thyroiditis, juvenile idiopathic arthritis, Sjögren syndrome, dermatomyositis, and dermatitis herpetiformis.38–50 Erythema elevatum diutinum is also seen in patients with HIV infection.51–56 In HIV-infected patients, lesions may mimic Kaposi sarcoma.51,57 Extensive acro-osteolysis has been described in a single case.58 The exceptional association with pityriasis rubra pilaris and mosquito bites is probably coincidental.59
Although it has been suggested that a condition described as ‘neutrophilic dermatosis of the dorsal hands’ may be part of the spectrum of erythema elevatum diutinum, it is more likely to represent a variant of Sweet syndrome.60
Pathogenesis and histologic features Erythema elevatum diutinum is possibly immune complex mediated. Both a streptococcal antigen and E. coli have been implicated.2,61 As mentioned above, the disease has also been recorded in association with cryoglobulin IgA, monoclonal or biclonal gammopathy, multiple myeloma, hairy cell leukemia, and polycythemia rubra vera.1,62–64 In addition, IgA ANCA and less frequently IgG ANCA have been identified in patient’s serum.65 In early lesions, there is increased expression of the beta (2)-integrins CR3 and LFA-1 and this diminishes in older lesions.66 Peripheral blood neutrophils show increased migration in response to interleukin-8 (IL-8) and decreased responsiveness to the bacterial peptide analog N-formyl-methionyl-leucyl-phenylalanine. These findings suggest that in erythema elevatum diutinum the recruitment of neutrophils occurs as a result of activation of cytokines such as IL-8.66 Immune complexes and bacterial peptides sustain the persistent local inflammatory response.66 There appears to be no association with IgG4-related diseases.67,68
Biopsy of early lesions reveals typical features of leukocytoclastic vasculitis (Fig. 16.78).1,69 The epidermis may show acanthosis and parakeratosis. Fibrinoid necrosis and infiltration of the superficial vessels by neutrophil polymorphs are present. The perivenular connective tissue contains abundant fibrin and a dense inflammatory cell infiltrate of neutrophils, histiocytes, lymphocytes, and eosinophils. Leukocytoclasis is usually evident.
Older lesions are characterized by the development of granulation tissue and fibrous scarring, although even then, foci of neutrophilic vasculitis may be found after examination of multiple sections (Fig. 16.79). In ‘burnt out’ lesions, vasculitis may not be present. Granulation tissue and dense scarring mark the site of the previous acute inflammatory process. In older lesions the scarring often shows a storiform pattern (Fig. 16.80). Interstitial lipid deposition described in the past as extracellular cholesterolosis is uncommon.
Systemic involvement does not usually occur but pulmonary infiltrates have exceptionally been documented.14
An association with paraproteinemia is frequently present, often of the IgA subtype.1,15–19 Hyperimmunoglobulinemia D syndrome is a further rare association.20 An underlying myelodysplastic syndrome or a hematological malignancy (e.g., multiple myeloma, B-cell lymphoma, and chronic lymphocytic leukemia) has been found in some patients.1,21–25 Often, the skin lesions precede development of the hematological disorder.1 In one study, an average of 7.8 years separated onset of skin lesions and development of a myeloproliferative disorder.1,26
Erythema elevatum diutinum has rarely also been associated with other malignancies such as pulmonary lymphoepithelioma-like carcinoma and breast carcinoma.27,28
In ocular lesions, leukocytoclastic vasculitis with focal granulomatous inflammation has been described.11
Rare histopathological features described include palisaded necrotizing granuloma and pyogenic granuloma-like features.59
Differential diagnosis Erythema elevatum diutinum typically involves the dermis and must, therefore, be distinguished from granuloma faciale. Granuloma faciale usually shows an eosinophil predominance whereas in erythema elevatum diutinum neutrophils are much more numerous. However, the histologic features of late lesions in both entities often overlap and similar appearances are found in chronic fibrosing vasculitis. The latter represents a non-specific reaction pattern that is occasionally seen in solitary lesions from patients who have no clinical features of either granuloma faciale or erythema elevatum
743 Behçet disease
A
B
diutinum.70 Distinction from Sweet syndrome is afforded by the presence of neutrophilic vasculitis. Older sclerotic lesions, particularly when they present as mass lesions, may be mistaken for a neoplastic process or dermatofibroma.8 The presence of a leukocytoclastic vasculitis and neutrophilic infiltrate with karyorrhexis favors erythema elevatum diutinum.
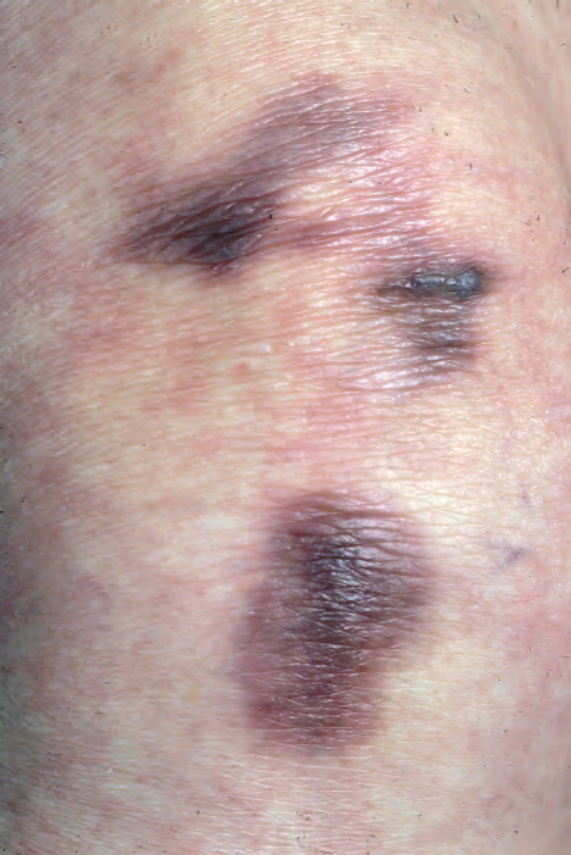
Fig. 16.76 Erythema elevatum diutinum: tuberose nodules present on the elbow. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 16.77 Erythema elevatum diutinum: the extensor surfaces are commonly affected. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
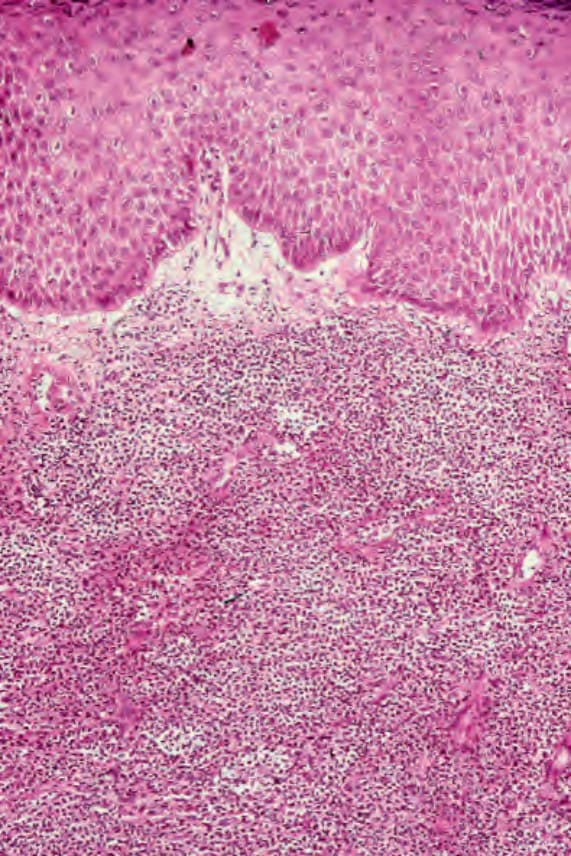
Fig. 16.78 Erythema elevatum diutinum: early lesion showing leukocytoclastic vasculitis in a background of a Sweet syndrome-like neutrophil infiltrate.
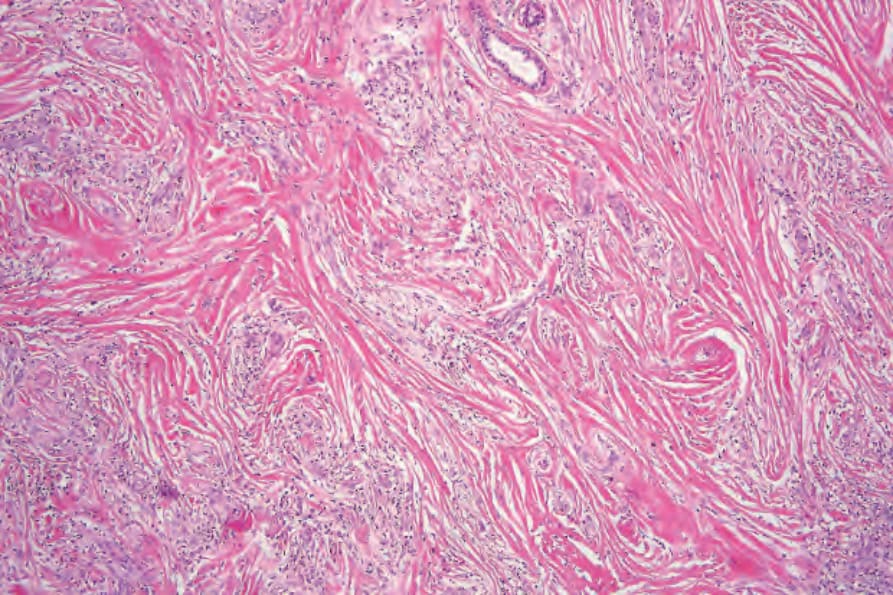
Fig. 16.79 Erythema elevatum diutinum: older lesion showing scar tissue with a vaguely storiform growth pattern.
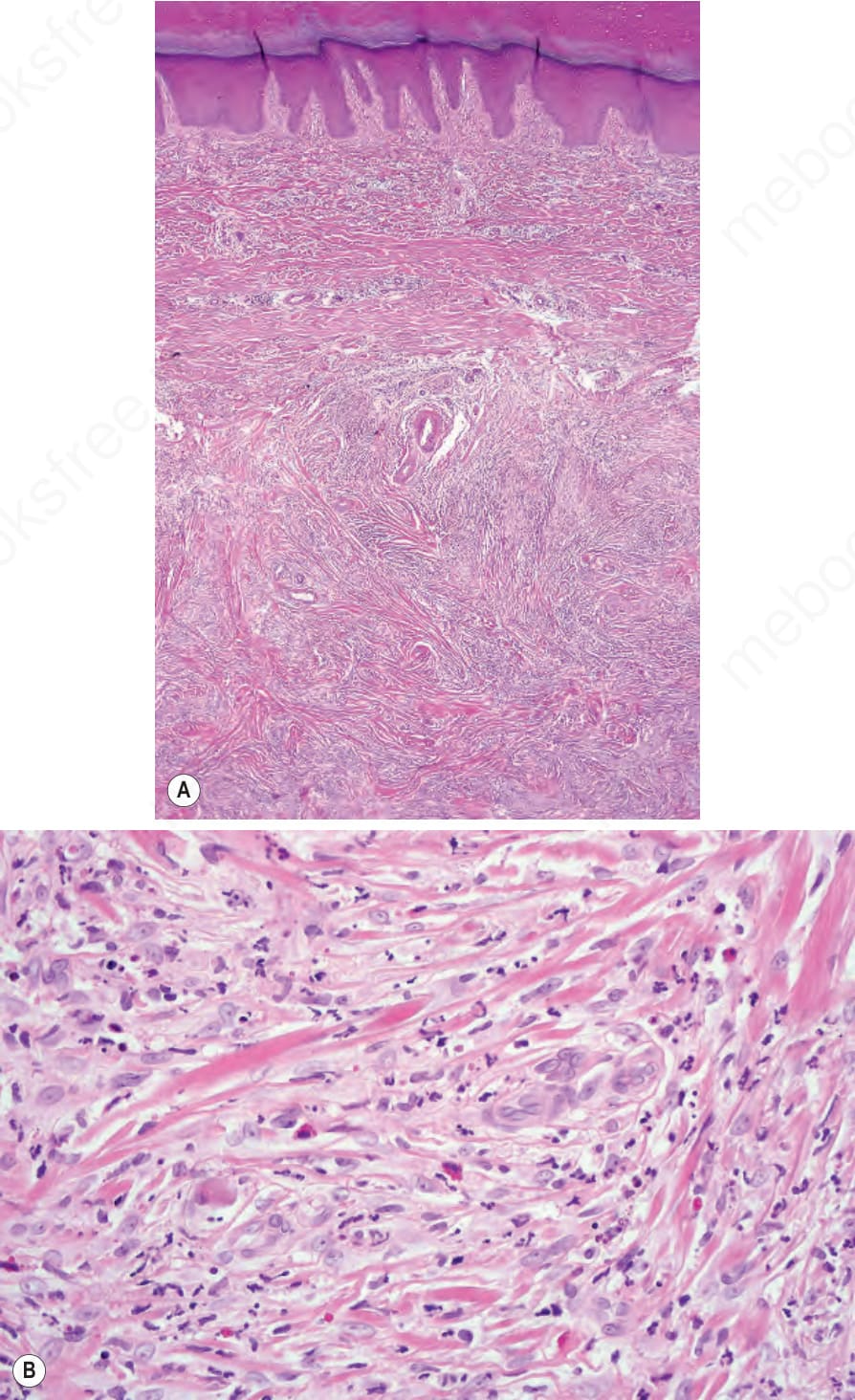
Fig. 16.80 (A, B) Erythema elevatum diutinum: this example was clinically thought to represent a keloid. There is a circumscribed dermal nodule composed of spindle cells in a hyalinized stroma. Focally perivascular nuclear debris is evident and there are scattered eosinophils.