Granuloma faciale
Granuloma faciale
Clinical features
Granuloma faciale is a localized form of leukocytoclastic vasculitis of uncertain pathogenesis. Although children may be affected, most cases occur in people who are middle aged or older, most commonly in men.1 Lesions occur most commonly on the face and are single or more often multiple, erythematous or brownish red, soft discrete papules, plaques or nodules up to several centimeters in diameter (Fig. 16.67).2–4 The surface often shows dilated follicles and fine telangiectasia (Fig. 16.68). Common sites include the nose, malar prominence, forehead, and ear (Fig. 16.69). A case simulating rhinophyma has been documented.5 Extrafacial lesions may occur
Of interest, there is a growing body of literature reporting Kawasaki disease, or a Kawasaki-like syndrome, in patients infected with the HIV.32–34
The histopathological features of cutaneous lesions in Kawasaki disease are often non-specific and comprise severe edema of the papillary dermis accompanied by vascular dilatation, endothelial cell swelling, and degeneration associated with a superficial perivascular mononuclear infiltrate.5 Immunopathological studies have shown the infiltrate is usually composed of CD4+ T lymphocytes and macrophages.35 Occasionally, however, the features of a leukocytoclastic vasculitis are evident (Fig. 16.66). The epidermis may show mild basal cell degeneration.5 Vesiculopustular lesions develop on the basis of subcorneal spongiform pustulation.10
Systemic lesions are characterized by necrotizing vasculitis.23,36,37 Aneurysm with mural thrombus formation may be evident in advanced lesions.
Lymph node involvement includes vasculitis, focal necrosis, and infarction.
Differential diagnosis The mucocutaneous manifestations of Kawasaki disease show considerable overlap with those seen in the toxic shock syndrome, which is not surprising, given that they appear to share a similar pathogenesis. Palmoplantar erythema, cutaneous desquamation, conjunctivitis, and pharyngitis are therefore common to both.38 Toxic shock syndrome (which has been linked to staphylococcal exotoxin complicating constant tampon use in menstruating females) is, however, not associated with systemic vascular involvement. Histologically, it is characterized by a mild, superficial, perivascular lymphocytic infiltrate associated with edema of the papillary dermis and no evidence of vasculitis.39
740 Vascular diseases
Pathogenesis and histologic features Examination of lesional biopsies by immunofluorescence reveals granular IgG and complement along the epidermal-dermal junction, outlining the hair follicles, and also within the walls of blood vessels; less often IgA and IgM are present, and there is abundant fibrin.23–25 Granuloma faciale is, therefore, a chronic vasculitis and may be immune complex mediated. However, some authors consider the above immunofluorescence findings non-specific. Immunohistochemistry shows the presence of abundant eosinophilic cationic protein.26 T-helper lymphocytes represent the main nonmyelocytic cell in the infiltrate and it has been suggested that they play a role in the pathogenesis of the disease, being attracted to the site by gamma-interferon.27
on the extremities, neck, chest, and scalp (Fig. 16.70).1,6–14 Although often asymptomatic, patients sometimes report symptoms of mild pruritus or stinging. There is no evidence of associated systemic involvement. Granuloma faciale tends to chronicity and is typified by periods of relapse and partial remissions. Treatment is very difficult and recurrences manifest after surgical excision, even at the site of full-thickness grafting.15
A histologically similar lesion affecting the mucosa of the upper respiratory tract has been designated ‘eosinophilic angiocentric fibrosis’. Concurrent cases of granuloma faciale and eosinophilic angiocentric fibrosis have been described.16–21 This suggests that the two diseases represent part of the same spectrum.
Granuloma faciale has been documented in a patient with prostate carcinoma.22 Any relationship with tumors is likely to be coincidental.
Some cases of granuloma faciale may be related to IgG4-associated sclerosing diseases. In one study, just over 20% of granuloma faciale cases met immunohistochemical criteria for IgG4 sclerosing diseases.28 In contrast, another large series demonstrated no evidence of IgG4-related disease, suggesting that the association may be less common.29
Histologically, granuloma faciale is characterized by a dense cellular infiltrate, which often has a nodular outline (Fig. 16.71).30 This infiltrate usually occupies the mid-dermis, although the deep dermis and the subcutaneous fat may be involved; it typically spares the immediate subepidermis and hair follicles, forming a ‘grenz zone’ (Fig. 16.72). The infiltrate is polymorphic, being composed of large numbers of eosinophils, neutrophils
741 Erythema elevatum diutinum
raise the possibility of a Langerhans cell proliferative disorder; however, the presence of only scattered Langerhans cells and a grenz zone (Langerhans cell proliferative disorders tend to be epidermotropic) with significant numbers of neutrophils favors granuloma faciale. The grenz zone also helps to distinguish granuloma faciale from hypersensitivity reactions, such as to an arthropod bite. Epithelioid hemangioma (angiolymphoid hyperplasia) is distinguished by the presence of a lobular proliferation of vessels lined by epithelioid endothelial cells. An exceptional case of infection by Trichophyton rubrum with histology mimicking that of granuloma faciale has been documented.33
Histologic features identical to those of granuloma faciale may be seen in patients presenting with a solitary lesion (papule, nodule, or plaque) that does not have the clinical appearance or location typical of the disease. The histologic picture in these cases has been described as chronic fibrosing vasculitis. As there is also histologic overlap with erythema elevatum diutinum, it has been suggested that the microscopic appearances represent a non-specific inflammatory reaction pattern.34 Therefore, establishing the diagnosis requires close clinicopathological correlation.
(often displaying leukocytoclasis), and an admixture of plasma cells, mast cells, and lymphocytes (Fig. 16.73).31 Red cell extravasation is often present. Blood vessels, which often appear increased in number, are dilated and may show infiltration of their walls by eosinophils with fibrin deposition (Fig. 16.74). Diagnostic features of vasculitis, namely inflammation of vessel walls associated with fibrinoid change, may be difficult to identify or absent in some lesions.6 In other cases, fibrin is widely distributed in the dermis. Older lesions may show fibrosis and hemosiderin deposition.1 The microscopic picture in late stages overlaps with that seen in erythema elevatum diutinum (Fig. 16.75).1
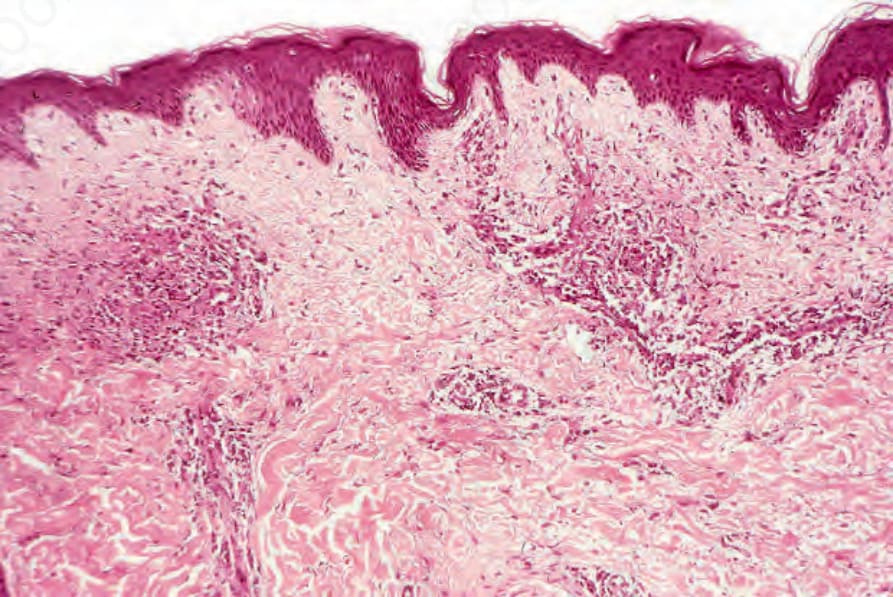
Fig. 16.66 Kawasaki disease: in this example, the features of severe, acute leukocytoclastic vasculitis are present in the superficial dermis. This is an uncommon finding. By courtesy of W.G. Phillips, MD, Institute of Dermatology, London, UK.

Fig. 16.67 Granuloma faciale: multiple brown nodules. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 16.68 Granuloma faciale: the face is a commonly affected site. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
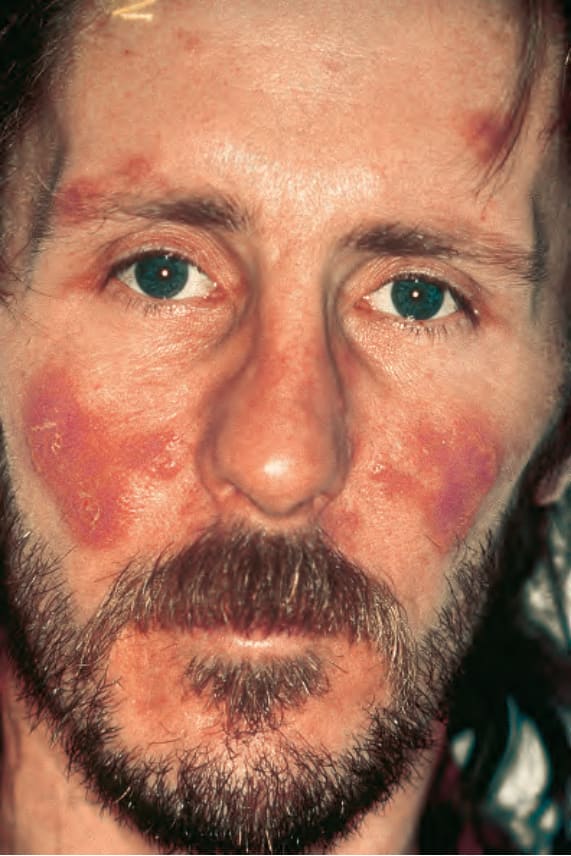
Fig. 16.69 Granuloma faciale: the lesions are frequently multiple. By courtesy of K. Liddell, MD, Eastbourne District Hospital, East Sussex, UK.

Fig. 16.70 Granuloma faciale: there are multiple lesions on this patient’s neck. By courtesy of the Institute of Dermatology, London, UK.
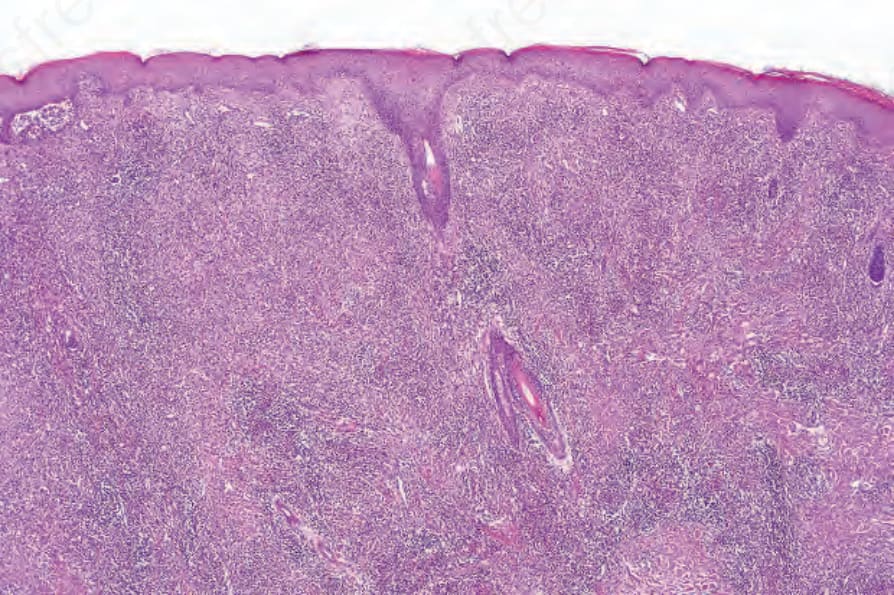
Fig. 16.71 Granuloma faciale: a dense inflammatory cell infiltrate is present in the dermis. Note the conspicuously spared grenz zone.
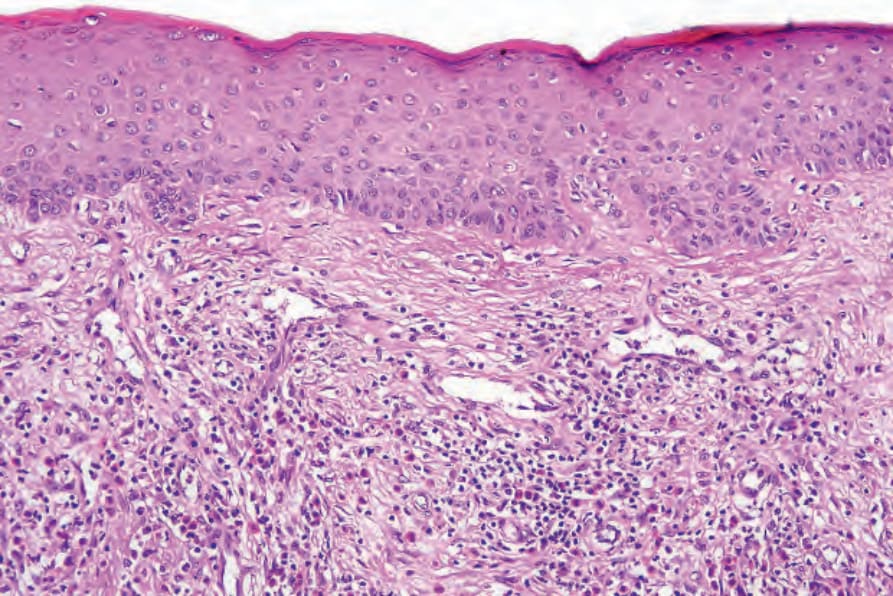
Fig. 16.72 Granuloma faciale: close-up view of grenz zone.
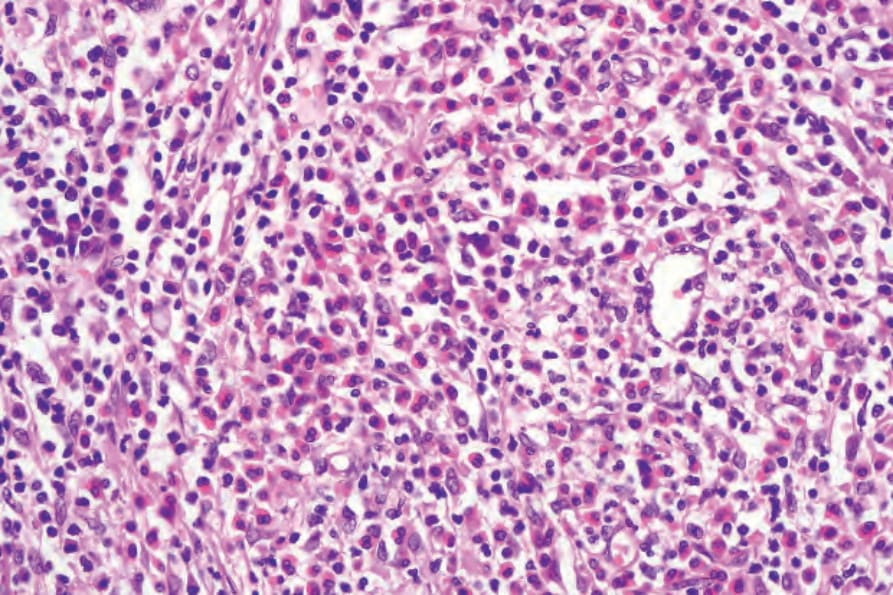
Fig. 16.73 Granuloma faciale: the infiltrate contains large numbers of eosinophils as well as lymphocytes, histiocytes, and occasional polymorphs and plasma cells.
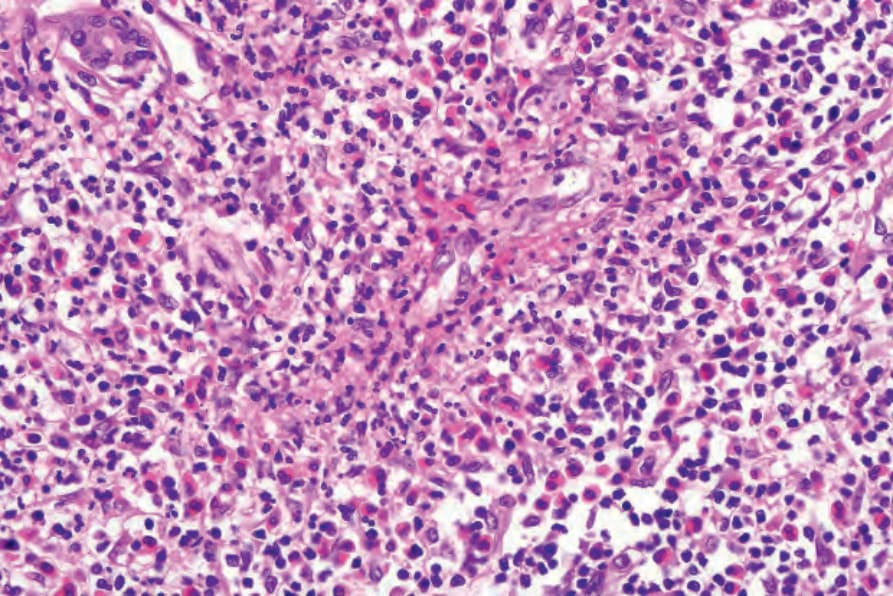
Fig. 16.74 Granuloma faciale: this dilated blood vessel shows marked endothelial swelling, fibrin deposition, and disruption of its wall.
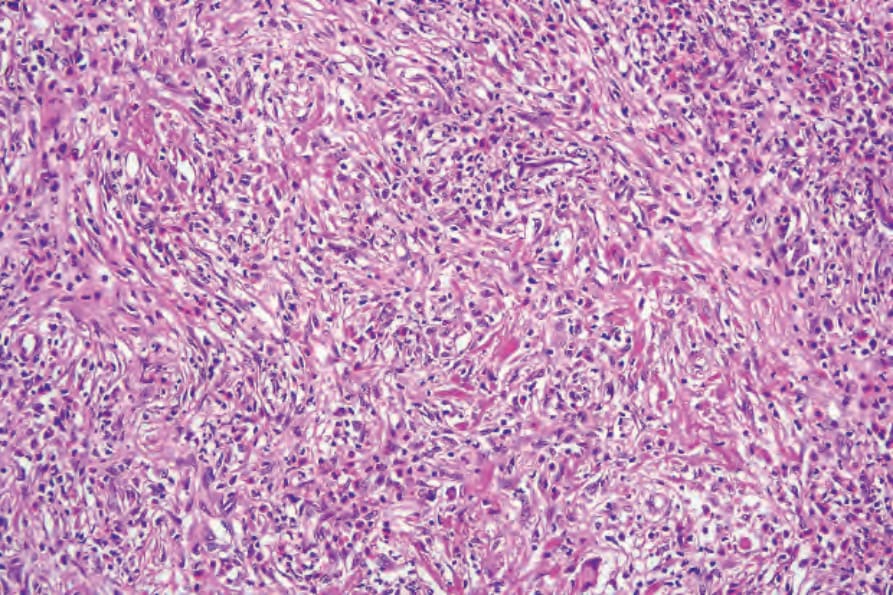
Fig. 16.75 Granuloma faciale: there is a well-developed storiform pattern.