Kawasaki disease (mucocutaneous lymph node syndrome)
Kawasaki disease (mucocutaneous lymph node syndrome)
Kawasaki disease (mucocutaneous lymph node syndrome) is a multisystem disease that predominantly affects infants and young children.1–6 Although it was first described, and shows a marked preponderance, in Japan, it has been diagnosed worldwide and in all races. Kawasaki disease is characterized by both endemic and epidemic variants.4 The incidence among Japanese children is 16–150/100 000/year whereas in white children the incidence is 6–21/100 000/year.4,6,7 The incidence of reported disease in the United States is rising but has been attributed to increased physician awareness.8,9 Kawasaki disease shows a male predominance and occurs most frequently in children aged 6–18 months.10 Adults are only rarely affected.11–14 Kawasaki syndrome is thought to have an infectious etiology on the basis of symptoms of fever and exanthem, age distribution, seasonality (peaks in winter and spring), and occurrence of community-wide epidemics.15
Clinical features The diagnostic features of Kawasaki syndrome are summarized in Table 16.6 and include:
• a spiking fever unresponsive to antibiotic therapy,
• an erythematous polymorphic cutaneous eruption (Fig. 16.61),
• erythema, edema, and induration of the extremities followed by cutaneous desquamation of the tips of the fingers and toes (Fig. 16.62),
• oropharyngeal mucosal changes including edema, erythema, and fissuring of the lips, erythema of the cheeks, and a strawberry (scarletiform) tongue (Figs 16.63 and 16.64),
• bilateral, nonexudative conjunctivitis,
• nonsuppurative cervical lymphadenopathy. In an appropriate clinical context, children are judged to have Kawasaki syndrome if they show a high fever plus four of the signs described above.4,6,16 This has been amended to include coronary artery aneurysm plus three of the above features.4
The cutaneous findings are variable and include erythematous, macular, maculopapular (morbilliform), urticarial, pustular, erythema multiforme-like (targetoid), and erythema marginatum-like lesions.2,6,17 A vesiculopustular eruption has also been reported.18 The skin lesions show a propensity for
738 Vascular diseases
Gastrointestinal involvement presents as abdominal pain, vomiting, and diarrhea. Liver lesions may result in abnormal liver function tests and, less often, jaundice. Pancreatitis and hydrops of the gallbladder are seen in approximately 10% of patients.2
the trunk and extremities, but may be more generalized. A diffuse, erythematous macular or plaquelike eruption involving the perineum is said to be characteristic.5,6 This can be pruritic or painful and typically desquamates. Transverse orange-brown or white color changes of nails can be seen in up to 75% of cases.19 Beau lines are another nail finding.6 Rare cases of alopecia have been described.20
Neurological symptoms develop in about 30% of patients and include features of aseptic meningitis, seizures, and transient paralyses.2 Arthralgias and arthritis are present in up to 30% to 40%, although chronicity is not a feature. Renal involvement manifests as sterile pyuria, hematuria, and infarction.
The features of adult Kawasaki syndrome are essentially those described above and can include erythema of the buttocks, as illustrated in Fig. 16.65. Coronary artery aneurysm, however, appears to be a less common complication.11 It is important to differentiate this condition from staphylococcal toxic shock syndrome.23
Occasionally, patients develop a relapse, which may occur years after initial disease and resolution.24
Pathogenesis and histologic features The etiology of this disease is unknown, but an infectious trigger is likely. Some evidence points to an immunoregulatory defect of T cells stimulated by superantigen-producing strains of Streptococcus pyogenes and S. aureus.23,25,26 Superantigens are a class of microbial antigens that are thought to be capable of stimulating a large number of naive T cells in a non-specific manner by binding to histocompatibility antigens on antigen-presenting cells leading to T-cell activation. Superantigens have been postulated to play a role in the pathogenesis of a number of skin diseases in addition to Kawasaki disease, such as atopic dermatitis, psoriasis, and toxic shock syndrome. However, in one study, superantigen-producing bacteria were found in 56% of cultures (taken from throat, rectum, and groin) from patients with Kawasaki disease compared with 35% of controls with positive culture.27 These differences did not achieve statistical significance. Another study found strains of streptococci and staphylococci in the jejunum of patients with Kawasaki disease but not in controls.28 These same authors, in a follow-up study, found V beta 2+ T cells selectively increased in small bowel mucosa
Cervical lymphadenopathy affects 50% to 75% of patients and may be unilateral or bilateral and involves one or a group of nodes.
Cardiovascular involvement is characteristic and is the most important cause of morbidity and mortality.2 Some 50% of patients show evidence of myocarditis, which may progress to congestive cardiac failure. Pericardial effusion (subclinical) is not uncommon. Of particular significance is the development of coronary artery ectasia or aneurysm, a feature that develops in 15% to 25% of patients, which may be complicated by coronary artery ischemia, thrombosis, and infarction. In 2% of patients, it proves fatal.13 In a very large follow-up study of 594 patients, the incidence of coronary artery aneurysm was 25%.21 Angiographic evidence of regression was seen in 55% of patients.21 There is an inverse relationship between the size of the aneurysm and the likelihood of resolution: large aneurysms, especially giant aneurysms (defined as greater than 8.0 mm), tend to persist, or become obstructed or stenotic.22
of Kawasaki patients compared with control subjects.29 Other research has demonstrated IgA plasma cells and oligoclonal IgA response in affected arterial tissue, suggesting that the disease may be triggered from a pathogen at a mucosal site.30 Clearly, further research is necessary to elucidate the precise pathogenesis of Kawasaki disease.
Other infectious agents that have been implicated, but not proved to be involved in the pathogenesis of Kawasaki disease, include retroviruses, rickettsiae, spirochetes Propionibacterium acnes, M. pneumoniae, Epstein-Barr virus, and adenoviruses.5,6,31 Additionally favored hypotheses include exposure to house mites and recently cleaned or shampooed carpet, living in close proximity to open water or complicating a recent respiratory illness.15 It is likely that Kawasaki disease represents a vasculitic disorder developing as a consequence of multiple infectious agents in a genetically susceptible individual.
739 Granuloma faciale

Fig. 16.61 Kawasaki disease: erythematous macular eruption. By courtesy of W.G. Phillips, MD, Institute of Dermatology, London, UK.

Fig. 16.62 Kawasaki disease: desquamation of the skin of the toes is a characteristic finding. By courtesy of J. Ross, MD, Lewisham Hospital, London, UK.

Fig. 16.63 Kawasaki disease: the lips are erythematous and swollen. Angular cheilitis is evident. By courtesy of J. Ross, MD, Lewisham Hospital, London, UK.

Fig. 16.64 Kawasaki disease: the tongue shows intense erythema. By courtesy of J. Ross, MD, Lewisham Hospital, London, UK.

Fig. 16.65 Kawasaki disease: disease in an adult is very rare. In this patient, the erythema particularly affects the buttocks and thighs. By courtesy of W.G. Phillips, MD, Institute of Dermatology, London, UK.
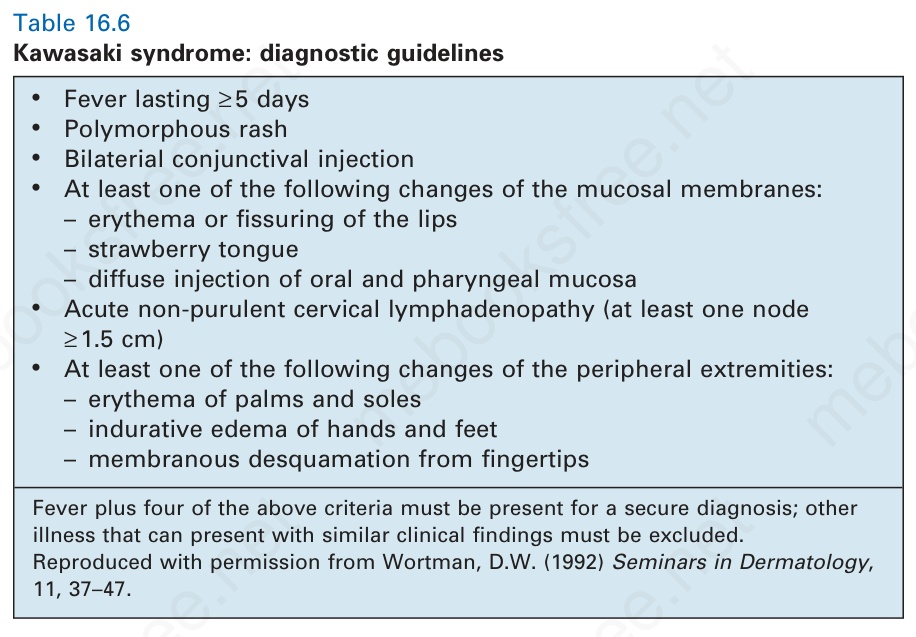
Table 16.6 Kawasaki syndrome: diagnostic guidelines