Polyarteritis nodosa
Polyarteritis nodosa
Classic polyarteritis nodosa (Kussmaul-Maier disease) is a rare systemic vasculitis predominantly involving medium-sized and small arteries.1,2 Some view the disorder not as a disease sui generis but, less restrictively, as a syndrome with many triggering causes and disease associations. Classic polyarteritis nodosa overlaps both clinically and histologically with microscopic polyangiitis (microscopic polyarteritis nodosa, microscopic polyarteritis), but polyarteritis nodosa is predominantly a medium vessel vasculitis while microscopic polyangiitis is predominantly a small-vessel vasculitis and is discussed elsewhere.2
decade.6,7 There is a male predilection (4 : 1). Patients commonly present with constitutional symptoms including weight loss, pyrexia, and anorexia.1
Cutaneous lesions are common and are present in 30% to 60% of patients.6–12 Palpable purpuric lesions and foci of ulceration, particularly involving the lower limbs, are most often found (Figs 16.46–16.48).11 Livedo reticularis is also a common cutaneous manifestation (Fig. 16.49). Cutaneous nodules may also be seen. A maculopapular rash, vesiculation, and pustular lesions are occasional features (Figs 16.50–16.53).
Joint involvement (arthralgias and arthritis) is often present; arthritis is usually asymmetrical and particularly affects the lower limbs. Non-specific muscle pain and weakness are additional features. Muscle wasting is commonly found.
Clinical features Classical polyarteritis nodosa Classic polyarteritis nodosa is a multisystem disease with protean clinical manifestations (Table 16.5).1,3–6 It should be noted that the 1990 criteria from the American College of Rheumatology did not distinguish polyarteritis nodosa from microscopic polyarteritis. However, in the more recent Chapel Hill consensus nomenclature, they are divided by the size of vessel involved (see Table 16.1).2,6 Polyarteritis nodosa is associated with significant morbidity and mortality even when treated with corticosteroids. With therapy, survival is in the range of 75% to 80%.1 Although a wide age group may be affected, patients are most often in their fifth or sixth
Both peripheral and CNS involvement are often encountered. The former presents as sensory neuropathies (numbness or paresthesias), motor neuropathies (wrist or foot drop), and combined sensorimotor lesions (mononeuritis multiplex and polyneuropathy). CNS involvement may present as confusion, disorientation, or delirium. Eye involvement is a rare feature of polyarteritis nodosa.13,14 Complications include choroidal infarction, ischemic optic neuropathy, retinal artery occlusion, episcleritis, ulcerative keratitis, uveitis, and orbital pseudotumor.13–16
Involvement of the kidney is common and is of major importance because its sequelae – renal failure and hypertension – are among the commonest causes of death in this disease.1,6,12 Patients on occasion have episodes of loin pain due to renal infarction. Hypertension is often present in patients with classical polyarteritis nodosa and in some patients it may enter the malignant phase. Urinalysis for proteinuria, hematuria and red cell casts, and serum creatinine estimations are therefore mandatory early investigations.
733 Polyarteritis nodosa
A
B
Gastrointestinal involvement is also an important cause of morbidity and mortality.6,12,17,18 Symptoms include nausea, vomiting, and abdominal pain. Serious complications include gastrointestinal hemorrhage, perforation, and infarction, the last being a not uncommon cause of death. Involvement of the hepatobiliary tract may also be seen.19,20 Involvement of the gallbladder and pancreas has also been reported and can represent an incidental finding or patients may present with symptoms of acute cholecystitis.21,22
Cardiac involvement occurs in less than one third of cases.6,12 Manifestations include pericarditis, arrhythmias, and myocardial infarction due to
coronary artery involvement (Fig. 16.54).23 Although it is often stated that polyarteritis nodosa does not involve the lung, in exceptional cases pulmonary involvement is seen and patients occasionally complain of asthma, hemoptysis, and effusions. Although clinical involvement of the lungs is rare, autopsy evaluation has shown that arteritis affecting the bronchial arteries is not uncommon, being seen in 70% in one small series.24
Orchitis, usually unilateral, is a characteristic feature of polyarteritis nodosa.25–27 Affected patients present with symptoms of acute orchitis or features that suggest a testicular neoplasm.25,27
Laboratory investigations often reveal anemia, leukocytosis, and a raised ESR. Low-titer rheumatoid factor and antinuclear antibody are sometimes features and, in occasional patients, a cryoglobulin is identified. Diminished serum complement levels may also be detected. ANCAs are uncommonly
734 Vascular diseases
seen in patients with classic polyarteritis nodosa. One group with extensive experience estimates that less than 5% of patients with the classic form of the disease have ANCAs.28 However, the presence of ANCAs should prompt strong consideration of an ANCA-related vasculitis rather than polyarteritis nodosa.6 Polyarteritis nodosa in children may present in two forms: the infantile variant, which may be related to Kawasaki disease, and a childhood form, which is similar to adult polyarteritis nodosa (see also section on Kawasaki disease).29
Cutaneous polyarteritis nodosa In addition to classic polyarteritis nodosa, ‘localized (cutaneous) polyarteritis nodosa’ has also been described.30–39 This is a relatively benign variant in which patients develop cutaneous lesions, often over very prolonged periods, but serious visceral involvement is, by definition, never a feature. In one study, none of 79 patients with cutaneous polyarteritis nodosa who were followed for an average of 6.9 years developed systemic vasculitis.30 It may occur at any age, including childhood, and shows no sex predilection. The disease has occasionally been associated with minocycline treatment.40–42
Patients have recurrent episodes during which tender, painful nodules develop, particularly on the lower legs, although these may sometimes be
735 Polyarteritis nodosa
quite widespread. Individual lesions vary from 2 mm to 2 cm in diameter. In the early stages they are pink or red, while more established nodules may have a purplish coloration. Patients sometimes also manifest livedo reticularis, usually on the lower legs and often related to groups of nodules. Other complications include ulceration and, rarely, gangrene. Very occasionally, patients develop lesions reminiscent of atrophie blanche.30
virus.56,58 Parvovirus infection has been associated with polyarteritis nodosa in occasional cases.59,60
In childhood polyarteritis nodosa, there appears to be a striking association with group A streptococci.61
Although there is some evidence to suggest a role for immune complexes generated during infection, such a relationship cannot be demonstrated in many cases. Therefore, the pathogenesis of classic polyarteritis nodosa is unclear in many patients.
In a small subset of patients, the disease is related to deficiency of adenosine deaminase 2 (DADA2). This is a recently described autoinflammatory disease secondary to mutations of CECR1 on chromosome 22q11.1. It is characterized by early childhood onset of livedoid vasculopathy with CNS involvement and mild immunodeficiency. Patients frequently have clinical and histopathological findings indistinguishable from polyarteritis nodosa, reflecting that concept of multiple pathogenetic pathways.62,63 The early onset is in stark contrast to conventional polyarteritis nodosa. Therefore, investigation for this possible genetic condition should be considered in cases encountered in infants and young children.
Other features include fever, malaise, arthralgias, and myalgias, and peripheral nerves may be affected, but there is never any evidence of more widespread visceral involvement.32,36,37
Immunofluorescence often reveals IgM and/or complement in the walls of cutaneous arteries, suggesting a possible immune complex pathogenesis.43 Rare reports of infants of mothers with cutaneous polyarteritis developing the disease and experiencing subsequent resolution are suggestive of a pathogenic circulating factor.44
Pathogenesis and histologic features The pathogenesis of polyarteritis nodosa is poorly understood. Classic polyarteritis nodosa has been suggested to be immune-complex mediated, on the basis of serum immune-complex levels, immunofluorescence investigations, and ultrastructural studies. However, in many patients immune complexes cannot be demonstrated and their role in the development of this disease is controversial. Important suspect antigens include hepatitis B virus (HBV) surface antigens and cryoglobulins.45–48 It has been shown that a significant number of patients with polyarteritis nodosa have circulating HBV antigen.10,48 Furthermore, circulating immune complexes containing HBV antigen and immunoglobulin have been characterized in occasional patients.10 HBV surface antigen has also been identified within affected vessels in a small number of patients.10 A decrease in HBV-associated cases of polyarteritis nodosa in France has been reported and it has been suggested that this phenomenon is the result of vaccination programs.49 Rarely, however, polyarteritis nodosa may also develop following hepatitis B vaccination.50 Human immunodeficiency viral infection has also been reported in cases of polyarteritis nodosa or a polyarteritis nodosa-like syndrome.51–57
The histologic features of the cutaneous lesions in both the classic and localized variants of polyarteritis nodosa are similar and changes are variable.64–66 In some instances, the changes are indistinguishable from leukocytoclastic vasculitis involving the superficial dermal vessels (Fig. 16.55). More characteristic, however, is the finding of necrotizing vasculitis involving the muscular arteries of the deep dermis or subcutaneous fat; these are the changes that are also seen in the internal viscera, often associated with infarction (Fig. 16.56). Although the whole circumference and thickness of the vessel wall is often affected, sometimes the changes are focal. Typically in polyarteritis nodosa, the vascular changes are discontinuous, with uninvolved skip lesions between affected segments (Fig. 16.57).

Fig. 16.46 Polyarteritis nodosa: (A) a sharply defined ulcer with an indurated purplish border on the shin; (B) multiple ulcers, nodules, and foci of livedo reticularis. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 16.47 Polyarteritis nodosa: this patient presented with large hemorrhagic lesions on the legs. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.48 Polyarteritis nodosa: epidermal infarction has resulted in these digital ulcers. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
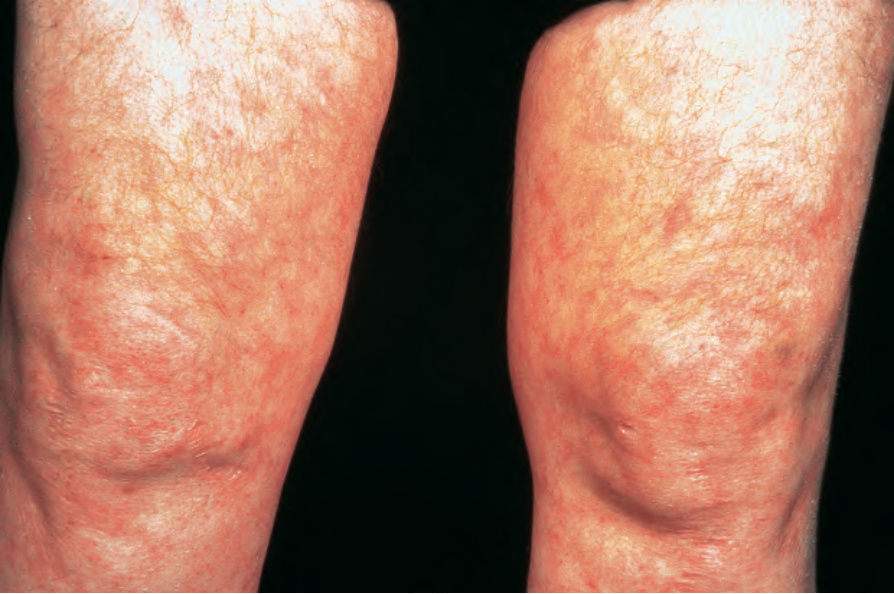
Fig. 16.49 Polyarteritis nodosa: this patient shows florid livedo reticularis. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.50 Polyarteritis nodosa: erythematous macules are occasionally seen. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.51 Polyarteritis nodosa: erythematous papules are present around this patient’s ankles. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.52 Polyarteritis nodosa: this patient presented with acral erythematous lesions. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.53 Polyarteritis nodosa: in some patients, an intense neutrophil infiltrate results in pustular lesions as seen in this patient. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.54 Polyarteritis nodosa: coronary arteries showing conspicuous aneurysmal dilatation are now very rarely seen (museum specimen). By courtesy of the Department of Pathology, St Thomas’ Hospital, London, UK.
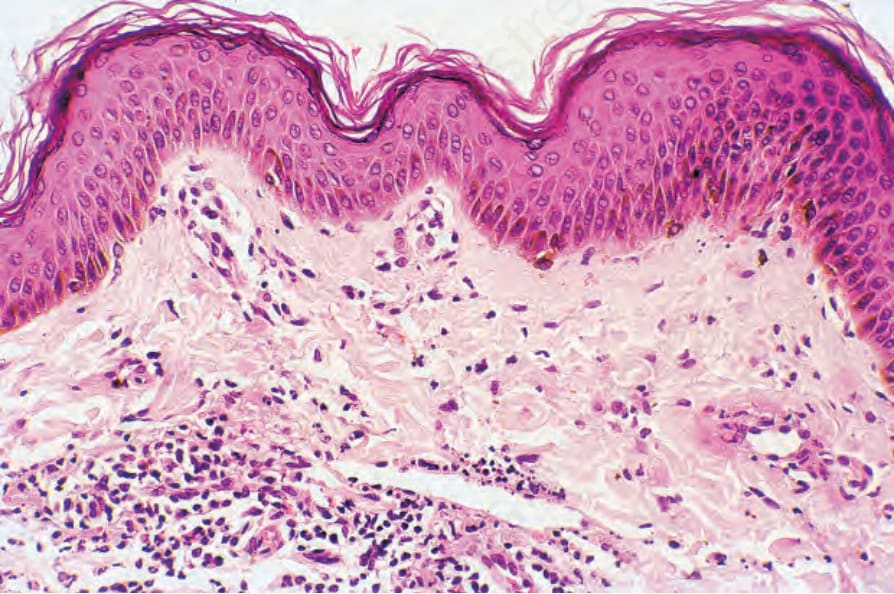
Fig. 16.55 Polyarteritis nodosa: in this case the features are those of a superficial leukocytoclastic vasculitis. It is important to remember that this histologic lesion may represent a serious systemic disease.
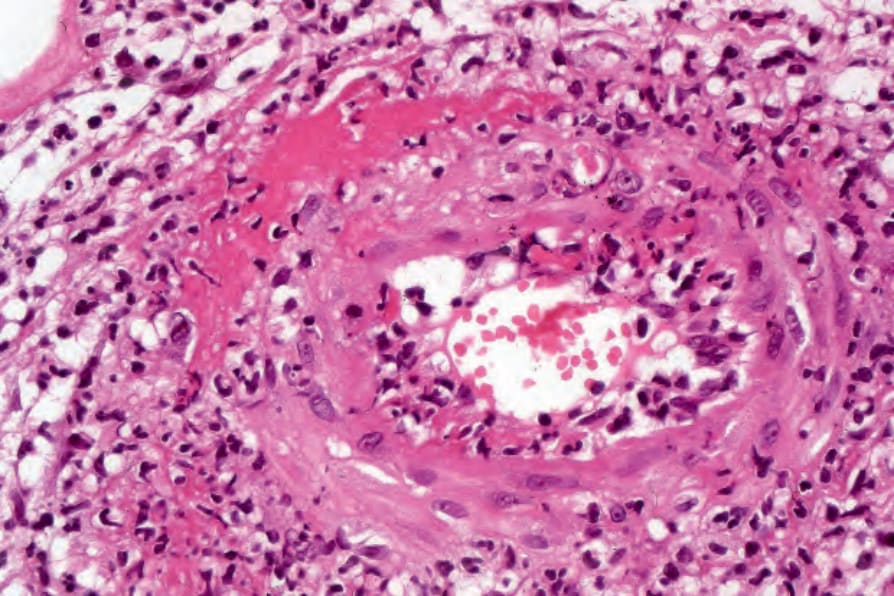
Fig. 16.56 Polyarteritis nodosa: high-power view showing fibrinoid necrosis.
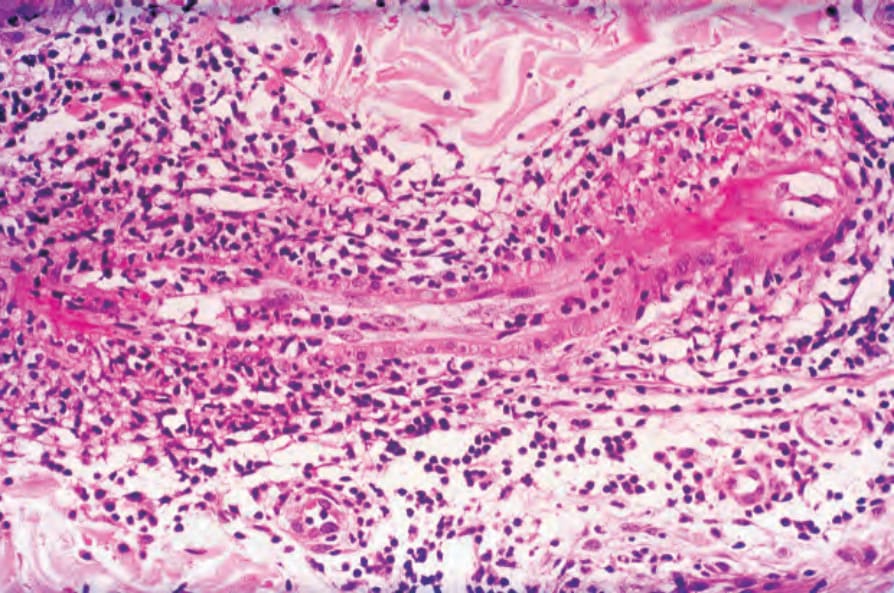
Fig. 16.57 Polyarteritis nodosa: while fibrinoid necrosis involves both lateral extremities of this vascular segment, the middle portion is relatively unaffected.

Fig. 16.61 Kawasaki disease: erythematous macular eruption. By courtesy of W.G. Phillips, MD, Institute of Dermatology, London, UK.
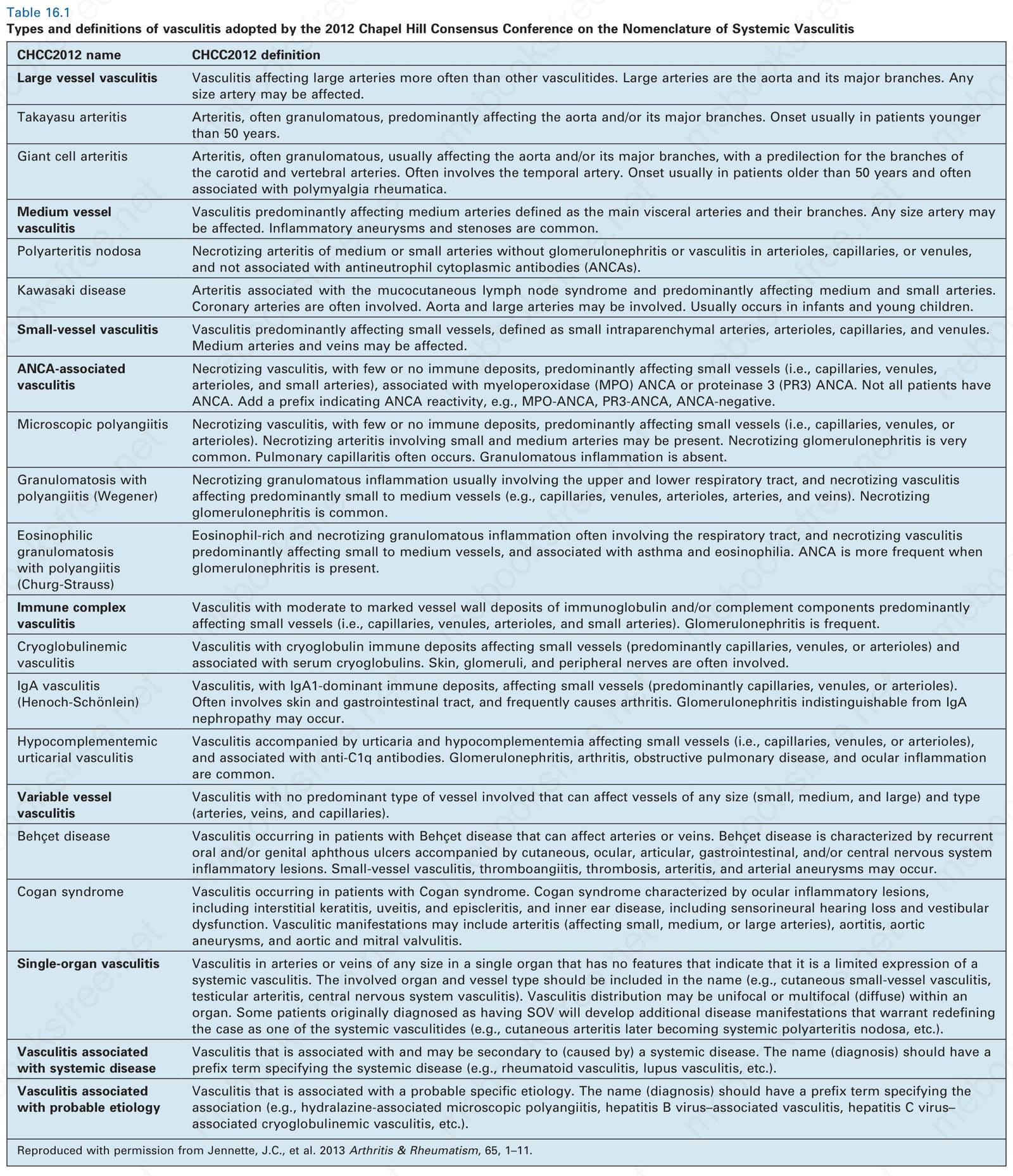
Table 16.1 Types and definitions of vasculitis adopted by the 2012 Chapel Hill Consensus Conference on the Nomenclature of Systemic Vasculitis
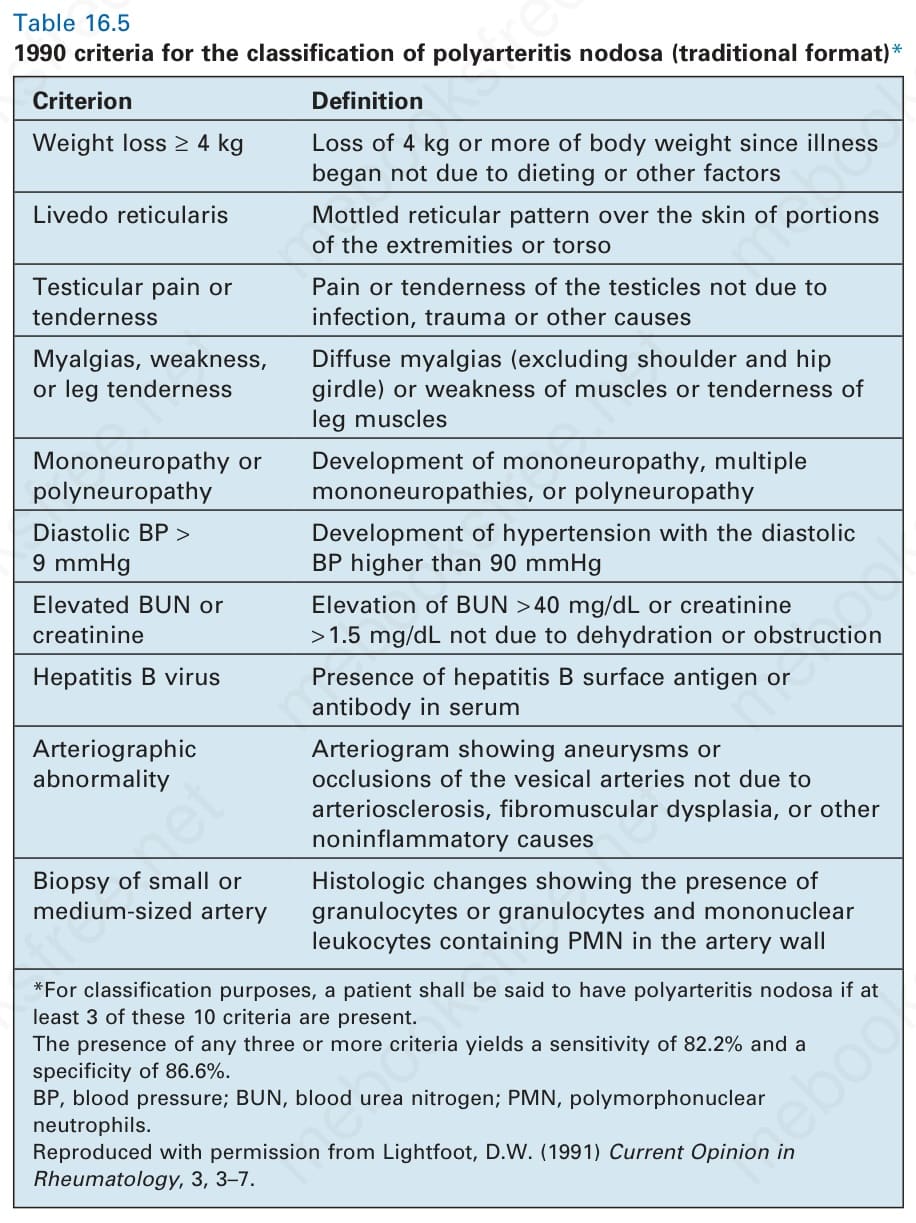
Table 16.5 1990 criteria for the classification of polyarteritis nodosa (traditional format)*
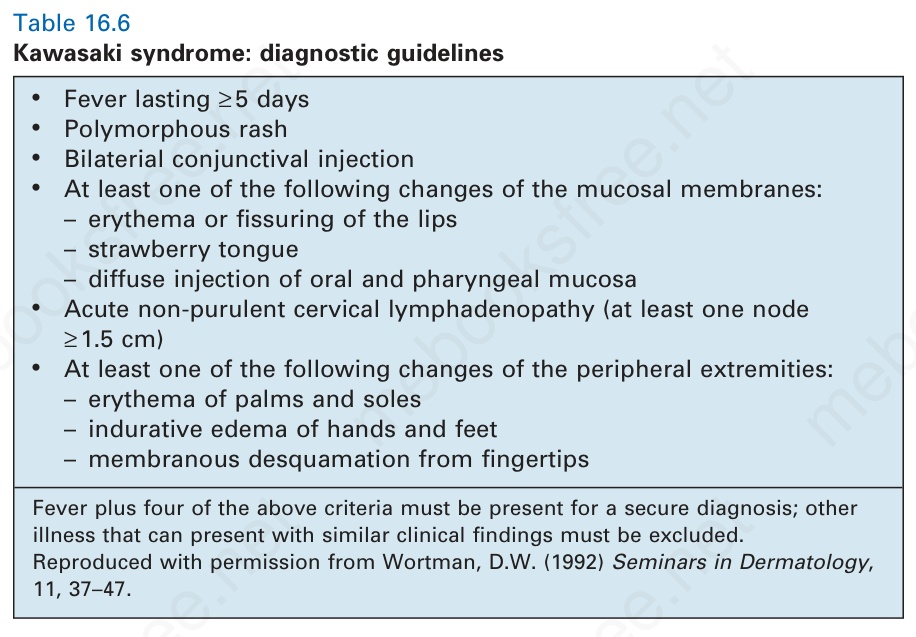
Table 16.6 Kawasaki syndrome: diagnostic guidelines
Evidence of hepatitis C viral infection has been documented in some patients. In one study, 20% of patients had antibodies against hepatitis C
The acute changes, those of fibrinoid necrosis, involve the muscle coat and often destroy the internal elastic lamina; this is often best appreciated by the use of a stain for elastic tissue (Fig. 16.58). Associated with the necrosis is an inflammatory cell infiltrate of neutrophils, eosinophils, and mononuclear cells. Leukocytoclasis is sometimes an additional feature. Thrombosis is common and may be complicated by ischemic necrosis of the surface epithelium. Healing lesions are associated with fibroblastic proliferation and eventual fibrous scarring. In the healing phase a lymphocytic infiltrate rather than a neutrophilic infiltrate is often present.68,69 Endarteritis is often evident and any disruption of the internal elastic lamina is permanent. A characteristic feature that often presents in wedge biopsies that contain multiple vessels is the presence of lesions at varying stages of evolution. Deep, surgical incisional biopsies are essential for the diagnosis of cutaneous involvement in polyarteritis nodosa. A punch biopsy will often
736 Vascular diseases
A
B
not sample larger vessels that are typically affected. Furthermore, the diagnosis is subject to sampling error due to the multifocal nature of the disease. Aneurysm formation may sometimes be appreciated microscopically.1
Internal visceral involvement is based upon the effects of necrotizing arteritis. Interestingly, nodular swellings (aneurysms) are much more obvious. The effects depend upon the relative interplay of infarction and hemorrhage. Renal involvement in classical polyarteritis nodosa is predominantly due to large-vessel vasculitis, with resultant thrombosis and infarction, coupled with the effects of hypertension (Fig. 16.59).67 Patients may also manifest focal, segmental proliferative or necrotizing glomerulonephritis similar to that seen in patients with microscopic polyarteritis nodosa (Fig. 16.60).
Differential diagnosis Distinction between classic polyarteritis nodosa and microscopic polyangiitis is based on the size of vessels involved, spectrum and type of organ involvement, and presence of ANCAs. Similar to polyarteritis nodosa, erythema induratum frequently shows vasculitis of medium-sized vessels, but also has an associated lobular panniculitis in contrast to polyarteritis nodosa. Cutaneous lymphocytic thrombophilic/macular lymphocytic arteritis likely represents the healing phase of polyarteritis nodosa rather than a distinct entity.68–70
737 Kawasaki disease (mucocutaneous lymph node syndrome)
• Fever lasting ≥ 5 days
• Polymorphous rash
• Bilaterial conjunctival injection
• At least one of the following changes of the mucosal membranes: – erythema or fissuring of the lips – strawberry tongue – diffuse injection of oral and pharyngeal mucosa
• Acute non-purulent cervical lymphadenopathy (at least one node ≥ 1.5 cm)
• At least one of the following changes of the peripheral extremities: – erythema of palms and soles – indurative edema of hands and feet – membranous desquamation from fingertips
Fever plus four of the above criteria must be present for a secure diagnosis; other illness that can present with similar clinical findings must be excluded. Reproduced with permission from Wortman, D.W. (1992) Seminars in Dermatology, 11, 37–47.
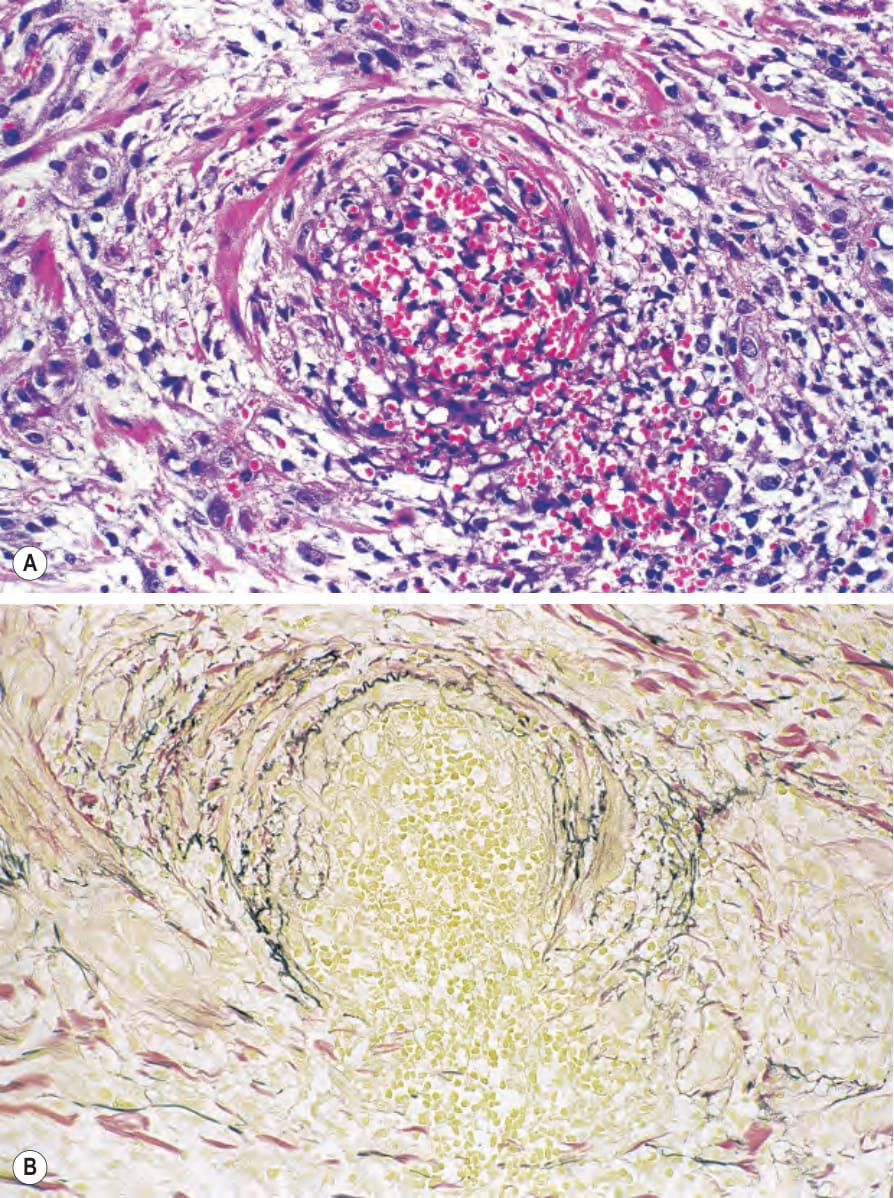
Fig. 16.58 Polyarteritis nodosa: (A) there is marked red cell extravasation; (B) elastic–van Gieson staining shows disruption of the internal elastic lamina.
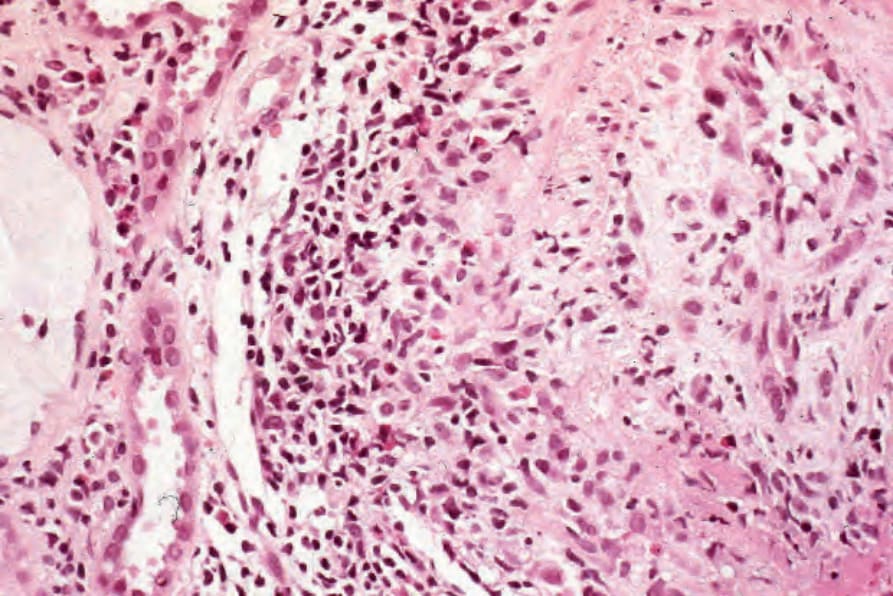
Fig. 16.59 Polyarteritis nodosa: in this kidney section an arcuate artery shows necrotizing vasculitis and fibrointimal thickening. The inflammatory cell infiltrate contains conspicuous eosinophils.
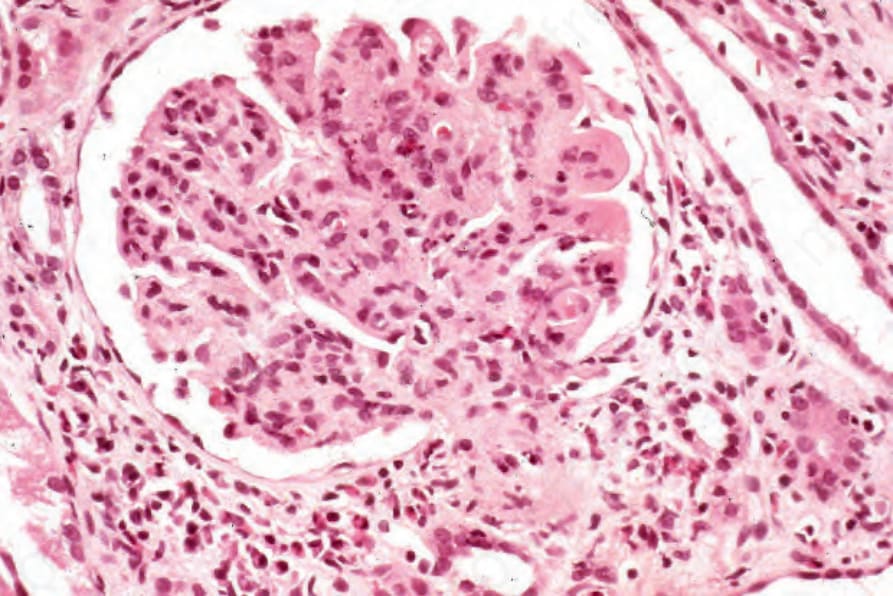
Fig. 16.60 Polyarteritis nodosa: segmental necrotizing glomerulonephritis.