Microscopic polyangiitis
Microscopic polyangiitis
Clinical features Microscopic polyangiitis (microscopic polyarteritis) is a necrotizing vasculitis predominantly affecting small vessels with few to no immune complexes.1 Patients often present with non-specific constitutional symptoms including malaise, fever, and myalgia. There may be a past history of sore throat or a flulike illness, which obviously raises the possibility of an iatrogenic pathogenesis for the subsequent vasculitic process.2 Renal involvement, consisting of glomerulonephritis, is seen in about 90% of patients, manifesting as microscopic hematuria, proteinuria, or acute renal failure.2–6 Hypertension is present in a large proportion of patients. Pulmonary lesions present as hemoptysis, pulmonary fibrosis, and intrapulmonary hemorrhage, which
Pathogenesis and histologic features The precise pathogenesis is uncertain, but ANCAs are clearly implicated. In vitro and mouse studies implicated MPO-ANCA as a causative agent in microscopic polyangiitis.4 Glomerulonephritis can be induced by injection of MPO-IgG into recipient mice.19 There have also been reports suggesting an etiological link related to silica exposure, but this evidence is not conclusive.20–22
Microscopic polyangiitis (microscopic polyarteritis) is characterized by small-vessel leukocytoclastic vasculitis, which may predominantly affect the muscular arterioles, capillaries, and venules (Fig. 16.45).2,16,23 Necrotizing vasculitis with fibrinoid necrosis and variable numbers of neutrophils and monocytes is seen. In early lesions, neutrophils associated with karyorrhexis predominate, while lymphocytes and histiocytes dominate the infiltrate in older lesions. Renal lesions include focal segmental necrotizing glomerulonephritis (often with crescents), vasculitis, interstitial inflammation, and
732 Vascular diseases
Criterion Definition
Weight loss ≥ 4 kg Loss of 4 kg or more of body weight since illness began not due to dieting or other factors
Livedo reticularis Mottled reticular pattern over the skin of portions of the extremities or torso
Testicular pain or tenderness
Pain or tenderness of the testicles not due to infection, trauma or other causes
Myalgias, weakness, or leg tenderness
Diffuse myalgias (excluding shoulder and hip girdle) or weakness of muscles or tenderness of leg muscles
Mononeuropathy or polyneuropathy
Development of mononeuropathy, multiple mononeuropathies, or polyneuropathy
Diastolic BP > 9 mmHg
Development of hypertension with the diastolic BP higher than 90 mmHg
Elevation of BUN > 40 mg/dL or creatinine > 1.5 mg/dL not due to dehydration or obstruction
Elevated BUN or creatinine
Hepatitis B virus Presence of hepatitis B surface antigen or antibody in serum
Arteriographic abnormality
Arteriogram showing aneurysms or occlusions of the vesical arteries not due to arteriosclerosis, fibromuscular dysplasia, or other noninflammatory causes
tubular atrophy. Large-vessel disease, visceral infarction, and granulomatous inflammation are not features.
Differential diagnosis The absence of involvement of capillaries and venules in classic polyarteritis nodosa is a major point of distinction from microscopic polyangiitis. IgA vasculitis and conventional leukocytoclastic vasculitis tend to affect superficial vessels predominantly, whereas microscopic polyangiitis usually involves superficial and deep vessels. However, this is not sufficiently reliable. Microscopic polyangiitis may also be confused with granulomatosis with polyangiitis and eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome). The presence of granulomatous inflammation in the lung favors the first of the last two conditions. The presence of blood eosinophilia and asthma favors a diagnosis of eosinophilic granulomatosis with polyangiitis. Ultimately, microscopic polyangiitis is a diagnosis of exclusion. Therefore, the biopsy findings must never be used in isolation to determine the diagnosis. Only after careful clinical, serological, and histologic correlation should a definitive diagnosis be rendered. Careful clinical investigation is required to evaluate for underlying causes/disease associations.
Biopsy of small or medium-sized artery
Histologic changes showing the presence of granulocytes or granulocytes and mononuclear leukocytes containing PMN in the artery wall
*For classification purposes, a patient shall be said to have polyarteritis nodosa if at least 3 of these 10 criteria are present. The presence of any three or more criteria yields a sensitivity of 82.2% and a specificity of 86.6%. BP, blood pressure; BUN, blood urea nitrogen; PMN, polymorphonuclear neutrophils. Reproduced with permission from Lightfoot, D.W. (1991) Current Opinion in Rheumatology, 3, 3–7.
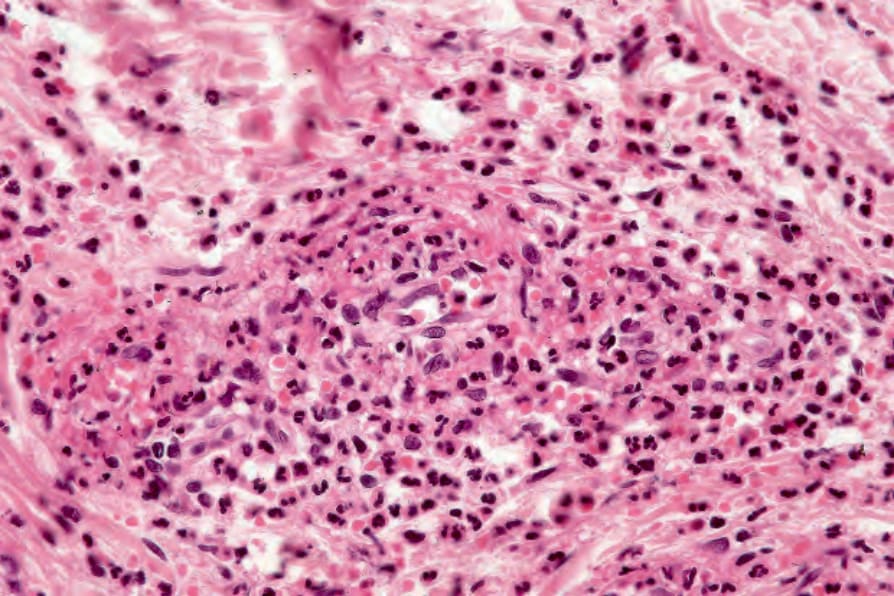
Fig. 16.45 Microscopic polyarteritis nodosa: acute necrotizing vasculitis of a small muscular arteriole is evident. Numerous eosinophils are present.
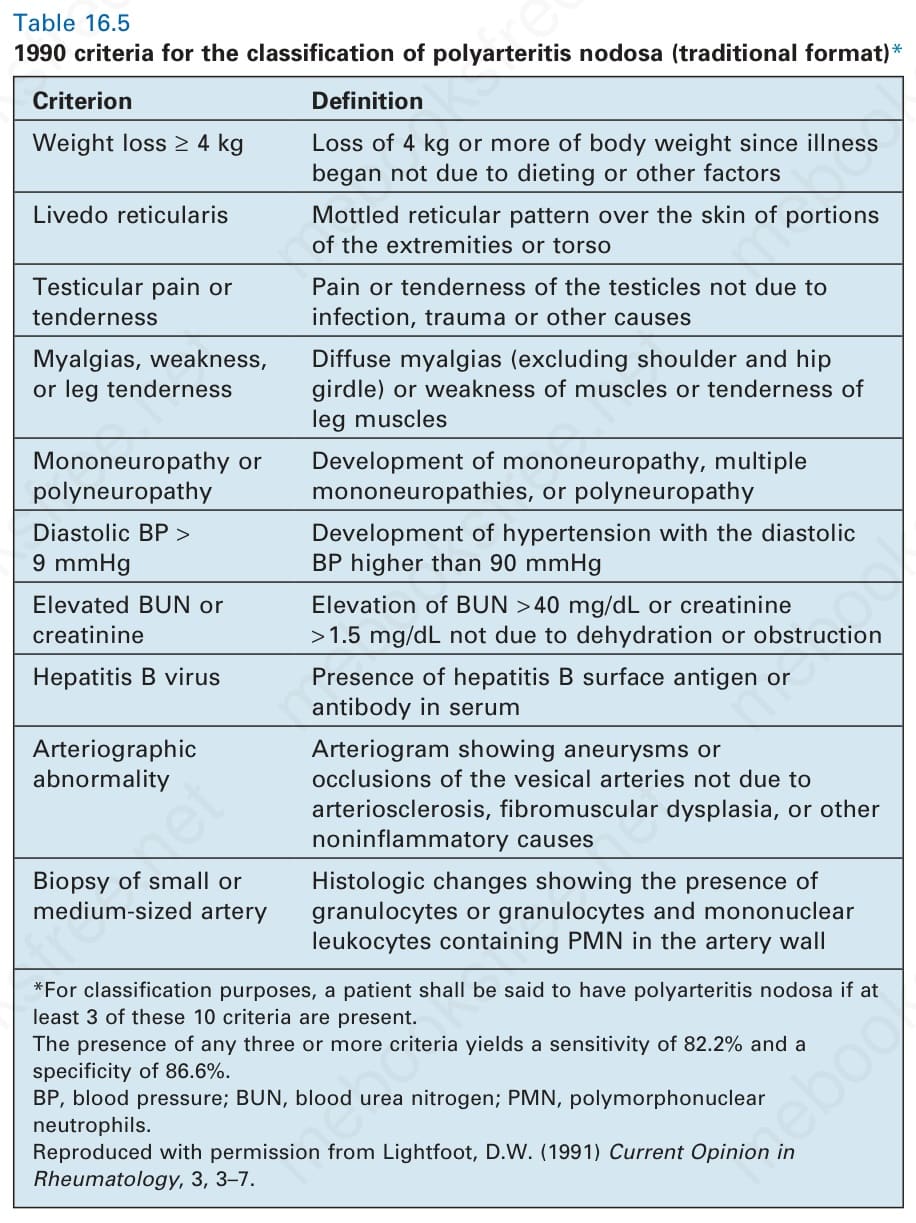
Table 16.5 1990 criteria for the classification of polyarteritis nodosa (traditional format)*