Urticarial vasculitis
Urticarial vasculitis
Clinical features Urticarial vasculitis is an uncommon condition characterized clinically by urticaria and histologically by leukocytoclastic venulitis.1–5 In addition to urticarial skin lesions, patients may also experience angioedema, arthralgia, gastrointestinal symptoms, and evidence of renal involvement.6,7 The term encompasses a spectrum of illness, with some patients experiencing only mild symptoms while others develop serious systemic involvement.7,8
Urticarial vasculitis is most often seen in the third to fifth decades and shows a female predominance.7 The cutaneous lesions are urticarial in appearance, consisting of edematous, raised, erythematous plaques associated with nonblanchable purpura (Figs 16.23 and 16.24). However, in contrast to uncomplicated urticaria, cutaneous lesions of urticarial vasculitis
The ESR is raised in many patients with hypocomplementemia. There may also be depression of the early classic pathway components C1q, C4, and C2. Patients with hypocomplementemic urticarial vasculitis have a high prevalence of autoantibodies to endothelial cells.21,22 Elevated rheumatoid factor has also been reported.23
724 Vascular diseases
Schnitzler syndrome is a term that has been applied to patients with urticarial vasculitis and monoclonal IgM gammopathy.24–29 Hepatosplenomegaly, elevated ESR and white blood cell count, fever, and joint pain are characteristic features.25–27 An associated monoclonal IgA gammopathy has been reported and an underlying lymphoproliferative disorder is present in some patients.24,30,31 In one series, 90% had a monoclonal IgM gammopathy, 5% had a monoclonal IgA gammopathy, and 5% had a monoclonal IgG gammopathy. Interestingly, these patients had perivascular and/or interstitial neutrophilic infiltrate or a mononuclear infiltrate with eosinophils, but none had vasculitis.32 The current Strasbourg criteria in fact do not require vasculitis. Obligate criteria include a chronic urticarial rash and a monoclonal IgM or IgG gammopathy. Minor criteria include recurrent fever, objective findings of abnormal bone remodeling, neutrophilic dermal infiltrate, and leukocytosis and/or elevated CRP. Patients with IgM paraproteinemia require both obligate criteria and two minor criteria, while patients with IgG paraproteinemia require both obligate criteria and three minor criteria.33 These criteria have > 80% sensitivity and > 90% specificity for the diagnosis.34
Importantly, urticarial vasculitis (especially the hypocomplementemic variant) is often associated with, or heralds the onset of, a variety of systemic diseases, including SLE, arthritis, interstitial lung disease, pericarditis, mixed connective tissue disease, systemic sclerosis, relapsing polychondritis, hepatitis, inflammatory bowel disease, serum sickness, polyarteritis nodosa and Granulomatosis with polyangiitis, viral infection, Sjögren syndrome, cryoglobulinemia, polycythemia rubra vera, reaction to drugs (including cocaine and diltiazem), and as a response to sunlight.8,13,14,35–46 The condition may be exacerbated by methotrexate.47 More than 50% of patients had uveitis, scleritis, conjunctivitis, or episcleritis.8,13 It appears that patients with hypocomplementemia have more severe disease.38 Some authors have postulated that hypocomplementemic urticarial vasculitis represents a subset of SLE. Others, however, have failed to confirm this observation.8,48,49
Urticarial vasculitis has been documented in association with malignancy.8,50–58 Given the rarity of this association, this may well be coincidental. Nevertheless, a diagnosis of urticarial vasculitis should always initiate an evaluation for possible underlying disease. Urticarial vasculitis usually has a benign outcome.8
Pathogenesis and histologic features In many patients, no underlying cause is discovered. In others, antibody- antigen complexes (a type III hypersensitivity reaction) is implicated.4,5 Mutations in DNASE1L3 have been identified in two families with autosomal recessive hypocomplementemic urticarial vasculitis.59 Mutations in this same gene have been implicated in SLE.
cyclophosphamide therapy it was associated with a dismal prognosis. Mean survival was of the order of 5 months following diagnosis and approximately 80% of patients died within 1 year, most as a consequence of renal involvement.
Although it may present in a wide variety of age groups, from infancy to the elderly, it is the middle aged that are predominantly affected, with a peak incidence in the fourth decade.1–5 There is a slight predilection for males (3 : 2). In one large study, 97% of patients were Caucasians.6
The vasculitis affects the superficial vascular plexus and is characterized by a leukocytoclastic pattern (Fig. 16.25). Extravasation of red blood cells is evidence of vascular damage. A background of dermal edema may be seen. Often, the histologic features are subtle and are easily overlooked, with only focal fibrinoid vascular change, few neutrophils, and sparse karyorrhexis. In our experience, the vasculitis is usually low grade or subtle in nature; however, more impressive necrotizing vasculitis is seen in some patients. Others have shown that endothelial necrosis is unusual.5
In summary, urticarial vasculitis may show a spectrum of histologic changes ranging from urticaria with very mild vascular injury to frank necrotizing vasculitis.60
Granulomatosis with polyangiitis comprises a triad of characteristics:
• necrotizing, destructive, granulomatous lesions in the upper respiratory tract (nose, nasal sinuses, nasopharynx, and larynx) and/or in the lower respiratory tract (trachea, bronchi or lungs); frequently, both are present. Similar lesions may also be found in virtually any organ in the body,
• a generalized focal vasculitis occurring in a wide variety of sites, but particularly affecting the lungs,
• glomerulonephritis.3,7,8
Early in the disease, when patients may not have developed the full clinical triad, definitive diagnosis can be difficult or impossible (see Table 16.3). According to the current Chapel Hill criteria, glomerulonephritis is not requisite for the diagnosis.3 The most common presenting symptoms relate to involvement of the nose and nasal sinuses, and include severe and often purulent nasal discharge or evidence of sinusitis with pain and discharge. Clinical examination may reveal mucosal ulceration, perforated septum, paranasal sinusitis, or a saddle-nose deformity. Serous or purulent otitis media is occasionally a presenting feature. Middle and inner ear involvement is also a common manifestation of disease.9–12
Differential diagnosis Clinical correlation is necessary to distinguish urticarial vasculitis from other forms of leukocytoclastic vasculitis. Although urticarial vasculitis is often associated with subtle low-grade vascular injury, this feature should not be relied upon in its distinction from other forms of vasculitis. In short, the pathologist’s role in diagnosis is to confirm the presence of vasculitis.

Fig. 16.23 Urticarial vasculitis: this very large lesion has developed a bizarre outline due to central clearing. By courtesy of the Institute of Dermatology, London, UK.
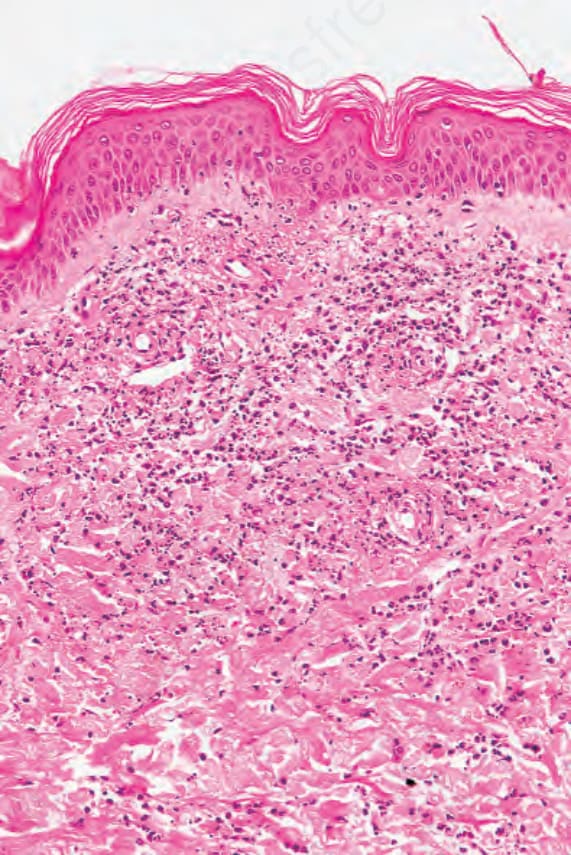
Fig. 16.25 Urticarial vasculitis: the changes are unusually florid in this example.
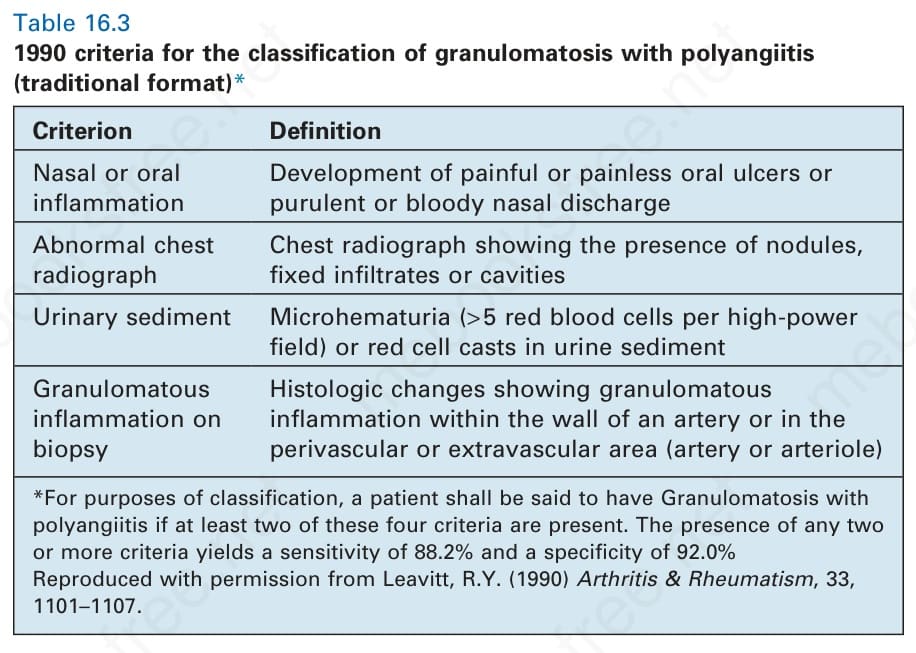
Table 16.3 1990 criteria for the classification of granulomatosis with polyangiitis (traditional format)*