Leukocytoclastic vasculitis
Leukocytoclastic vasculitis
Clinical features Leukocytoclastic vasculitis (allergic vasculitis, cutaneous leukocytoclastic angiitis, hypersensitivity vasculitis, leukocytoclastic angiitis) is the commonest form of vasculitis.1–7 It is not a disease entity but represents a vascular reaction pattern due to circulating immune complexes that may either be idiopathic or caused by a number of underlying disorders. The antigens possibly involved are summarized in Table 16.2.1–8 The most frequent associations are drugs in addition to infections.9,10 In over 40% of cases, however, no underlying condition can be identified.11 Although the condition may be limited to the skin, it is important to recognize that it can also be associated with systemic manifestations involving the joints, kidneys, and gastrointestinal system in between 15% and 50% of patients.5,11–14 The disease occurs equally in men and women, and may present in any age group.
The histologic features of most forms of vasculitis are not specific for an entity per se. A specific diagnosis requires careful clinical, histologic, and serological (i.e., presence of antineutrophil antibodies) correlation.1 The role of the pathologist in evaluating a biopsy is to confirm or deny the presence of vasculitis, and to describe the nature of the inflammatory infiltrate and the type(s) and size(s) of the vessel(s) involved. A histologic differential diagnosis is established to guide patient evaluation. Correct biopsy technique and timing are important to allow for adequate assessment for vasculitis. Incisional biopsies to include sufficient subcutis and larger subcutaneous vessels within the first 48 hours after development of the lesion yield the best results.1
A pathological diagnosis of vasculitis may indicate a primary or secondary disease (i.e., in the setting of connective tissue disease). Secondary forms of vascular disease may manifest as diverse histologic patterns. For example, connective tissue diseases may be associated with either a small-vessel leukocytoclastic disease or a large-vessel vasculitis. Likewise, different histologic
Skin lesions are typically polymorphic, but palpable purpura (nonblanching erythematous papules) is the commonest manifestation (Fig. 16.1). Urticarial, bullous or vesicular, ulceroinfarctive, nodular, pustular, livedoid, and annular lesions may also be encountered (Figs 16.2–16.8).15–19 The
715 Leukocytoclastic vasculitis
CHCC2012 name CHCC2012 definition
Large vessel vasculitis Vasculitis affecting large arteries more often than other vasculitides. Large arteries are the aorta and its major branches. Any size artery may be affected.
Takayasu arteritis Arteritis, often granulomatous, predominantly affecting the aorta and/or its major branches. Onset usually in patients younger than 50 years.
Giant cell arteritis Arteritis, often granulomatous, usually affecting the aorta and/or its major branches, with a predilection for the branches of the carotid and vertebral arteries. Often involves the temporal artery. Onset usually in patients older than 50 years and often associated with polymyalgia rheumatica.
Medium vessel vasculitis
Vasculitis predominantly affecting medium arteries defined as the main visceral arteries and their branches. Any size artery may be affected. Inflammatory aneurysms and stenoses are common.
Polyarteritis nodosa Necrotizing arteritis of medium or small arteries without glomerulonephritis or vasculitis in arterioles, capillaries, or venules, and not associated with antineutrophil cytoplasmic antibodies (ANCAs).
Kawasaki disease Arteritis associated with the mucocutaneous lymph node syndrome and predominantly affecting medium and small arteries. Coronary arteries are often involved. Aorta and large arteries may be involved. Usually occurs in infants and young children.
Small-vessel vasculitis Vasculitis predominantly affecting small vessels, defined as small intraparenchymal arteries, arterioles, capillaries, and venules. Medium arteries and veins may be affected.
ANCA-associated vasculitis
Necrotizing vasculitis, with few or no immune deposits, predominantly affecting small vessels (i.e., capillaries, venules, arterioles, and small arteries), associated with myeloperoxidase (MPO) ANCA or proteinase 3 (PR3) ANCA. Not all patients have ANCA. Add a prefix indicating ANCA reactivity, e.g., MPO-ANCA, PR3-ANCA, ANCA-negative.
Microscopic polyangiitis Necrotizing vasculitis, with few or no immune deposits, predominantly affecting small vessels (i.e., capillaries, venules, or arterioles). Necrotizing arteritis involving small and medium arteries may be present. Necrotizing glomerulonephritis is very common. Pulmonary capillaritis often occurs. Granulomatous inflammation is absent.
Granulomatosis with polyangiitis (Wegener)
Necrotizing granulomatous inflammation usually involving the upper and lower respiratory tract, and necrotizing vasculitis affecting predominantly small to medium vessels (e.g., capillaries, venules, arterioles, arteries, and veins). Necrotizing glomerulonephritis is common.
Eosinophilic granulomatosis with polyangiitis (Churg-Strauss)
Eosinophil-rich and necrotizing granulomatous inflammation often involving the respiratory tract, and necrotizing vasculitis predominantly affecting small to medium vessels, and associated with asthma and eosinophilia. ANCA is more frequent when glomerulonephritis is present.
Immune complex vasculitis
Vasculitis with moderate to marked vessel wall deposits of immunoglobulin and/or complement components predominantly affecting small vessels (i.e., capillaries, venules, arterioles, and small arteries). Glomerulonephritis is frequent.
Cryoglobulinemic vasculitis
Vasculitis with cryoglobulin immune deposits affecting small vessels (predominantly capillaries, venules, or arterioles) and associated with serum cryoglobulins. Skin, glomeruli, and peripheral nerves are often involved.
IgA vasculitis (Henoch-Schönlein)
Vasculitis, with IgA1-dominant immune deposits, affecting small vessels (predominantly capillaries, venules, or arterioles). Often involves skin and gastrointestinal tract, and frequently causes arthritis. Glomerulonephritis indistinguishable from IgA nephropathy may occur.
Hypocomplementemic urticarial vasculitis
Vasculitis accompanied by urticaria and hypocomplementemia affecting small vessels (i.e., capillaries, venules, or arterioles), and associated with anti-C1q antibodies. Glomerulonephritis, arthritis, obstructive pulmonary disease, and ocular inflammation are common.
Variable vessel vasculitis
Vasculitis with no predominant type of vessel involved that can affect vessels of any size (small, medium, and large) and type (arteries, veins, and capillaries).
Behçet disease Vasculitis occurring in patients with Behçet disease that can affect arteries or veins. Behçet disease is characterized by recurrent oral and/or genital aphthous ulcers accompanied by cutaneous, ocular, articular, gastrointestinal, and/or central nervous system inflammatory lesions. Small-vessel vasculitis, thromboangiitis, thrombosis, arteritis, and arterial aneurysms may occur.
Cogan syndrome Vasculitis occurring in patients with Cogan syndrome. Cogan syndrome characterized by ocular inflammatory lesions, including interstitial keratitis, uveitis, and episcleritis, and inner ear disease, including sensorineural hearing loss and vestibular dysfunction. Vasculitic manifestations may include arteritis (affecting small, medium, or large arteries), aortitis, aortic aneurysms, and aortic and mitral valvulitis.
Single-organ vasculitis Vasculitis in arteries or veins of any size in a single organ that has no features that indicate that it is a limited expression of a systemic vasculitis. The involved organ and vessel type should be included in the name (e.g., cutaneous small-vessel vasculitis, testicular arteritis, central nervous system vasculitis). Vasculitis distribution may be unifocal or multifocal (diffuse) within an organ. Some patients originally diagnosed as having SOV will develop additional disease manifestations that warrant redefining the case as one of the systemic vasculitides (e.g., cutaneous arteritis later becoming systemic polyarteritis nodosa, etc.).
Vasculitis associated with systemic disease
Vasculitis that is associated with and may be secondary to (caused by) a systemic disease. The name (diagnosis) should have a prefix term specifying the systemic disease (e.g., rheumatoid vasculitis, lupus vasculitis, etc.).
Vasculitis associated with probable etiology
Vasculitis that is associated with a probable specific etiology. The name (diagnosis) should have a prefix term specifying the association (e.g., hydralazine-associated microscopic polyangiitis, hepatitis B virus–associated vasculitis, hepatitis C virus– associated cryoglobulinemic vasculitis, etc.).
Reproduced with permission from Jennette, J.C., et al. 2013 Arthritis & Rheumatism, 65, 1–11.
716 Vascular diseases
• Infection – bacterial: Streptococcus – mycobacterial: Mycobacterium tuberculosis – viral: hepatitis, influenza – cytomegalovirus – HIV infection – leprosy
• Drugs – aspirin, phenacetin, sulfonamides, penicillin, iodides, phenothiazines
• Chemicals – insecticides, weed killers, petroleum products
• Foreign proteins – serum sickness – hyposensitization antigens
• Associated diseases – autoimmune diseases: systemic lupus erythematosus, inflammatory
bowel disease – hemolytic anemia – Hodgkin lymphoma, carcinoma – rheumatoid arthritis – mixed connective tissue disease – dermatomyositis – relapsing polychondritis – Sjögren syndrome – IgA vasculitis – cryoglobulinemia – polyarteritis nodosa – Granulomatosis with polyangiitis – Churg-Strauss disease – granuloma faciale – erythema elevatum diutinum – Waldenström hypergammaglobulinemia – sarcoidosis
717 Leukocytoclastic vasculitis
Although occasional cases are asymptomatic, patients not uncommonly complain of pruritus or burning; less frequently, pain is a feature. Additional features, which are sometimes present, include abdominal pain and gastrointestinal bleeding, joint pains with associated erythema and swelling, and evidence of renal involvement.14,21 In severe cases, the features resemble acute glomerulonephritis and the nephrotic syndrome may even supervene. Rarely, patients have respiratory involvement (nodular or diffuse infiltrative lesions on X-ray examination), and very exceptionally the central or peripheral nervous system is affected, causing symptoms such as headache, diplopia, and dysphagia.14
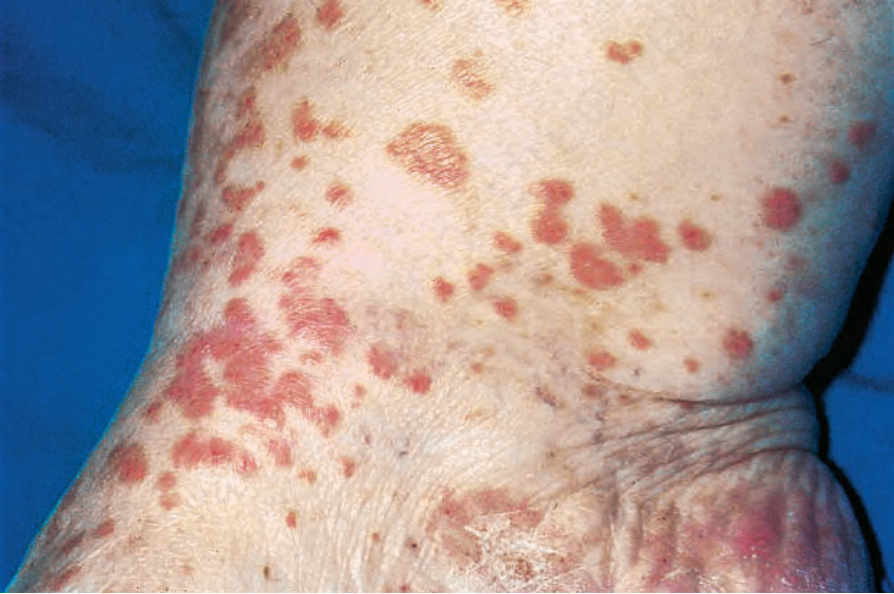
Fig. 16.1 Leukocytoclastic vasculitis: typical erythematous maculopapular lesions are present on the medial aspect of the ankle. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 16.2 Leukocytoclastic vasculitis: close-up view showing small erythematous lesions. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.3 Leukocytoclastic vasculitis: in this patient an extensive purpuric eruption showing central necrosis is evident. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 16.4 Leukocytoclastic vasculitis: here confluent purpura with ulceration is present. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 16.5 Leukocytoclastic vasculitis: this patient presented with bullous lesions which developed as a consequence of thrombosis with epidermal infarction. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.6 Leukocytoclastic vasculitis: nodular lesions. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.7 Leukocytoclastic vasculitis: in this patient, there are extensive ulceroinfarctive lesions. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.8 Leukocytoclastic vasculitis: close-up view of a hemorrhagic blister. By courtesy of the Institute of Dermatology, London, UK.
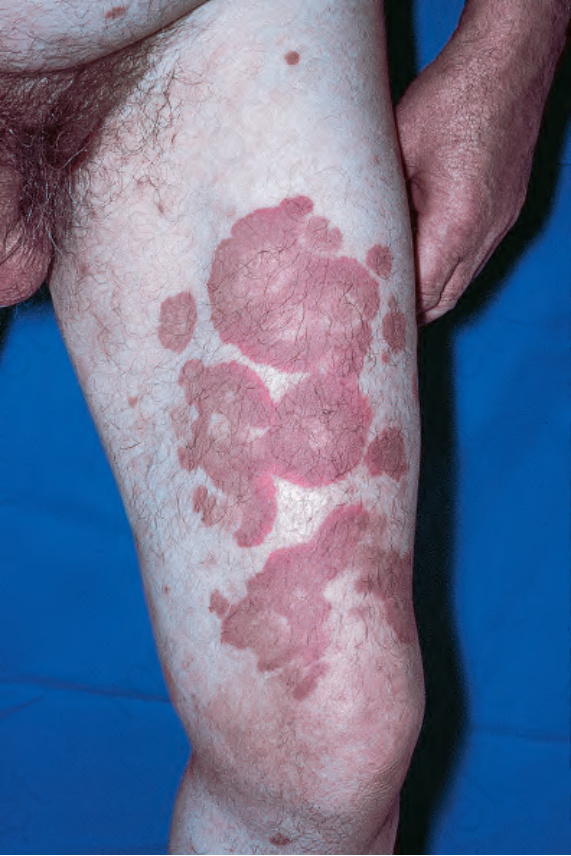
Fig. 16.11 Leukocytoclastic vasculitis: this patient has serological evidence of systemic lupus erythematosus.
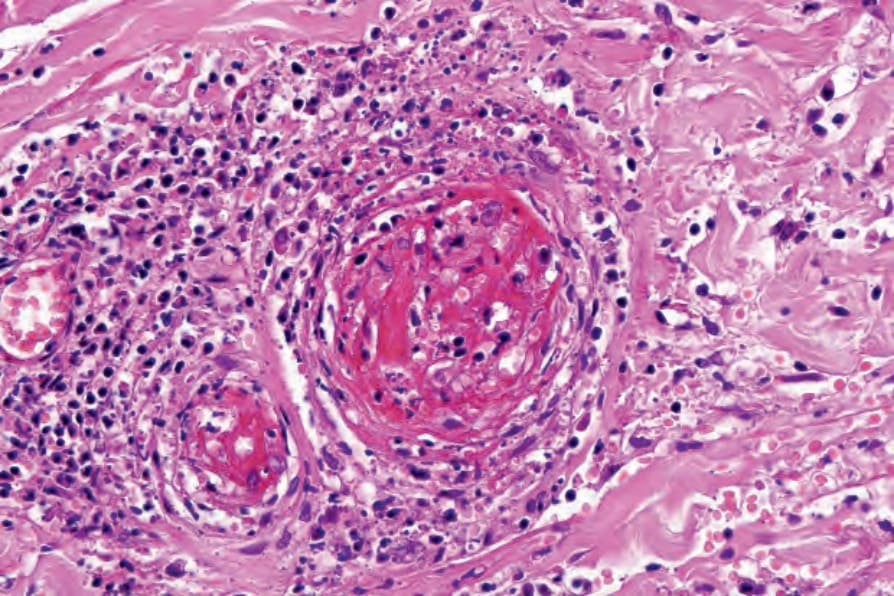
Fig. 16.15 Leukocytoclastic vasculitis: high-power view showing complete vessel wall destruction.
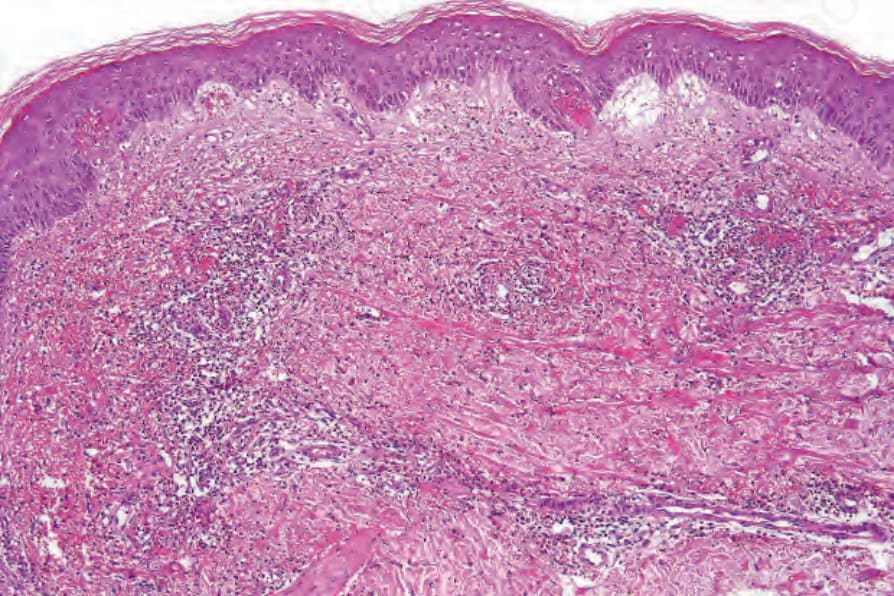
Fig. 16.18 Leukocytoclastic vasculitis: in this example, there is incipient subepidermal vesiculation.
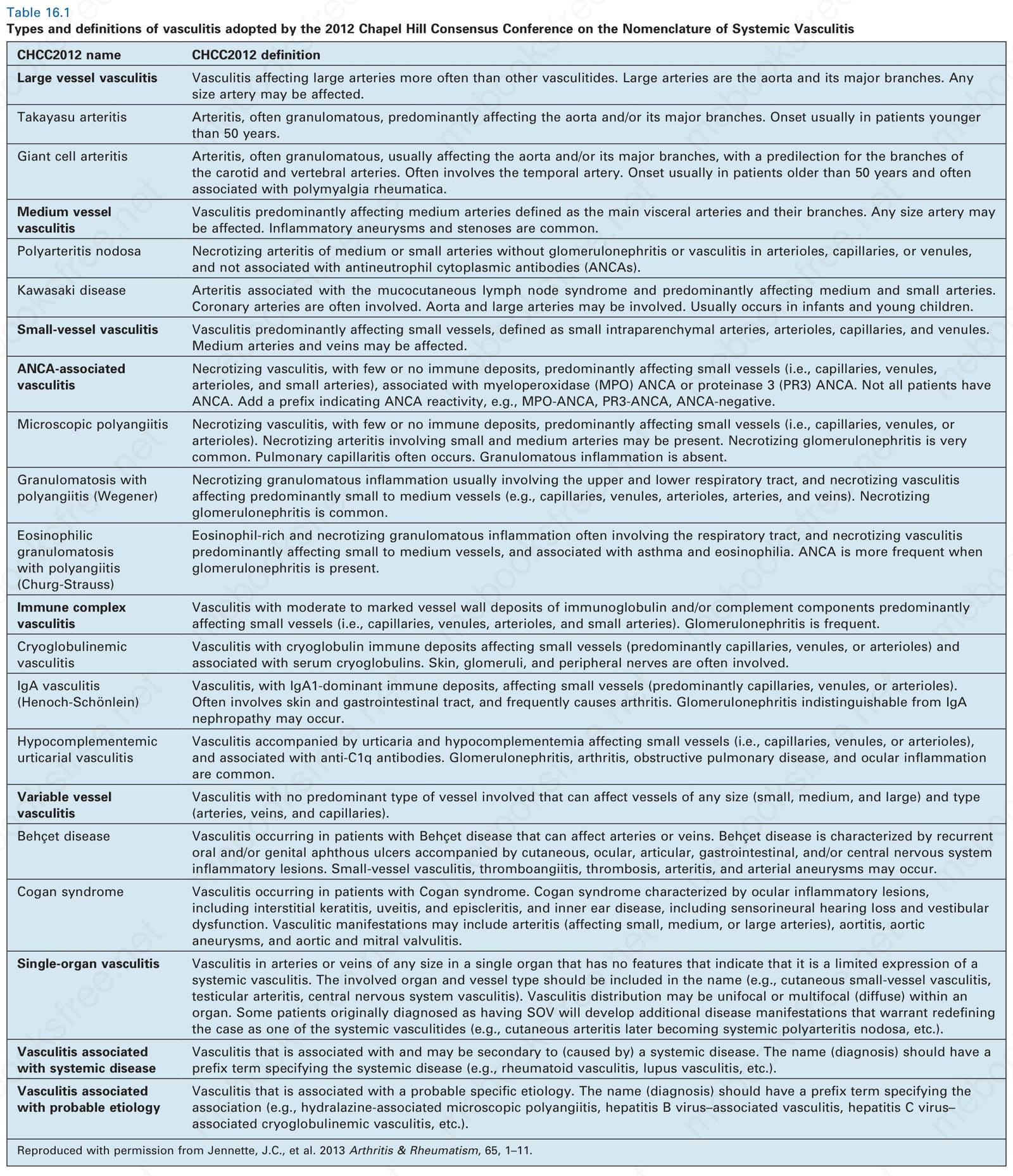
Table 16.1 Types and definitions of vasculitis adopted by the 2012 Chapel Hill Consensus Conference on the Nomenclature of Systemic Vasculitis
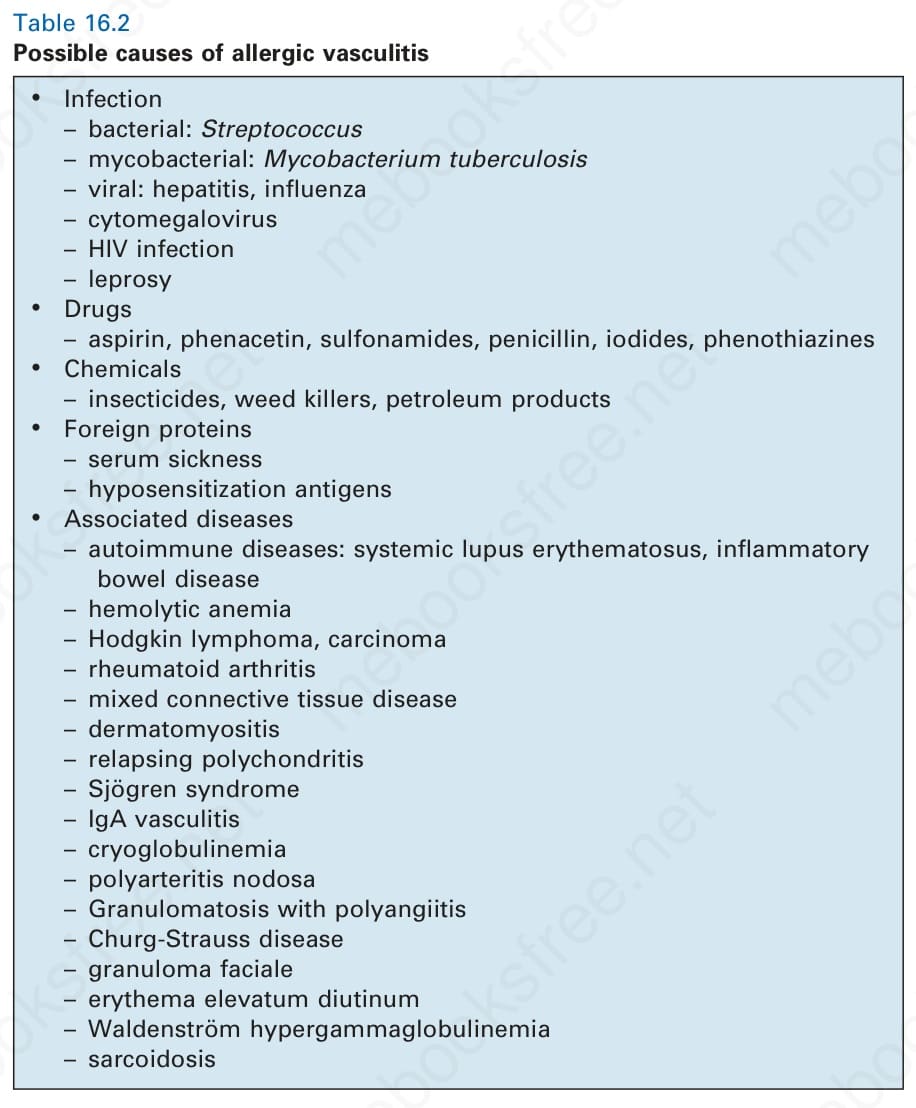
Table 16.2 Possible causes of allergic vasculitis
lesions measure from 1 mm to several centimeters in diameter. Occasionally, annular erythema multiforme-like lesions occur (Fig. 16.9). The lower legs are affected most often, but lesions can present at a wide variety of sites, including the buttocks, arms, feet, ankles, trunk, and face, particularly in more seriously affected patients (Figs 16.10 and 16.11). Lesions may be noted in the skin of dependent areas of bedridden patients, such as the back and buttocks. A frequent accompaniment is edema of the lower legs or ankles (Fig. 16.12). Patients either experience a single occurrence or develop frequent recurrences over months or years. The eruption often occurs in episodes at irregular intervals, each lasting 1–4 weeks. Lesions usually heal completely, although on occasions atrophic scars and hyperpigmentation may occur. Rarely, leukocytoclastic vasculitis shows an erythema gyratum repens gross morphology.20
In one study, drug therapy, often following an upper respiratory tract infection, was the inciting event in 45% of patients.22 Numerous drugs have been implicated as a trigger including nonsteroidal anti-inflammatory drugs (aspirin, ibuprofen, naproxen, phenylbutazone), phenytoin, quinidine, amiodarone, potassium iodide, allopurinol, sulfonamides, griseofulvin, penicillin, erythromycin, clindamycin, oxacillin, vancomycin, ofloxacin, clarithromycin, furosemide (frusemide), thiazides, cimetidine, omeprazole, gabapentin, orlistat, zidovudine, indinavir, efavirenz, lisinopril, sotalol, insulin, retinoids, propylthiouracil, thiouracil, mefloquine, methotrexate, azathioprine, sirolimus, granulocyte colony-stimulating factor, haloperidol,
718 Vascular diseases
cytarabine, erlotinib, rituximab, cinacalcet, famciclovir, rifampin, pyrazinamide, insulin aspart, metformin, gold, and disulfiram.2,23–65 Levamisole has been described as producing a vasculitis localized to the ears in children. 66,67 More recently, levamisole has been implicated in vasculitis and thrombotic vasculopathy related to cocaine abuse, discussed in more detail below.68–75 Localized leukocytoclastic vasculitis may occur at the site of interferon alpha injection.76,77
Collagen vascular disease (most often rheumatoid arthritis and lupus erythematosus) is commonly associated with leukocytoclastic vasculitis, 2,78 and in one study it was found in 21% of patients.2 The presence of leukocytoclastic vasculitis in a patient with dermatomyositis raises the possibility of associated malignancy.79–81
719 Leukocytoclastic vasculitis
Specific syndromes associated with leukocytoclastic vasculitis, such as urticarial vasculitis and Henoch-Schönlein purpura, are discussed under separate headings in this chapter.
Pathogenesis and histologic features Leukocytoclastic vasculitis is an immune complex-mediated disorder similar to the classic Arthus reaction.133 Immune complexes are deposited in the walls of small blood vessels.5 This is associated with activation of the complement cascade and the production of C5a (a neutrophil polymorph chemotactant). The resultant polymorph influx is associated with release of lysosomal enzymes, including elastases and collagenases, resulting in blood vessel wall damage, fibrin deposition, and the release of red blood cells (purpura) into the perivenular connective tissue. Thrombosis may ensue and, in particularly severe examples, epidermal ischemic damage results. Lesions are particularly seen on the lower legs because of hydrostasis and blood vessel flow sludging.5
Infection is also commonly associated with leukocytoclastic vasculitis, with bacterial, fungal, and viral infection all being implicated.82 Associated bacterial infections include streptococci, Klebsiella pneumoniae, Mycobacterium tuberculosis, and Mycoplasma pneumoniae.83–85 Systemic cat scratch disease presenting as leukocytoclastic vasculitis has been documented.86 Hepatitis C infection is a particularly frequent association. It should be noted that hepatitis C is also often associated with cryoglobulins (see section on cryoglobulinemia).87–91
Inflammatory bowel disease, both ulcerative colitis and Crohn disease, may be coupled with leukocytoclastic vasculitis.92–106 One study suggested that vasculitis was more commonly a complication of Crohn disease rather than ulcerative colitis.106 In some patients with inflammatory bowel disease, there is evidence that implicates treatment with tumor necrosis alpha inhibitors as the inciting factor.107–109 Further rare associations include sarcoidosis, α1-antitrypsin deficiency, cystic fibrosis, and the Wiskott-Aldrich syndrome.17,110,111
Evidence for an immune complex-mediated pathogenesis is convincing.1 Patients have been clinically proven to have high levels of circulating immune complexes, and these are shown to correlate with vasculitic lesions. Immunoglobulin and complement can be identified in vitro, by immunofluorescence or immunoperoxidase techniques, and in biopsies from blood vessel wall lesions less than 24 hours old (Fig. 16.13).134 Immune complexes can be identified ultrastructurally as clumps of electron-dense material, usually within the basement membrane between endothelial cells and pericytes of postcapillary venules. Examination of apparently uninvolved skin from patients with leukocytoclastic vasculitis sometimes shows immunoglobulin and complement within the walls of dermal blood vessels. If histamine is injected into uninvolved skin 3–4 hours previously, all the features of leukocytoclastic vasculitis are evident at biopsy, including neutrophil degeneration; this suggests that the immunoreactants are a cause rather than a consequence of the vasculitis.1
Physical exercise has also been related to the development of leukocytoclastic vasculitis. Outdoor activities in hot weather such as walking, running, golfing (golfer’s vasculitis), swimming, and dancing have especially been implicated and middle aged to elderly individuals are more frequently affected.111–115 In the setting of exercise-induced vasculitis, venous stasis may be a contributing factor.115 Leukocytoclastic vasculitis rarely represents a paraneoplastic manifestation of an underlying malignancy, especially leukemia and lymphoma.116 Hairy cell leukemia is particularly often associated with leukocytoclastic vasculitis but other forms of vasculitis may also be seen.117,118 In one study of 42 patients with hairy cell leukemia and vasculitis, 21 had leukocytoclastic vasculitis and 17 had polyarteritis nodosa.117 In addition, four patients had direct infiltration of vessel walls by leukemic cells (see also section on paraneoplastic vasculitis). Although uncommon, leukocytoclastic vasculitis may also be seen in patients with a variety of solid tumors including non-small cell carcinoma of lung, adenocarcinoma of breast, colon, prostate, and kidney, papillary thyroid carcinoma, thymoma, and chondrosarcoma.119–122
The findings of immunofluorescence studies vary according to the age of the lesion. Immunoglobulins have been described in up to 81% of patients.9 In early lesions, C3 and IgM predominate, in fully developed lesions there is predominance of fibrinogen and IgG, and in late lesions fibrinogen and C3 are detected.9
Some authors, noting that early lesions may contain abundant CD3+, CD4+, and CD1a+ cells, have suggested that cell-mediated immune mechanisms may also play a role in the pathogenesis of leukocytoclastic vasculitis.9 Consistent with this hypothesis is the demonstration of Langerhans cells in the late phase of vasculitis.135 Expression of 72 kD heat shock protein and the presence of gamma/delta T cells in patients with vasculitis
Leukocytoclastic vasculitis can be a manifestation of human immunodeficiency virus (HIV) infection.123,124 Unusual associations of this condition include the use of a nicotine patch, drug additives, sodium benzoate, protein A column pheresis, interleukin-12 receptor beta-1 deficiency, prolonged exercise, and as a complication of an infected hip prosthesis.125–131
Laboratory investigation may reveal an elevated erythrocyte sedimentation rate (ESR), proteinuria, or hematuria. In some idiopathic cases and in those associated with systemic disease (e.g., rheumatoid arthritis, systemic lupus erythematosus (SLE), and Sjögren syndrome), hypocomplementemia is sometimes evident.5 Urinalysis may reveal proteinuria or hematuria. Cryoglobulins have been found in up to 25% of patients.2 Perinuclear staining antineutrophil antibodies are present in about 20% of patients.2,132
The outcome of leukocytoclastic vasculitis is variable, ranging from a mild, self-limiting illness through to a serious, potentially fatal disorder due particularly to renal involvement.21 About 1.9% of patients die of systemic disease.2 Most patients have a benign outcome. An acute clinical course is seen in approximately 50% of patients.2,11 A chronic course or one characterized by relapses and remissions is seen in some patients.2 In one study of patients with hypersensitivity vasculitis, 54 did not require therapy, 26 were treated with nonsteroidal anti-inflammatory medications, and 14 required immunosuppressive agents, most often corticosteroids.22
720 Vascular diseases
associated with infection have led one group of authors to postulate that the cell-mediated immune response plays an important role in that subset.136
In leukocytoclastic vasculitis, it is the postcapillary venule and the capillary loops (and not the arteriole) which are primarily affected, usually within the superficial dermis (Figs 16.14 and 16.15). In severe cases, particularly those associated with malignancy or connective tissue disease, the inflammatory changes extend into the vasculature of the deep reticular dermis or even the subcutaneous fat.10 The histologic features are similar irrespective of the underlying etiology.
The histologic features of leukocytoclastic vasculitis are those of fibrinoid necrosis associated with endothelial cell swelling and infiltration of the blood vessel walls by neutrophils and conspicuous nuclear dust (Fig. 16.16).2,132,137,138 Variable numbers of mononuclear cells and eosinophils may be seen. In early lesions, nuclear dust is associated with a perivascular neutrophilic infiltrate but multiple tissue sections may be needed to identify fibrinoid vascular changes. The former features, even without unequivocal fibrinoid change, are suggestive of an evolving leukocytoclastic vasculitis. In late lesions lymphocytes may be more prominent than neutrophils.
Intravascular thrombi and ischemic necrosis of the overlying epidermis (often with bullae formation) may sometimes be seen (Figs 16.17–16.19). Occasionally, one may encounter intradermal or subepidermal pustules.

Fig. 16.9 Leukocytoclastic vasculitis: these urticarial lesions on the back of the arm resemble those of erythema multiforme. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 16.10 Leukocytoclastic vasculitis: lesions may be widely disseminated in severely affected patients. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 16.12 Leukocytoclastic vasculitis: in addition to the typical maculopapular eruption there is marked swelling of the legs. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
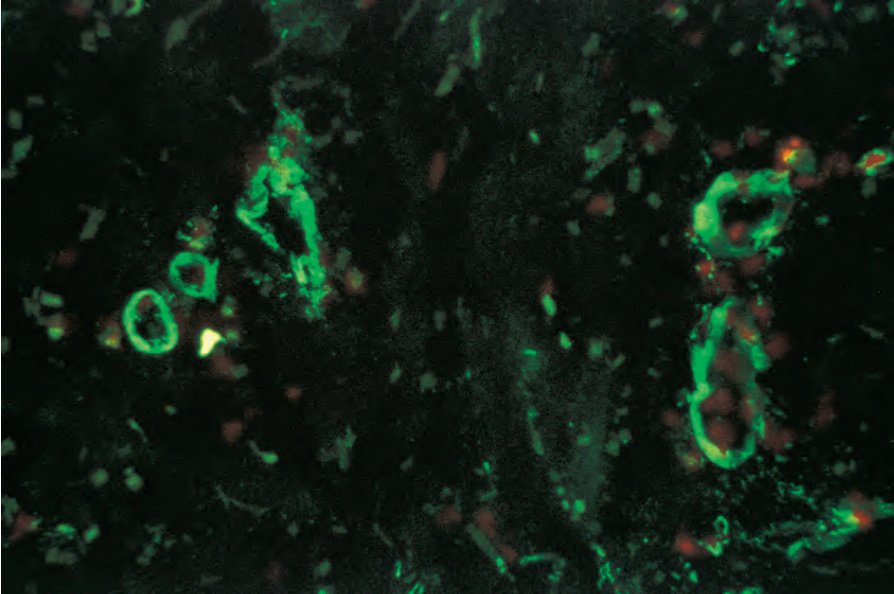
Fig. 16.13 Leukocytoclastic vasculitis: IgM is present in the blood vessel walls (direct immunofluorescence). By courtesy of B. Bhogal, FIMLS, Institute of Dermatology, London, UK.
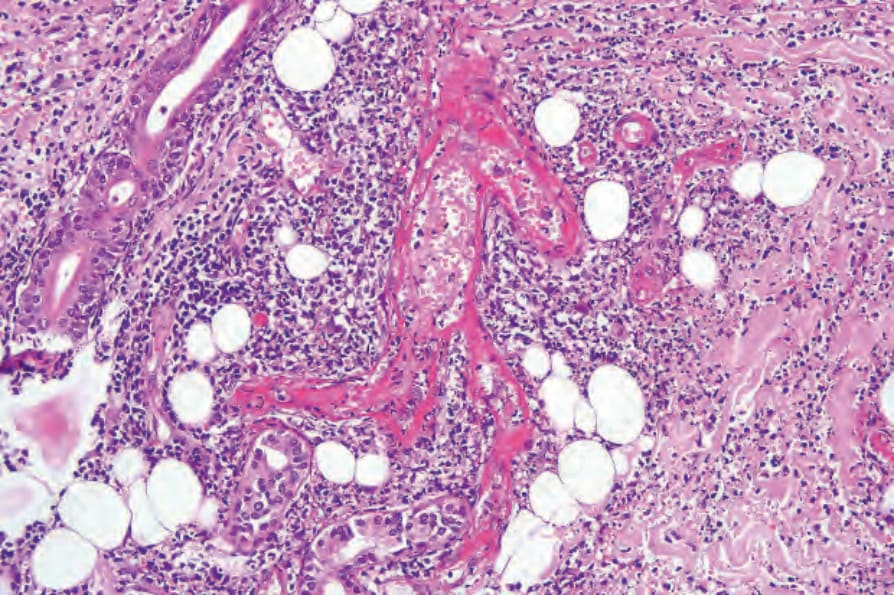
Fig. 16.14 Leukocytoclastic vasculitis: the blood vessels show florid fibrinoid necrosis and intense inflammation.
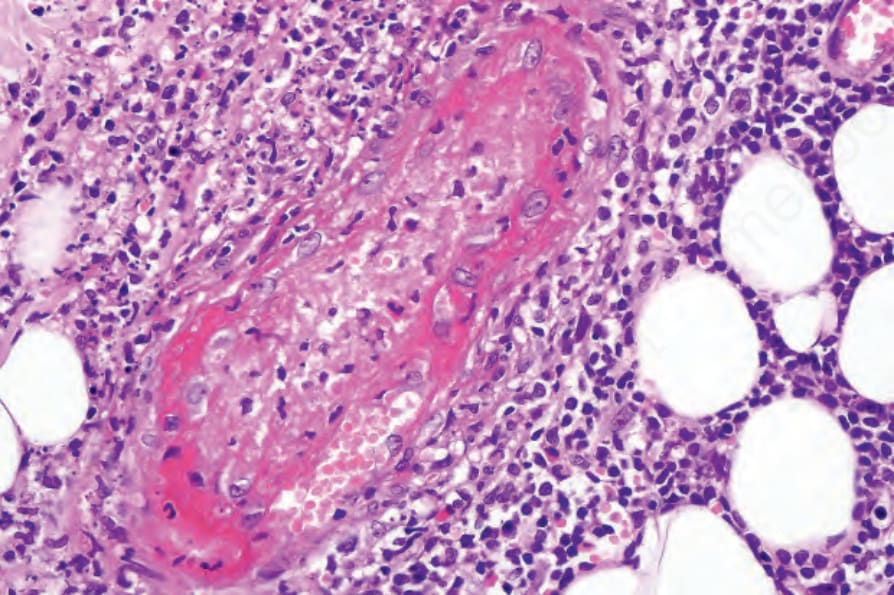
Fig. 16.16 Leukocytoclastic vasculitis: high-power view showing fibrinoid necrosis and a mixed inflammatory cell infiltrate composed of neutrophils, eosinophils, and lymphocytes. There is marked leukocytoclasis (karyorrhexis, nuclear dust).
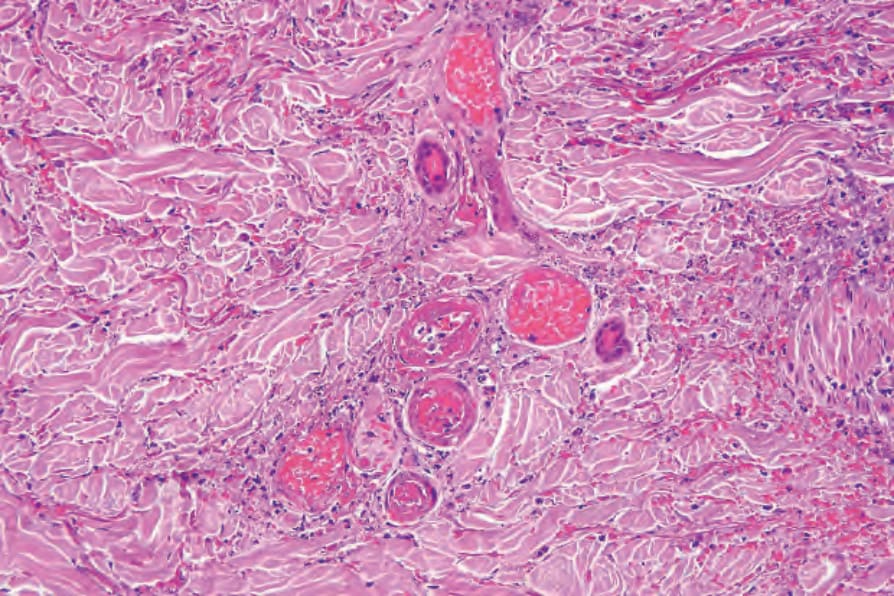
Fig. 16.17 Leukocytoclastic vasculitis: vascular thrombosis as seen in this field is not uncommon.
721 IgA vasculitis (Henoch-Schönlein purpura)
by myriad underlying disorders. Furthermore, leukocytoclastic vasculitis is frequently encountered in association with other forms of vasculitis. For example, it is much more commonly encountered in patients with granulomatosis with polyangiitis than granulomatous vasculitis. Therefore, a biopsy showing leukocytoclastic vasculitis does not exclude diseases that may be associated with other forms of vasculitis. Sometimes it coexists with a large-vessel vasculitis. An inadequate biopsy that does not include deep dermis and subcutaneous tissue containing large vessels can produce misleading results. The presence of leukocytoclastic vasculitis in a superficial biopsy does not exclude an associated large-vessel vasculitis; therefore the report of a superficial biopsy from a patient suspected of having large-vessel vasculitis should comment on the lack of larger vessels for evaluation.
Sweet syndrome may resemble leukocytoclastic vasculitis; however, the presence of a diffuse (rather than predominantly perivascular) neutrophilic infiltrate without fibrinoid vascular change or necrosis favors the former condition.