Prurigo pigmentosa
Prurigo pigmentosa
Clinical features Prurigo pigmentosa is a distinctive inflammatory dermatosis first described by Nagashima in 1978.1–6 Most cases occur in Japanese patients although the disease appears to have a wider distribution and may have been underdiagnosed in the past.6–12 Most cases present in young adults and there is a predilection for females. Cases in small children are very uncommon. The disease also seems to have a predilection for patients in Sicily, Turkey, and Iran.13–16 It presents as very pruritic urticarial papules, papulovesicles, and vesicles in a reticular pattern on the back, neck, and chest.17,18 (Fig. 15.68) Pustules are rarely seen.19 Involvement of the lower trunk may be seen and lesions on the face are exceptional.20,21 Lesions last for a few days and heal, leaving a reticulate hyperpigmentation (Fig. 15.69). Recurrences are frequent. It most commonly occurs in the spring and summer. Unilateral
Pathogenesis and histologic features The pathogenesis of the disease is as yet unknown although some cases may be induced by ketosis or allergic contact dermatitis to chromium and nickel.24–29,33,34,46 Antinuclear antibodies have been reported in some patients but it is not clear whether this has pathogenetic importance or represents a coincidence.47 The detection of Borrelia garinii and Borrelia afzelii in skin specimens with serological evidence of Borrelia infection in three reported cases has raised the possibility that this is an unusual manifestation of the disease.48 It has also been suggested that the disease is an inflammatory variant of confluent and reticulated papillomatosis.49
Early lesions show a superficial perivascular inflammatory cell infiltrate composed of neutrophils (Fig. 15.70). In these early lesions, dermatitis
713 Prurigo pigmentosa
herpetiformis-like changes have been described.50 As the disease progresses, neutrophils may be seen in the papillary dermis and extending into the epidermis. This is associated with spongiosis, ballooning, and scattered necrotic keratinocytes.6,51 As the lesions evolve, epidermal neutrophilic microabscesses may be found and dermal eosinophils and lymphocytes are seen (Fig. 15.71). A focal lichenoid pattern may be present (Fig. 15.72). Hydropic degeneration of basal cells is very focal, and colloid bodies are not usually detected. Microvesicle formation is present in some cases but subepidermal blister formation is rare.51 Epidermal acanthosis and hyperkeratosis are features in late stages along with pigment incontinence and melanophages (Fig. 15.73). Follicular involvement in the form of bacterial colonies in the hair follicle, folliculitis, and perifolliculitis has been reported in 78% in a series of cases.52
Access ExpertConsult.com for the complete list of references
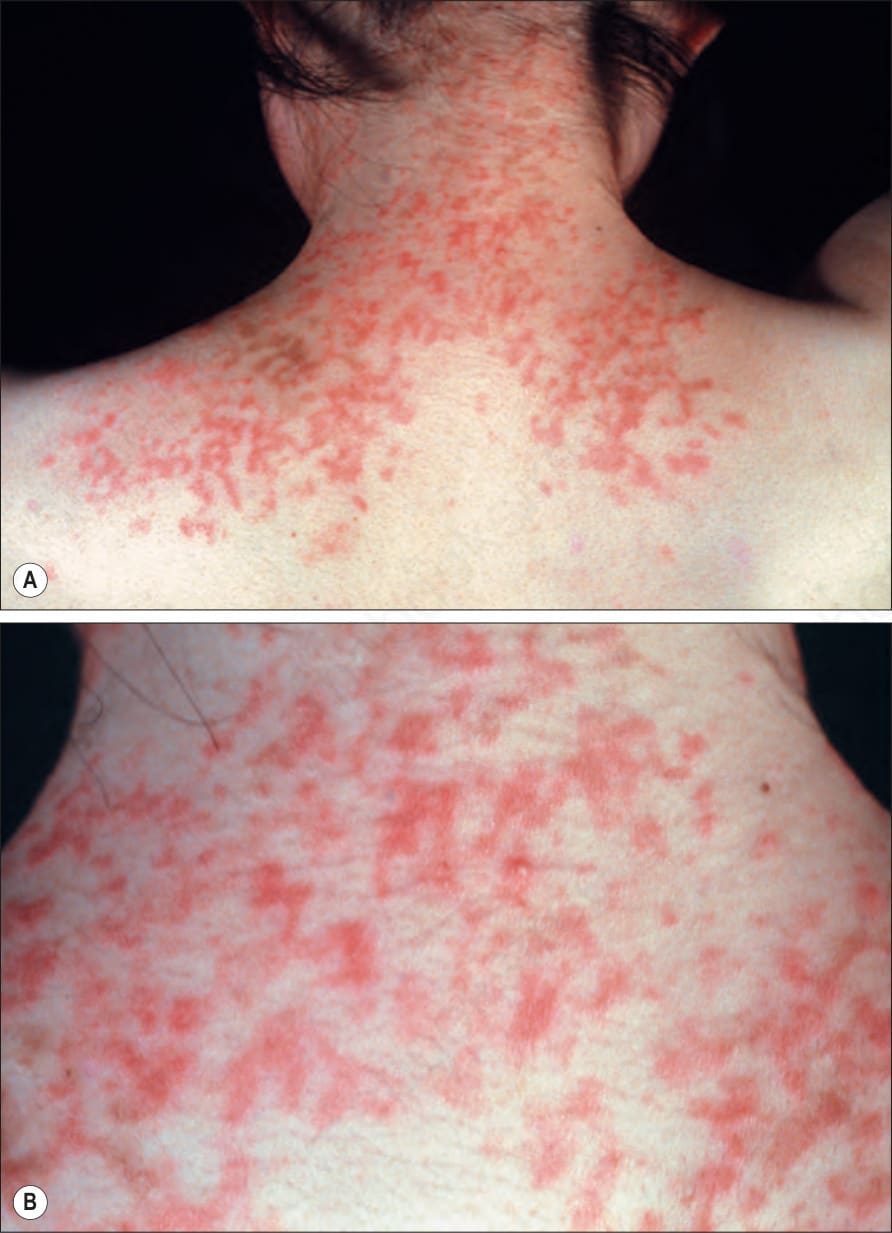
Fig. 15.68 Prurigo pigmentosa: reticulate urticarial papules on (A) the upper back and (B) the neck. By courtesy of the Institute of Dermatology, London, UK.

Fig. 15.69 Prurigo pigmentosa: late lesions with typical reticulate hyperpigmentation. By courtesy of Drs. Chao-Kai Hsu and Prof. Julia Yu-Yun Lee, Tainan, Taiwan.
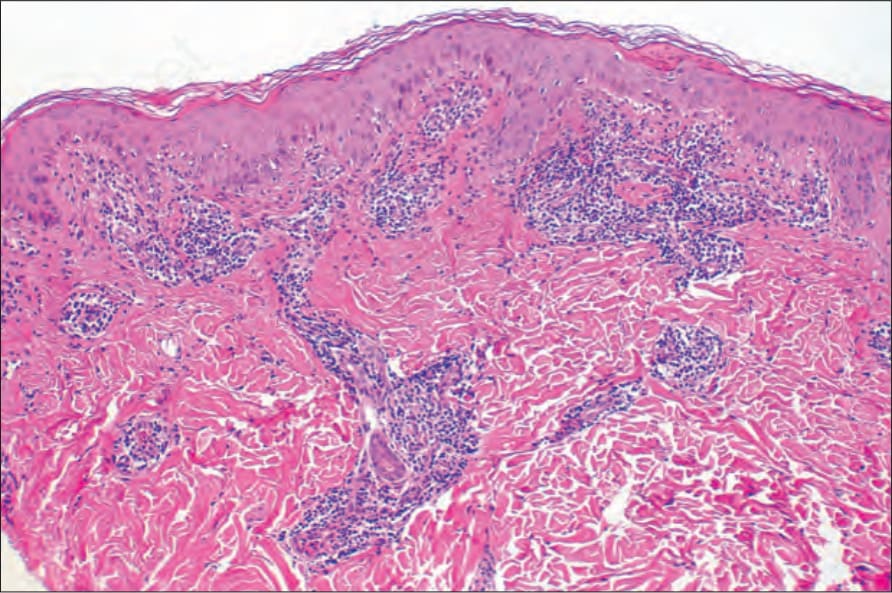
Fig. 15.70 Prurigo pigmentosa: superficial perivascular infiltrate in an established lesion.
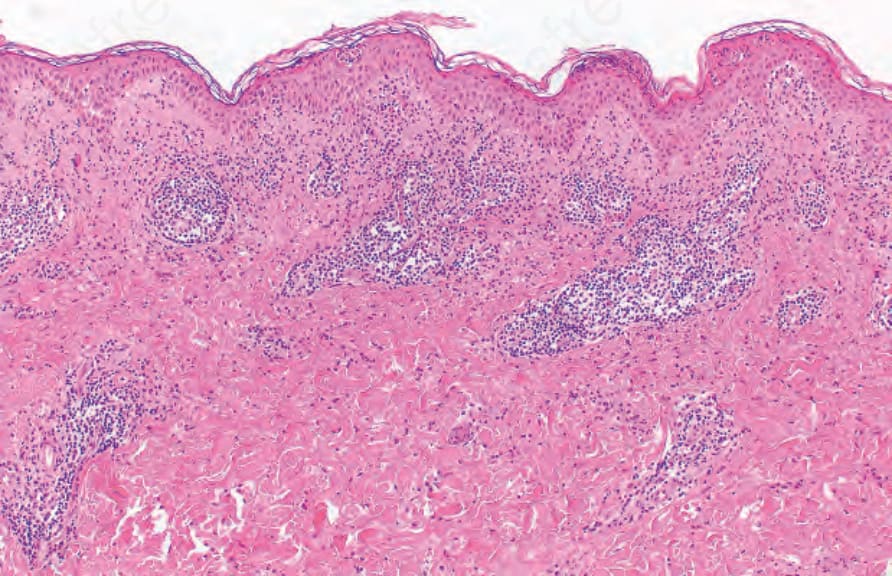
Fig. 15.71 Prurigo Pigmentosa: as the lesion evolves, there is exocytosis of neutrophils into the epidermis, with spongiosis and necrotic keratinocytes.
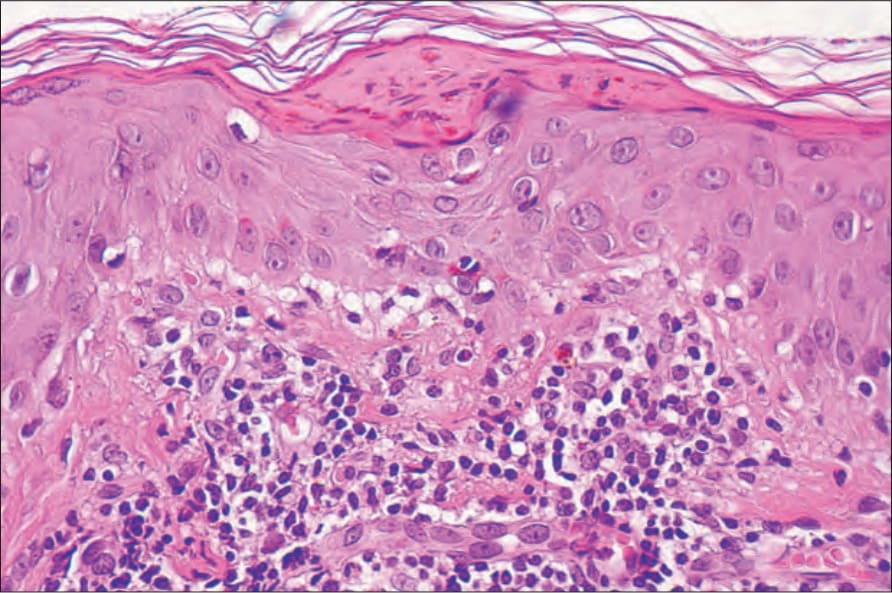
Fig. 15.72 Prurigo pigmentosa: focal lichenoid change combined with spongiosis and some exocytosis of lymphocytes. Neutrophils have been replaced by lymphocytes and histiocytes.
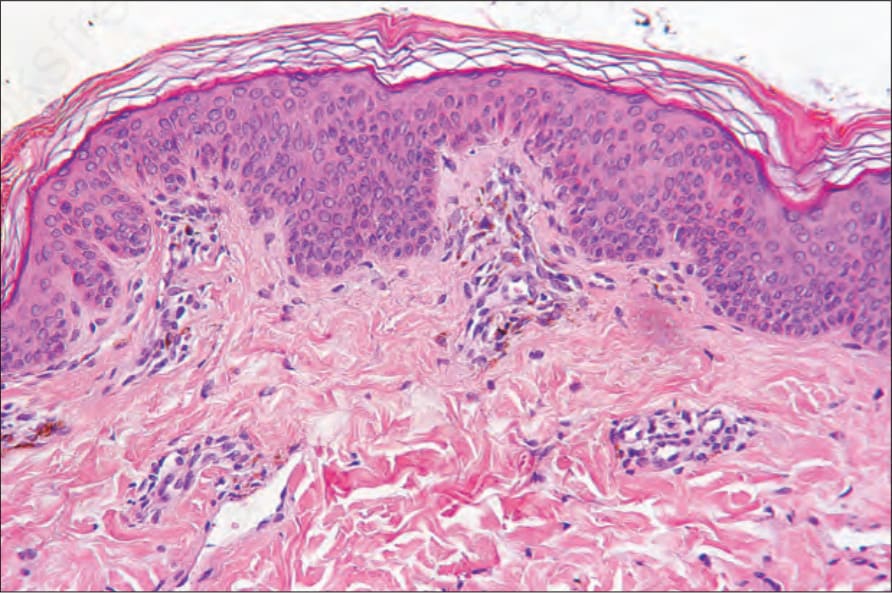
Fig. 15.73 Prurigo pigmentosa, late lesion: mild acanthosis with hyperkeratosis and pigment incontinence.