Hidradenitis suppurativa
Hidradenitis suppurativa
Clinical features Hidradenitis suppurativa (acne inversa, apocrine acne) is a common disease.1–3 The prevalence varies from < 1.0% to 4%.4–7
It is a chronic relapsing suppurative inflammation of regions where apocrine glands occur, i.e., the axilla, inguinal folds, perineum, genitalia, and periareolar region (Fig. 15.63).7,8 It usually occurs postpubertally in both sexes, more commonly in women.5 Karl Marx was famously afflicted.1–12 The disease is seen most frequently in young adults, although its first presentation may be in older individuals and also before puberty.13–15 In
710 Neutrophilic and eosinophilic dermatoses
prepubertal children, there is frequently a family history.15 Initially, there is a firm painful nodule in the groin or axilla. The nodule can involute slowly or else discharge pus through the skin; the discharge of pus is not copious, but is chronic and often malodorous. In the late stages, a complex interconnecting system of sinuses extends deeply into the dermis and subcutaneous fat with extensive dense fibrosis (Fig. 15.64).16
commonly in black males, and it is very rarely familial.34 Radical surgery is often the only satisfactory means of terminating the process. All the diseases in the follicular occlusion triad can occasionally be complicated by progression to cellulitis and septicemia. Squamous carcinoma (including the verrucous variant) is a rare and late additional complication.35–42 As with Marjolin ulcer–cancer, the carcinomas are capable of aggressive invasion and metastasis (50%) and are generally associated with a poor prognosis.17 Such tumors arise most frequently on the buttocks and are more often seen in males.38 Hidradenitis has been shown to be associated with systemic granulomatous lesions, in particular, Crohn disease.19,22,43–45 An association with spondyloarthropathy, Dowling-Degos disease, and lithium therapy has also been documented.22,46–48
Axillary lesions are more common in women and genitoinguinal lesions are more common in men. Changes may be confined to one region or occur in both, but the axillary region is involved in over 70% of cases.17 Some reports have attached etiological importance to axillary shaving and the use of deodorants, but this is not generally accepted.17,18 Obesity, metabolic syndrome, diabetes mellitus, inflammatory bowel disease, arthritis, and smoking are associated.6,19–22 In one study, nearly 90% of German patients were smokers (expected prevalence rate 27%).13 Whether cessation of smoking improves the course of the disease is unknown.23 Patients with the hidradenitis suppurativa appear to be at increased risk of developing nonmelanoma skin cancer, but it is usually late onset (~25 years) and may be due to the complications of a chronic inflammatory state.22,24
The lesions are clearly maintained by bacterial infection as various organisms are often grown.25 Symptomatic improvement can be achieved with long-term antibiotics. Perineal lesions are often severe and complicated by abscesses, fistulae, and draining sinus tracts.17
Treatment of this disease is difficult due to its chronic relapsing nature. Surgery is often used to remove affected areas, but the cure rate in some studies is very low.49 Nevertheless, occasional patients are satisfied with the relief of symptoms, albeit temporary, afforded by surgery.49 Other studies have shown a low recurrence rate following wide excision.50,51 Early surgical treatment appears to increase the chance of success.52 Recently, new-generation immunosuppressive agents and biological medications have shown some efficacy.53,54 Hormonal regulation has also been employed with more limited success.55,56
Lesions are also rarely seen on the malar region of the face and even on the eyelids (glands of Moll), sites with modified apocrine glands.
Hidradenitis suppurativa can be present in association with conditions which are said to be pathologically similar, namely, acne conglobata and dissecting folliculitis of the scalp. These three conditions have been referred to collectively as the ‘follicular occlusion triad’.26 Any one condition, however, may occur separately. Acne conglobata, an extremely severe nodulocystic variant of acne, occurs extensively on the trunk, buttocks, and limbs with predilection for males.27 The disease has been described in association with HIV and following pregnancy.28,29 Dissecting folliculitis (folliculitis capitis abscedens et suffodiens) is centered on the vertex of the scalp and is characterized by boggy tender lesions that tend to become confluent with formation of draining sinuses and suppuration.30–33 The disease presents more
Pathogenesis and histologic features The pathogenesis of hidradenitis suppurativa remains poorly understood.57–62 It has generally been thought that the earliest lesion is an acute inflammatory process involving the apocrine duct and gland, which extends into the surrounding connective tissue with subsequent abscess and sinus formation (Fig. 15.65).57 Other authors, however, believe that eccrine hidradenitis is more commonly found than apocrine involvement, and yet others think that the primary event is follicular obstruction.38,59 Some data suggest overactivation of the innate immune system, but a deeper underlying cause remains elusive.25,63,64
The provocation for the initial ‘apocrinitis’ is believed by some to be keratin occlusion of the corresponding hair follicle. Certainly, keratin plugging of follicles and sinuses and inflammation in and around the hair follicle
are regularly seen.58 In one study, follicular occlusion was present in all of 118 specimens examined in patients with disease duration that ranged from as little as 1 month to many years.60 The anatomic distribution of the lesions also supports the concept of an underlying apocrine gland defect. The condition has some similarity to Fox-Fordyce disease, which is more convincingly associated with an inflammatory process of the apocrine duct. Fox-Fordyce disease has the same sex predilection, age incidence, and anatomic distribution, and it, too, is alleviated by pregnancy. Interestingly, some cases of Fox-Fordyce disease have been reported to progress to hidradenitis suppurativa.
711 Hidradenitis suppurativa
The other members of the follicular occlusion triad – acne conglobata and dissecting folliculitis – are both clearly associated with keratin plugging.
There is no doubt that the main symptoms and chronic disability are related to the sinuses and fibrosis; these are largely due to the chronic secondary infection, since injection of sterile apocrine sweat into tissues does not induce an inflammatory response.
Organisms that may be found include Staphylococcus aureus, Streptococcus viridans, Escherichia coli, Proteus mirabilis, Klebsiella spp., Pseudomonas aeruginosa, Streptococcus milleri, and anaerobic organisms. Coagulase-negative S. aureus is the most common bacterium isolated from the depth of the lesions.25,65 Anaerobic organisms are responsible for the offensive smell, which can be a major problem for the patient. Generally, no immune deficiency is detectable, but there have been occasional reports of a functional neutrophil deficiency.
A
In considering the pathogenesis of this condition, it must also be noted that some cases clearly develop as an autosomal dominantly inherited tendency.66,67 Others have no suggestion of familial incidence.
The disease has been simulated in 3 of 12 normal volunteers by occlusion of axillary skin with atropine tape following depilation.68 The latter in itself could be expected to produce some pathology, which is clearly not seen in the normal individual. The absence of lesions in 75% of these volunteers shows at least that there is some variation in susceptibility to developing the disease. This experimental induction of the disease has not been repeated.
In a study of 42 women with hidradenitis suppurativa, the authors noted premenstrual exacerbation of symptoms in two-thirds of patients and over one-third of patients reported menstrual irregularities.69 In this same study, testosterone and free androgen index were higher compared with control patients.69 In contrast, another study was not able to correlate hyperandrogenism and development of hidradenitis in women.9,70 Pregnancy may relieve the symptoms of the disease.
B
In summary, the precise pathogenesis of hidradenitis suppurativa is not well understood. It seems likely, however, that while many patients have a tendency to follicular occlusion with resultant acne-like lesions, some individuals show an additional, occasionally inherited, tendency for follicular obstruction to cause, or be associated with, inflammation of the apocrine duct. With the additional occlusive effects of obesity and secondary infection, often by mixed organisms, there is a resultant florid destructive folliculitis centered on, or also involving, the apocrine glands. The secondary bacterial infection perpetuates the chronic inflammatory and scarring nature of the process. A defect in the immune system would be expected to exacerbate this vicious circle, but no consistent abnormality has yet been identified.71,72 The changes with pregnancy and menstrual cycle can be attributed to the hormonal effects on the apocrine gland and do not appear to be of primary importance.
Biopsies of established hidradenitis suppurativa show sinus tracts with marked suppuration and frank abscess formation. The sinus tracts are lined by a mixture of granulation tissue and squamous epithelium (Figs 15.66 and 15.67). The latter extends from the associated follicular epithelium. These inflammatory sinus tracts usually contain desquamated keratin and sometimes hair shafts, and are surrounded by dense fibrosis.60 The suppuration may extend into adjacent connective tissue where there can also be a chronic inflammatory infiltrate frequently including histiocytes and giant cells that are sometimes related to keratin fragments. At this stage, apocrine glands are conspicuously absent in the scarred and inflamed area, although adjacent apocrine glands often appear quite normal. Although some authors have emphasized the presence of acute inflammation of apocrine glands, in our experience, this is an uncommon finding in routine surgical specimens.
712 Neutrophilic and eosinophilic dermatoses
A
B
Others have also found primary inflammation of apocrine glands in only a minority of specimens.59,73
Differential diagnosis The main differential diagnoses are primary infection, a response to a ruptured epidermal inclusion cyst, or wounds. Clinical correlation and special stains for microorganisms are necessary to establish the correct diagnosis.
or segmental cases are exceptional.22,23 Associations with diabetes mellitus, ketosis, anorexia nervosa, bismuth, and allergic contact dermatitis to chromium and nickel have been documented.24–34 Rare associations with an atopic diathesis, pregnancy and primary biliary cirrhosis, Sjögren disease, H. pylori infection, after bariatric surgery, and in a pregnant woman with hyperemesis gravidarum have also been reported.35–41 H. pylori organisms have been identified in a dilated hair follicle of an affected patient.42 A prurigo pigmentosa-like rash has been reported in a case of adult-onset Still disease.43,44 A case in white monozygotic twins has been described.45
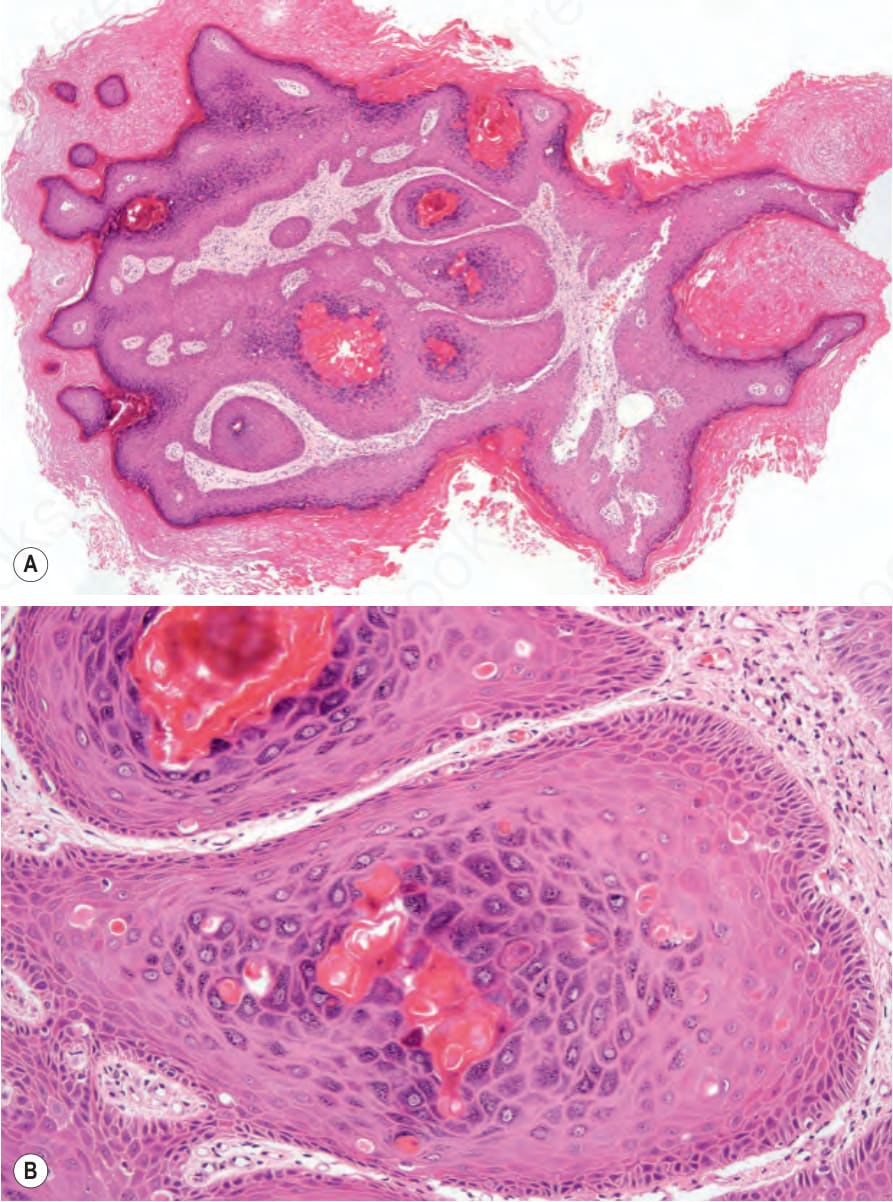
Fig. 15.63 (A, B) Incontinentia pigmenti: verrucous stage showing massive hyperkeratosis, papillomatosis, acanthosis, and numerous dyskeratotic cells.

Fig. 15.64 Hidradenitis suppurativa: early lesion presenting as an erythematous nodule discharging clear fluid. The axilla is a commonly affected site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 15.65 Hidradenitis suppurativa: in this very severe example, there is marked scarring and numerous sinuses are present. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 15.66 (A, B) Hidradenitis suppurativa: early lesion showing acute inflammation involving the apocrine gland.
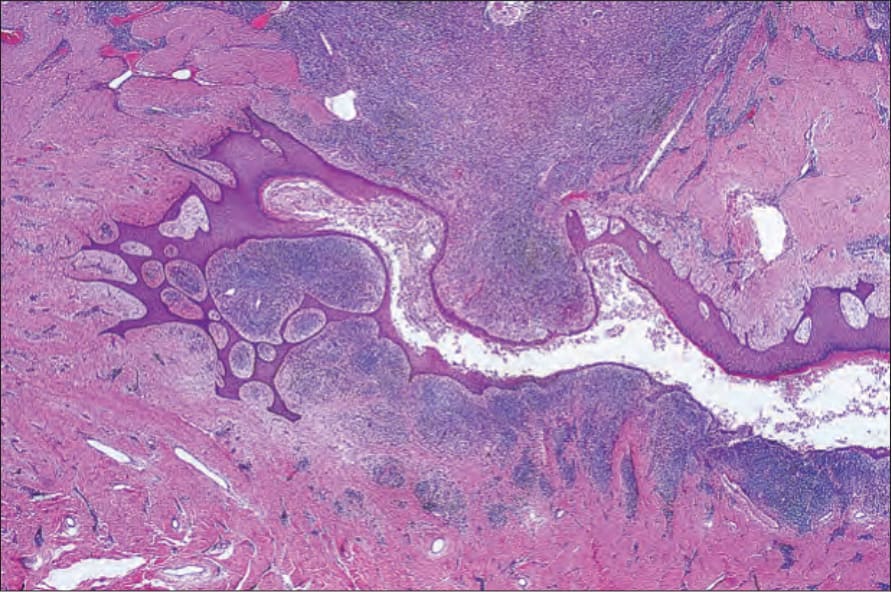
Fig. 15.67 Hidradenitis suppurativa: the sinuses are lined by stratified squamous epithelium and surrounded by fibrosis and inflammation.
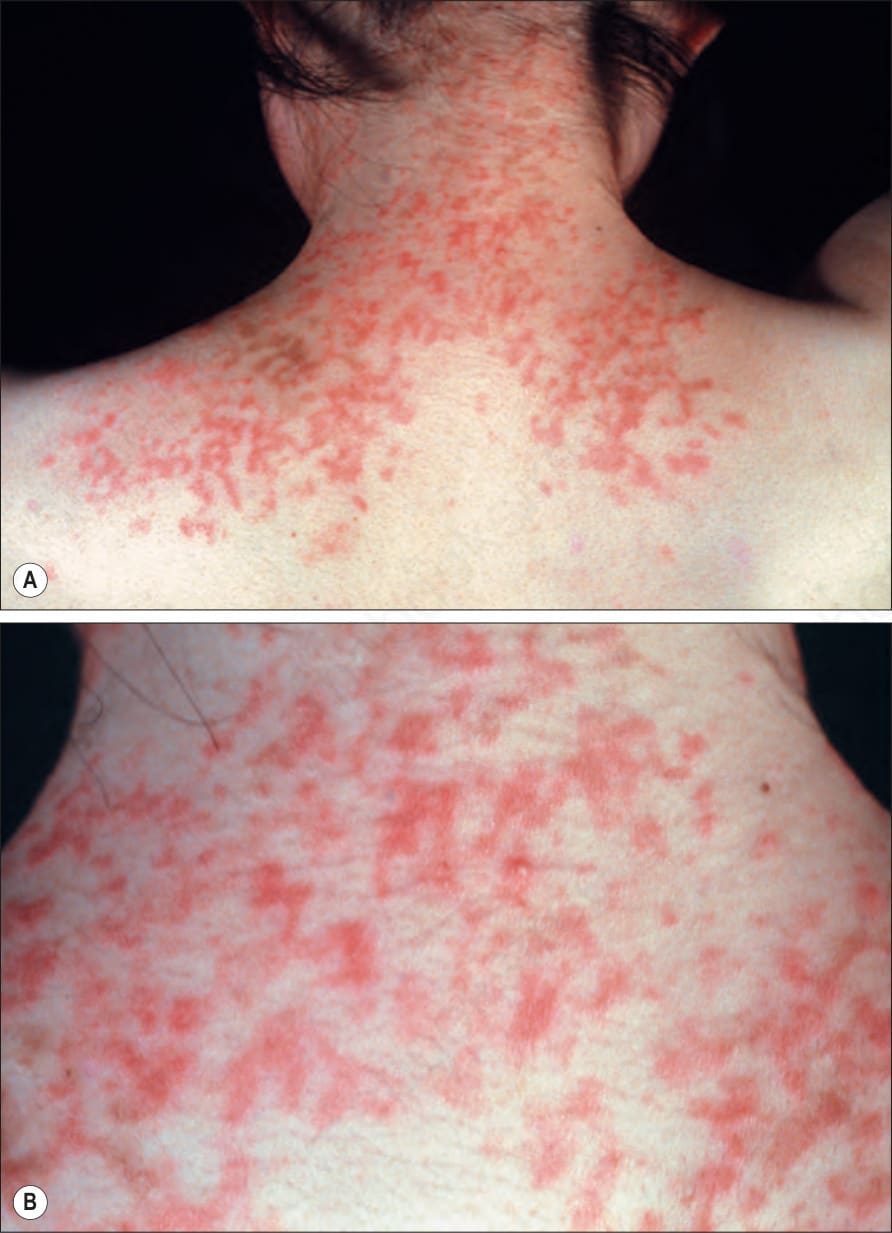
Fig. 15.68 Prurigo pigmentosa: reticulate urticarial papules on (A) the upper back and (B) the neck. By courtesy of the Institute of Dermatology, London, UK.

Fig. 15.69 Prurigo pigmentosa: late lesions with typical reticulate hyperpigmentation. By courtesy of Drs. Chao-Kai Hsu and Prof. Julia Yu-Yun Lee, Tainan, Taiwan.
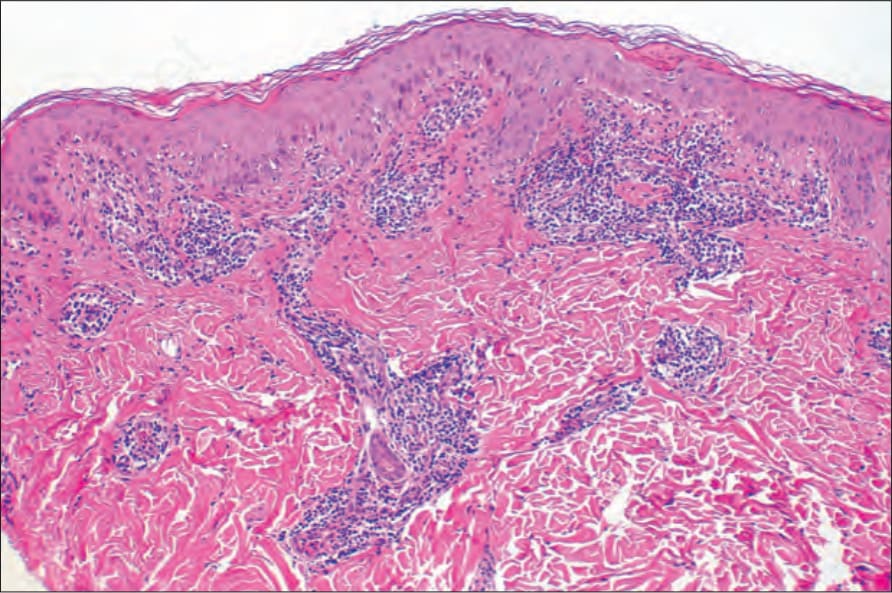
Fig. 15.70 Prurigo pigmentosa: superficial perivascular infiltrate in an established lesion.