Neutrophilic urticarial dermatosis
Neutrophilic urticarial dermatosis
Clinical features Neutrophilic urticarial dermatosis represents a particular cutaneous manifestation that may be seen in a variety of autoinflammatory disorders, including Schnitzler syndrome, Still disease, cryopyrin-associated periodic syndrome, SLE, rheumatoid arthritis, Sjögren syndrome, and other autoimmune diseases, as well as IgA monoclonal gammopathy and IgA myeloma.1–14 Clinically, patients present with present with variably pruritic, pale erythematous macules, papules, or plaques that resolve within 24–72 hours (Fig. 15.46).1,4
B
common in cryopyrin-associated periodic syndrome and IL-17-positve neutrophils are not seen in cryopyrin-associated periodic syndrome, indicative of multiple pathways to a common cutaneous and histologic presentation.15
Microscopically, neutrophilic urticarial dermatosis is associated with a dermal infiltrate of neutrophils. The infiltrate has both a perivascular and interstitial pattern and can be relatively mild to dense, mimicking Sweet syndrome (Fig. 15.47).1,4,16 Similar to Sweet syndrome, leukocytoclasis in the absence of vasculitis is common. Necrobiotic collagen bundles are sometimes present and the neutrophils can intercalate between collagen bundles in a manner similar to metastatic breast carcinoma (Fig. 15.48). The neutrophils may extend into the epithelium of the epidermis or adnexal structures, and this neutrophilic epitheliotropism is relatively sensitive and specific for neutrophilic urticarial dermatosis.16
Pathogenesis and histologic features The pathogenesis is incompletely understood and, given the multiple different disease associations, likely multifactorial. The pathogenesis, while incompletely understood, involves the proinflammatory effects of IL-β and IL-17. In cryopyrin-associated periodic syndrome, there is a mutation in NLRP3 (NOD-like receptor 3) that results in increased IL-β production and recruitment of neutrophils.10,12 A defined gene mutation is not known in Schnitzler syndrome, but cutaneous mast cells express IL-β and neutrophils in the dermis express IL-17.15 Interestingly, IL-β positive mast cells are less
Differential diagnosis The differential diagnosis includes Sweet syndrome, urticaria, leukocytoclastic vasculitis, and cellulitis. Sweet syndrome is clinically different with more indurated plaques and nodules and prominent dermal edema. Conventional urticaria usually has eosinophils associated with the infiltrate. Leukocytoclastic vasculitis has damage to the vascular walls, a feature not seen in
703 Hypereosinophilic syndrome
arthralgia, hepatosplenomegaly, basal ganglia calcifications, chondritis of the ear and nose, aseptic meningitis, and conjunctivitis and episcleritis.1–3
Pathogenesis and histologic features The pattern of transmission of the disease suggests that it is an autosomal recessive condition. Mutations in PSMB8 have been documented in most patients. This gene encodes many of the components of proteasomes, and alterations in these components lead to malfunction of proteasomes with accumulation of protein waste products in the cells.4–6 It appears that these patients also have a unique dysregulation of the IFN signaling pathway that contributes to many manifestations of the disease.7
Histologically, a prominent perivascular and interstitial cell infiltrate that may extend into the subcutaneous tissue, is seen. The infiltrate consists mainly of large mononuclear cells with pale cytoplasm, vesicular bean-shaped or oval vesicular nuclei, and a small nucleolus. These cells resemble those seen in leukemia and cutaneous infiltrates of myelodysplastic syndrome. Mitotic activity is present, and in the background there are neutrophils sometimes with nuclear dust, eosinophils, and lymphocytes.1,8 By immunohistochemistry, the large cells are positive for KP1 (CD68), lysozyme, CD45, and myeloperoxidase.1,8
Differential diagnosis In view of the presence of immature myelo-monocytic cells, distinction from leukemia cutis, the cutaneous infiltrates of myelodysplastic syndrome, and histiocytic Sweet syndrome may be difficult. Close clinicopathological correlation is critical as patients with CANDLE do not develop or have leukemia or myeolodysplastic syndrome, and histiocytic Sweet syndrome does not tend to occur early in life.

Fig. 15.46 Urticarial eruption in patient with Schnitzler syndrome involving the back (A) and arms (B). By courtesy of Dr. Anthony P. Fernandez, Cleveland Clinic, Cleveland, USA.
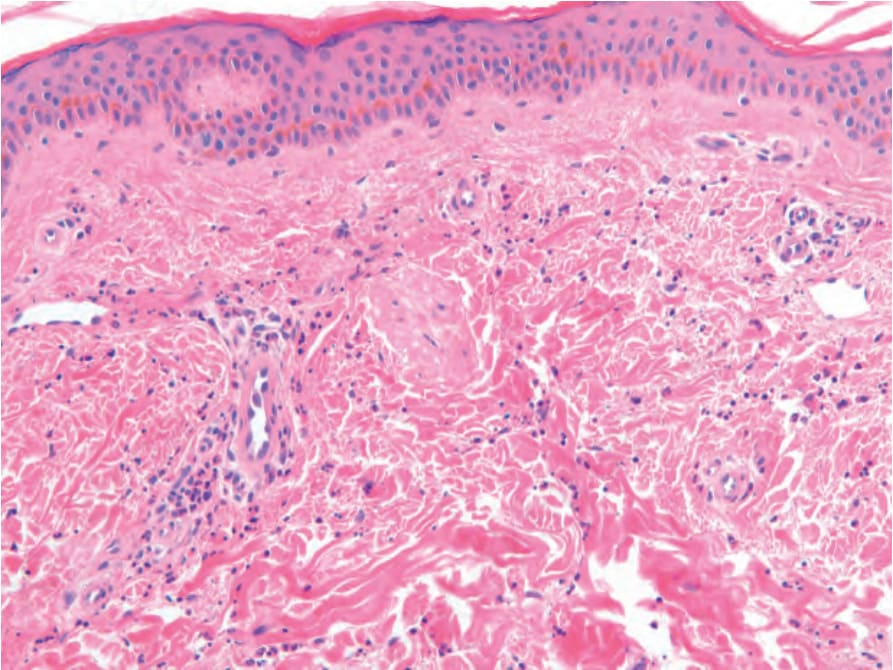
Fig. 15.47 Mild perivascular neutrophilic infiltrate in patient with Schnitzler syndrome. By courtesy of Dr. Anthony P. Fernandez, Cleveland Clinic, Cleveland, USA.
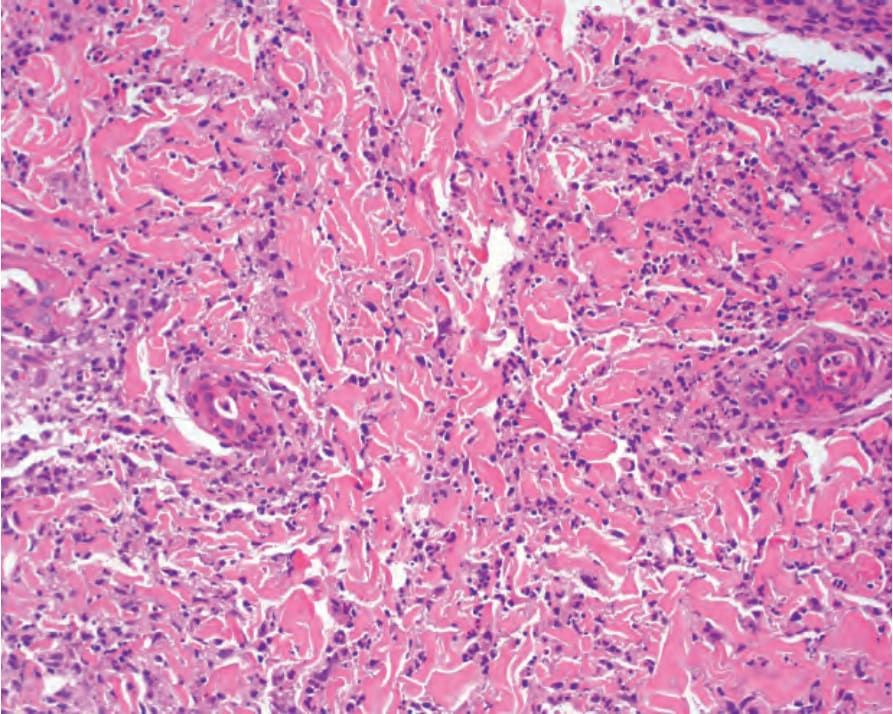
Fig. 15.48 Biopsy from patient with neutrophilic urticarial dermatitis with interstitial infiltrate with cordlike pattern intercalating between collagen bundles.