Urticaria
Urticaria
Clinical features Urticaria is an extremely common group of disorders that share common clinical and histologic features (Table 15.3).1 The lifetime incidence approaches one in five people.2 As will be seen later, urticaria has many
698 Neutrophilic and eosinophilic dermatoses
Types Subtypes Definition
Spontaneous urticaria Acute spontaneous urticaria Spontaneous wheals and/or angioedema < 6 weeks Chronic spontaneous urticaria Spontaneous wheals and/or angioedema > 6 weeks
Physical urticaria Cold contact urticaria Eliciting factor: cold objects/air/fluids/wind Delayed pressure urticaria Eliciting factor: vertical pressure (wheals arising with a 3–12 h latency) Heat contact urticaria Eliciting factor: localized heat Solar urticaria Eliciting factor: UV and/or visible light Urticaria factitia/dermographic urticaria Eliciting factor: mechanical shearing forces (wheals arising after 1–5 min) Vibratory urticaria/angioedema Eliciting factor: vibratory forces, e.g., pneumatic hammer
Other urticaria types Aquagenic urticaria Eliciting factor: water Cholinergic urticaria Elicitation by increase of body core temperature due to physical exercises, spicy food Contact urticaria Elicitation by contact with urticariogenic substance Exercise induced anaphylaxis/urticaria Eliciting factor: physical exercise
Table 2 from Zuberbier T, Asero R, Bindslev-Jensen C, et al. EAACI/GA2LEN/EDF/WAO guideline: definition, classification and diagnosis of urticaria. Allergy 2009; 64:1417–1426.
different etiologies but, more often than not, the cause remains unknown and the disease is then classified as idiopathic. In some patients, more than one stimulus may elicit symptoms.3 The clinical common denominator in urticaria is the development of ‘hives’ or ‘wheals’ – raised edematous lesions – which are often surrounded by a zone of erythema and are commonly pruritic (Figs 15.37–15.40).4,5 Dermatographism – pressure or light scratching resulting in linear urticarial lesions – is a common symptom. Urticaria may develop in only seconds. Lesions usually resolve in less than a few hours. By definition, lesions in patients with chronic urticaria, however, persist over a period in excess of 6 weeks.5,6 In addition, individual lesions in patients with chronic urticaria often last longer – up to 36 hours.4
sensitizing agent, such as a drug, may be necessary.10–12 In some patients, lesions even arise in areas covered by light clothing.13 ‘Fixed solar urticaria’ is a designation given to a rare form of urticaria seen in patients who develop lesions at the same sites with repeated light exposure.14,15 Solar urticaria has also been described following exposure to infrared and ultraviolet radiation.16,17
Given that urticaria is best viewed not as a single disease but as a group of related disorders, it comes as no surprise that the natural history of urticaria is highly variable.2 Resolution is seen in 50% of patients within a few years of onset; however, in some patients the disease persists for decades.2,5 The severity of symptoms is also variable. For many patients, the disease is a minor annoyance; for others, however, it can result in significant impacts in quality of life and severe reactions may be associated with life-threatening anaphylaxis.7
Physical causes of urticaria include sunlight, cold, heat, pressure, and vibration.
Solar urticaria Solar urticaria is characterized by development of wheals and pruritus that usually develop within minutes at sites exposed to light (Fig. 15.41).8,9 A
Aquagenic urticaria ‘Aquagenic urticaria’ is a bizarre variant of physical urticaria in which patients develop lesions following exposure to water (regardless of temperature).18,19 Extracutaneous manifestations such as migraine headache and familial occurrence has been described on rare occasion.20–22 Thankfully, patients do not develop symptoms from drinking water.5,23 Application of petrolatum ointment or other barrier cream prior to water exposure helps to prevent lesion development.18,24,25 It has been postulated that a water-soluble epidermal antigen may be responsible for such symptoms, since aqueous extracts of callus cause symptoms in patients’ skin but not in that of controls.26 Increased water salinity has also been implicated.27
699 Urticaria
• urticaria,
• fever,
• arthralgias,
• arthritis,
• conjunctivitis,
• leukocytosis. Patients with this syndrome develop symptoms with a decrease in body temperature but do not develop wheals at the site of an ice cube applied to skin. Patients have been shown to have gain of function mutations in the NLRP3 gene (also known as CIAS1) on chromosome 1q44 encoding the protein cryopryin. This protein is part of the cytosolic inflammasome protein complex and involved in its activation.38–46 Most patients have missense mutations resulting in increased production of IL-1.46 Interestingly, Muckle-Wells syndrome is associated with the same gene and consists of periodic fever, frequent sensorineural hearing loss, amyloidosis, and recurrent urticaria not linked to cold exposure.39,47 In addition, neonatal-onset multisystem inflammatory disease also maps to this gene.48 The spectrum of autoinflammatory disorders is now referred to as the cryopinopathies.49,50
Urticaria induced by heat has rarely been documented.51–53
Delayed pressure urticaria Patients with ‘delayed pressure urticaria’ develop lesions at sites of pressure, such as areas of tight clothing.5,54 This form of urticaria is seen in 40% of patients with chronic urticaria (see below).5,55,56
Cholinergic urticaria Cholinergic urticaria – one of the most common subtypes of urticaria – is thought to result from release of cholinergic substances by nerves.57–59 Evidence in support of this theory includes the observation that wheals may be elicited by the injection of cholinergic compounds, and injection of anticholinergic agents blocks wheal formation.57 Furthermore, wheals do not develop in skin innervated by nerves injected with local anesthetic, and application of scopolamine to skin prevents aquagenic urticaria.23,57 Common causes of cholinergic urticaria include increase in body temperature (e.g., following a hot bath or shower), emotional stress, exercise, or consumption of spicy food (Fig. 15.42).5,57,60 A significant proportion may be from autologous sweat hypersesnsitivity.61 Familial cases of cholinergic urticaria have been reported.62
Cold urticaria Placing an ice cube on the skin of patients may elicit a wheal – a condition designated ‘cold urticaria’.5,28 Some patients, however, develop symptoms only after generalized cooling of the body.5,29 Occasionally, drinking cold liquids, bathing in cold water, or exposure to cold air elicits symptoms.5,30 Prolonged exposure to cold can result in generalized symptoms, including headache, dyspnea, hypotension, anaphylaxis, and loss of consciousness.30,31 The condition can be associated with other types of physical urticaria. Very rarely, there is associated cryoglobulinemia and in some cases the condition follows a viral infection or drug ingestion.28,32,33
Familial cold urticaria (familial cold autoinflammatory syndrome) which follows exposure to cold is an autosomal dominant condition characterized by34–37:
Contact urticaria Contact urticaria may be divided into two main subtypes: allergic and irritant.5
• Allergic contact urticaria is a hypersensitivity reaction following exposure to an allergen such as chemicals, foods, latex, plants, fruits
700 Neutrophilic and eosinophilic dermatoses
and vegetables, and animal-derived antigens.63–66 Not surprisingly, this form of urticaria often occurs in patients with a history of atopy.63,67
• Irritant contact urticaria is a nonimmunologically mediated form of urticaria secondary to a wide variety of substances found in cosmetics, food, and medications.63
Urticarial angioedema Patients with urticaria often develop angioedema characterized by edematous swelling of the lips, eyelids, and tissues of the oropharynx.5,68,69 Two main subtypes of angioedema are recognized: hereditary and nonhereditary (acquired).
• Hereditary angioedema is rare, autosomal dominantly inherited, and due to C1-esterase inhibitor deficiency.70
• Acquired angioedema is caused by drug reactions, allergic reactions, reaction to physical agents, hypereosinophilia, and acquired (nonhereditary) C1-esterase deficiency.69
Drug-induced urticaria Drug-induced urticaria is fairly common. It is present in 0.16% of medical inpatients and in 9% of cases of chronic urticaria or angioedema seen in dermatology outpatient departments.119,120 The drugs most commonly implicated are sulfonamides, penicillins, and non-steroidal anti-inflammatory medications.119 Aspirin may induce acute urticaria, worsen chronic urticaria, or act as a cofactor to induce anaphylaxis.121 Other less common drug associations include antipsychotics, alendronate, recombinant IFN-β, cetirizine, bleomycin, and IL-3.121–127 Many of these reactions are mediated by IgE antibodies, but some result from direct activation of mast cells or interact with another pathway that augments the urticaria reaction.128 In this last category, modulation of arachidonic acid metabolites by aspirin and other agents can help initiate or exacerbate urticaria.129 A variety of genetic polymorphisms in different components of the inflammatory cascade have been linked to aspirin-induced urticaria, including the leukotriene C4 synthase, the prostaglandin E2 receptor subtype EP4, IL18 promoter, thromboxane A2 receptor, and adenosine A3 receptor.130–138
An idiopathic variant is also recognized.
Physical urticaria, secondary to vibration, cold, and sunlight, as well as contact (type I) hypersensitivity reaction and cholinergic urticaria may be associated with angioedema.69
Urticarial vasculitis Urticarial vasculitis is an uncommon condition which combines clinical features of chronic urticaria and histologic findings of leukocytoclastic or lymphocytic venulitis.71–75 A type III hypersensitivity reaction (caused by antibody–antigen complexes) appears to be the underlying etiology in a subset of patients.75,76 In many patients, however, no underlying cause is discovered.
Other urticarial associations Urticaria has also been documented in association with autoimmune progesterone dermatitis, dermatophytosis, candidiasis, parasites (anisakiasis), consumption of tonic water, nicotine, alcohol consumption, and hepatitis B vaccination.139–145
Urticarial vasculitis is associated with a female predominance (2 : 1) and is most often seen in young to middle-aged adults. Urticarial lesions tend to last 24–72 hours and may be associated with pruritus, a burning sensation or pain.75,78–80 The frequency of attacks varies from daily to monthly. Hyperpigmentation can be present at resolution.

Fig. 15.38 Urticaria: erythematous, edematous, coalescing plaques on the trunk and proximal extremities of an infant. By courtesy of J.C. Pascual, MD, Alicante, Spain.

Fig. 15.39 Urticaria: in this patient, the erythematous border is well demonstrated. By courtesy of the Institute of Dermatology, London, UK.
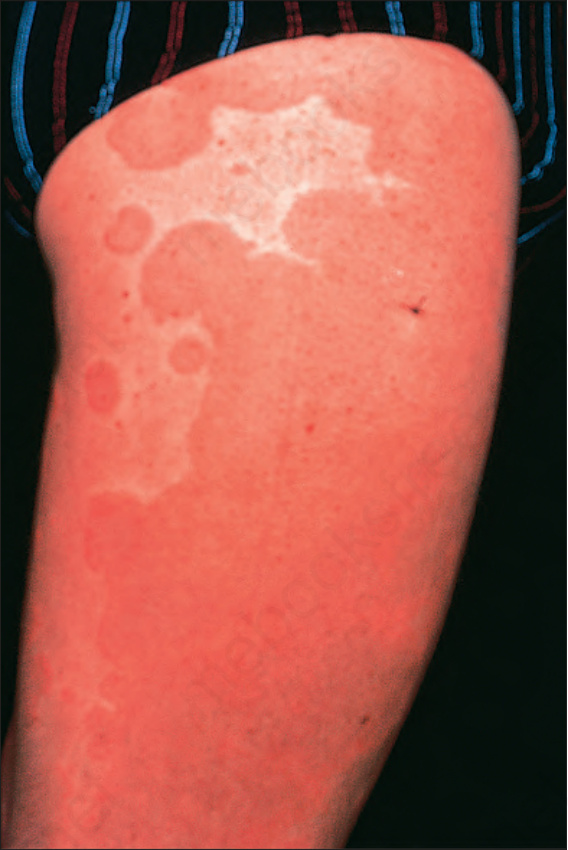
Fig. 15.40 Urticaria: in this extreme example, there is intense erythema. By courtesy of the Institute of Dermatology, London, UK.
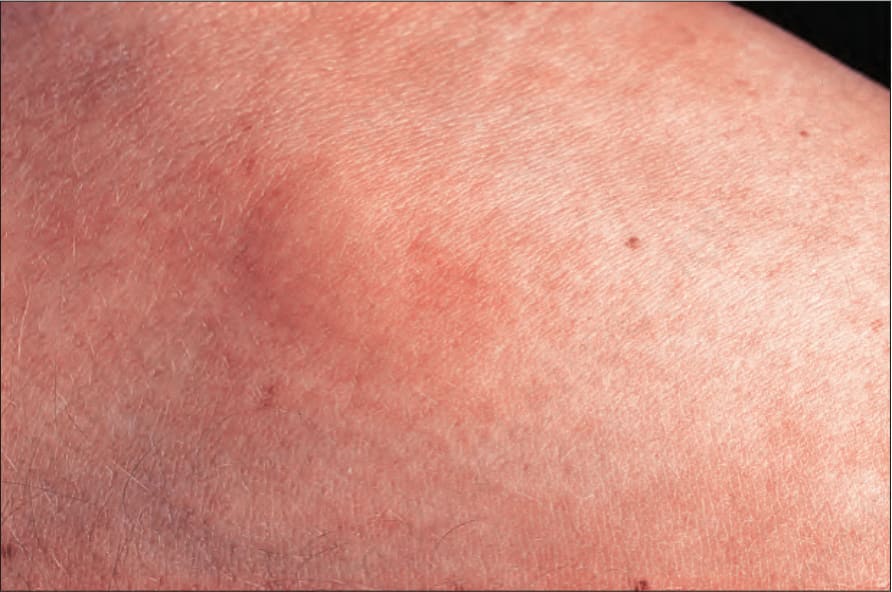
Fig. 15.41 Solar urticaria: in this patient, urticaria developed after exposure to sunlight. By courtesy of the Institute of Dermatology, London, UK.

Fig. 15.42 Cholinergic urticaria: in this variant, urticaria follows heat, emotional stress, or a spicy meal. By courtesy of the Institute of Dermatology, London, UK.
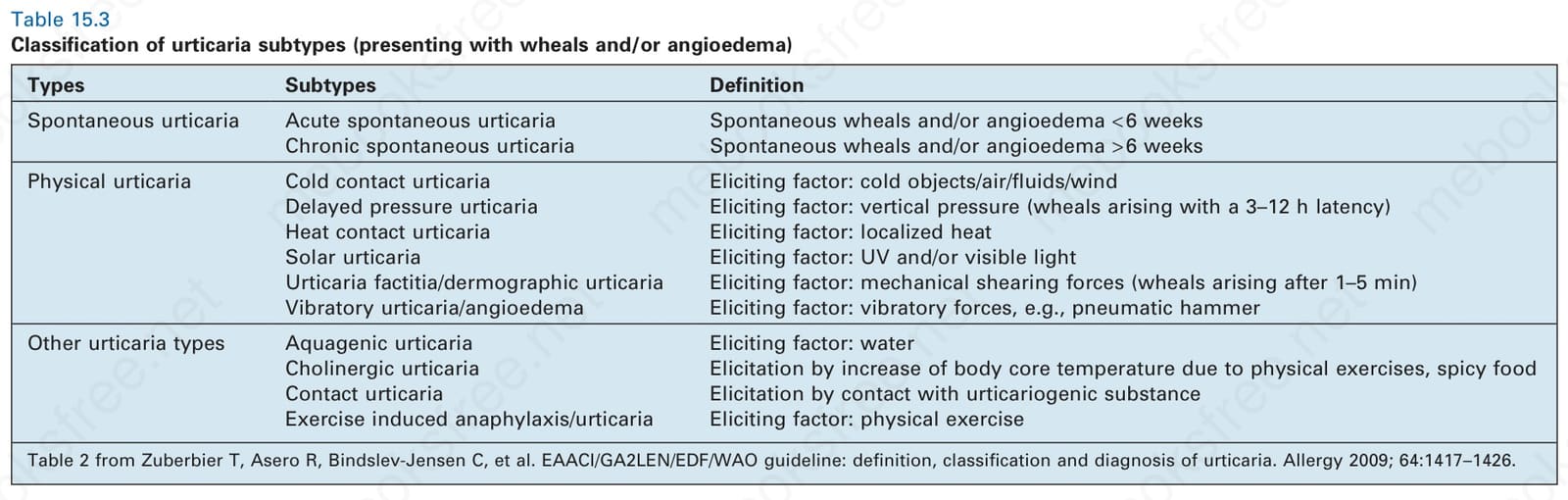
Table 15.3 Classification of urticaria subtypes (presenting with wheals and/or angioedema)
The spectrum of illness ranges from mild symptoms to a serious systemic illness.81 In addition to urticarial skin lesions, patients can also have angioedema, gastrointestinal symptoms, and evidence of renal involvement. Necrotic skin lesions are not usually seen. Other systemic manifestations/ associations include joint pain, stiffness, and swelling; however, frank arthritis is extremely rare. Some patients have proteinuria and hematuria. Rarely, renal biopsy reveals the features of focal or diffuse proliferative glomerulonephritis. Crescentic glomerulonephritis and mesangial and membranous nephropathy have been described in some patients.81–83 The ESR is frequently raised.
Pathogenesis and histologic features As has been stated above, urticaria is probably best viewed as a group of disorders sharing common clinical and histologic features. The pathogenesis of some forms of urticaria (e.g., allergic contact urticaria) is well understood; however, the precise pathogenesis of many cases of urticaria is obscure.146 Mast cell degranulation with perhaps some involvement of basophils appears to be a common denominator in the pathway of most types of urticaria.147,148
Release of histamine following a hypersensitivity reaction after exposure to an allergen is the basis for allergic contact urticaria.68 In sensitized patients, an allergen binds to IgE on mast cells causing degranulation and the release of histamine, eosinophil chemotactic factor, prostaglandin, leukotrienes, platelet activating factor, and enzymes.63,146,147,149,150 Similarly, IgE-mediated mast cell degranulation also underlies the pathogenesis of allergic contact urticaria in which direct contact with allergens on skin bind to the surface IgE on mast cells causing release of histamine and other inflammatory mediators. Autoantibodies against the IgE high-affinity receptor (FcεRI) or to IgE itself are present in about 30% of patients with chronic urticaria, designated autoimmune urticaria, a type II hypersensitivity reaction.146,151–155 Patients with physical urticaria or with connective tissue or autoimmune bullous disease may also have anti-FcεRI. However, in the last group of patients, the autoantibodies are nonfunctional (non-histamine releasing), whereas in chronic urticaria, the antibodies are functional (histamine releasing).154–156 A type III hypersensitivity reaction, caused by circulating antigen–antibody immune complexes, underlies a form of urticaria associated with serum sickness.
Rarely, urticarial vasculitis has been documented in association with malignancy, a relationship which may be coincidental.75,81,84–89
Hypocomplementemia is seen in many patients, and the presence of this sign correlates with systemic involvement and a high prevalence of autoantibodies to endothelial cells.76,81,90–92 Patients with Schnitzler syndrome have urticarial vasculitis and monoclonal IgM gammopathy.90–100 Hepatosplenomegaly, elevated ESR, raised white blood cell count, fever, and joint pain are frequent features.94–96 Occasional patients have an associated lymphoproliferative disorder.79 This disease is associated with anti-C1q autoantibodies in over half of the patients and likely mediate the disease in this subgroup.101,102
Urticarial vasculitis (especially the hypocomplementemic variant) is often associated with or precedes development of a variety of systemic diseases, including myeloma, hepatitis B and C, SLE, arthritis, interstitial lung disease, pericarditis, mixed connective tissue disease, inflammatory bowel disease, serum sickness, polyarteritis nodosa, granulomatosis with polyangiitis, viral infections, Sjögren syndrome, cryoglobulinemia, polycythemia rubra vera, reaction to drugs, and as a response to sunlight.75,81,89,90,101–113 Urticarial vasculitis has also been documented in association with pregnancy, exercise, and cocaine use.114–116 Ocular disease (including uveitis, scleritis, conjunctivitis, or episcleritis) is a very common feature.81,117 Patients with hypocomplementemia appear to be at risk of developing more severe disease.103 Obviously, a diagnosis of urticarial vasculitis in any patient should initiate an evaluation for underlying disease.118
There is growing evidence that infection with Helicobacter pylori may play a causative role in chronic urticaria in a subset of patients, including cases where the urticaria resolved after treatment and returned on reinfection. 157–165
The pathogenesis of irritant contact urticaria is not well understood, but evidence suggests that degranulation of mast cells due to direct, nonimmunologically mediated contact causes release of vasogenic mediators.63,147 Similarly, it is thought that the physical urticarias (heat, cold, pressure, vibration, water) also result from a direct effect on mast cells in susceptible individuals.150
Some investigators have suggested that solar urticaria results from a type I hypersensitivity reaction to a photo-induced antigen eliciting IgE-mediated mast cell degranulation.13 An intriguing study has shown that most patients (77%) develop an urticarial reaction when challenged with autologous serum that has been irradiated using the same spectrum of light that induces lesions in each particular patient.166 Furthermore, patients with ‘fixed’
701 Urticaria
A
B
urticaria develop lesions at the same specific sites that are affected by light exposure following injection with irradiated plasma.18 Consistent with these observations, some patients with severe solar urticaria may be effectively treated by plasma exchange.167,168
A type III hypersensitivity reaction (caused by antibody–antigen complexes) appears to be the underlying etiology in some patients with urticarial vasculitis; however, no underlying cause is discovered in many patients.77,81 More recently, urticarial vasculitis has been excluded from the formal urticaria group of disorders by some authors due to its variant pathogenic mechanism, but is still considered in this section for historical purposes.2
The biopsy findings in urticaria are non-specific. Dermal edema may be mild or severe, and its presence is confirmed by separation of dermal reticular collagen fibers. An often sparse dermal perivascular and interstitial mixed inflammatory infiltrate composed of variable numbers of lymphocytes, neutrophils, and eosinophils is present (Fig. 15.43). An increased number of intravascular neutrophils are a frequent finding, although this is not invariable (Fig. 15.44). Of interest, mast cells – which play such an important role in the pathogenesis of urticaria – do not appear to be increased in number except in chronic urticaria.153,169 Usually, more inflammatory cells are seen in lesions of chronic urticaria compared to those of acute urticaria.169
Urticarial vasculitis combines histologic features of urticaria with superimposed vascular damage. The vasculitis affects the superficial vascular plexus and shows features of a leukocytoclastic subtype; however, compared with typical leukocytoclastic vasculitis, the histologic findings tend to be
subtle and are easily overlooked (Fig. 15.45). Mild or focal fibrinoid change apparent on only a few sections associated with few neutrophils and sparse karyorrhexis is typical. Some authors have shown that endothelial necrosis is unusual.77 Occasionally, impressive necrotizing vasculitis (features of typical leukocytoclastic vasculitis) may be seen. In some cases, the infiltrate is predominantly lymphocytic and the lesion has the appearance of a lymphocytic vasculitis.75 In summary, urticarial vasculitis appears as a continuum, ranging from urticaria with very mild vascular injury (most cases) to frank necrotizing vasculitis.170
Differential diagnosis The diagnosis requires careful clinical correlation. The biopsy findings are often very subtle: the dermal edema and sparse inflammatory infiltrate may be easily overlooked. A definitive diagnosis sometimes requires testing for response to particular antigens. Other forms of hypersensitivity reaction
702 Neutrophilic and eosinophilic dermatoses
such as arthropod bite and drug eruption can show similar features and require clinical correlation to distinguish them from urticaria. Clinical correlation is necessary to distinguish urticarial vasculitis from other forms of leukocytoclastic vasculitis. Although urticarial vasculitis is often associated with subtle low-grade vascular injury, this pattern should not be relied on in the distinction from other forms of vasculitis. In short, the pathologist’s role in diagnosis is to confirm the presence of vasculitis.
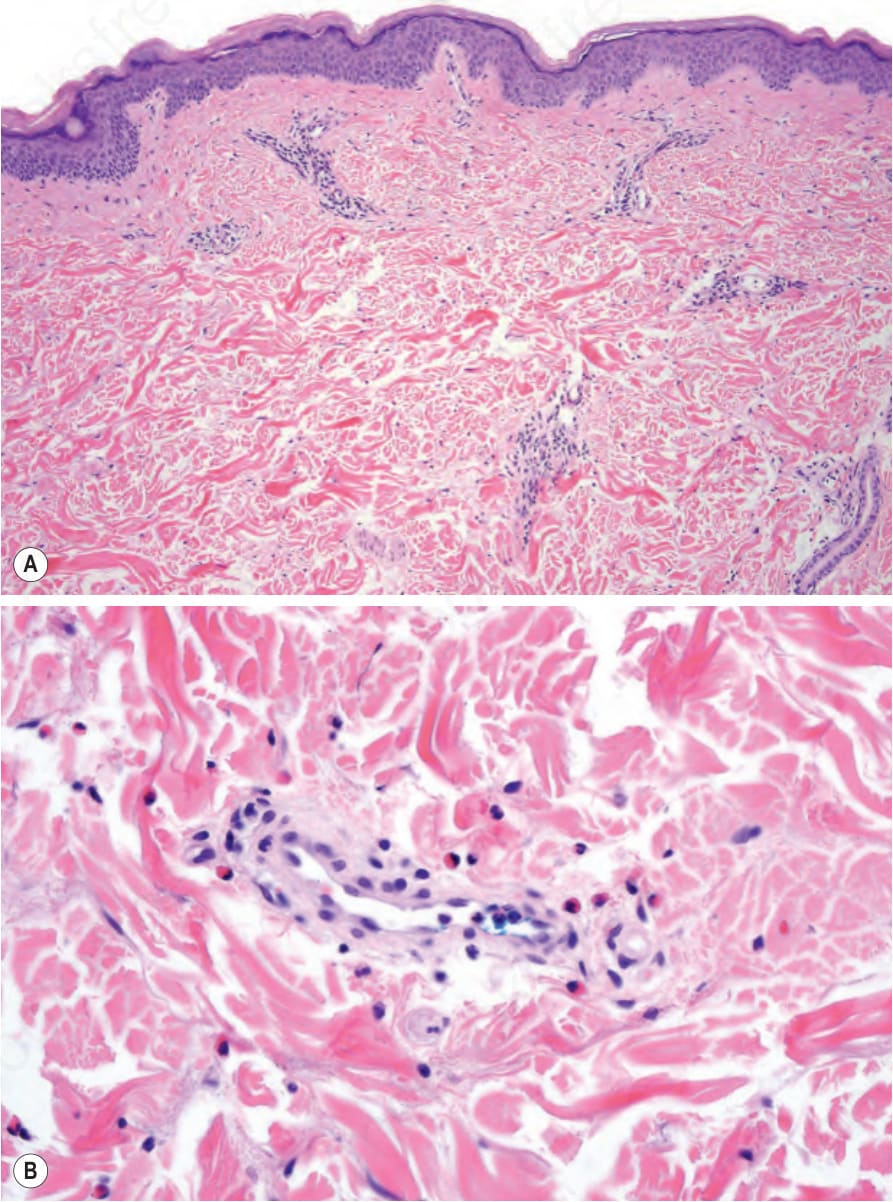
Fig. 15.43 Urticaria: (A) at low-power examination, the features are easily overlooked. There is a light perivascular infiltrate and the collagen fibers appear separated; (B) at high power, there is edema and a light perivascular infiltrate of lymphocytes with scattered eosinophils.
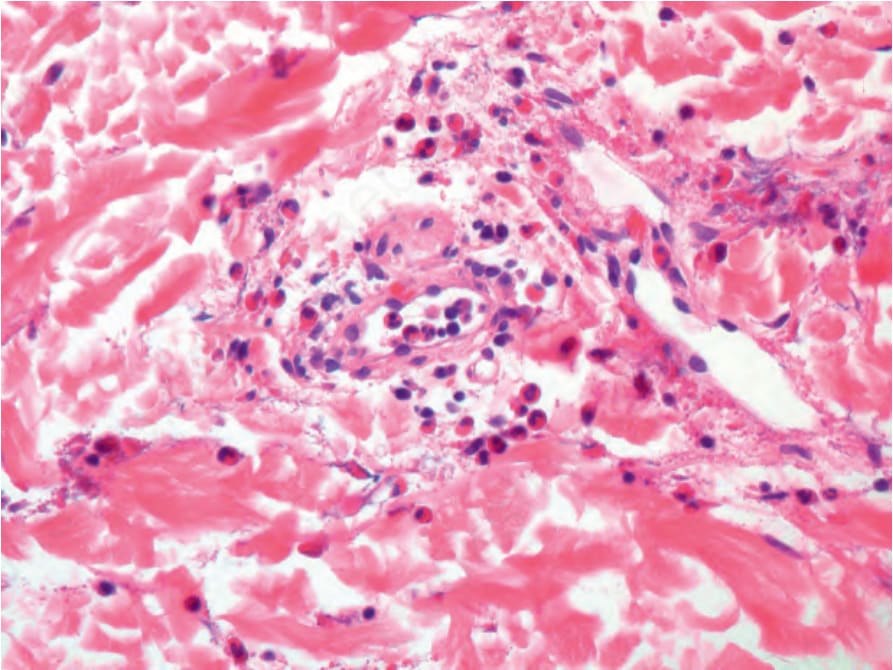
Fig. 15.44 Urticaria: in some cases intravascular neutrophils are prominent, and their presence can be a clue to the diagnosis.
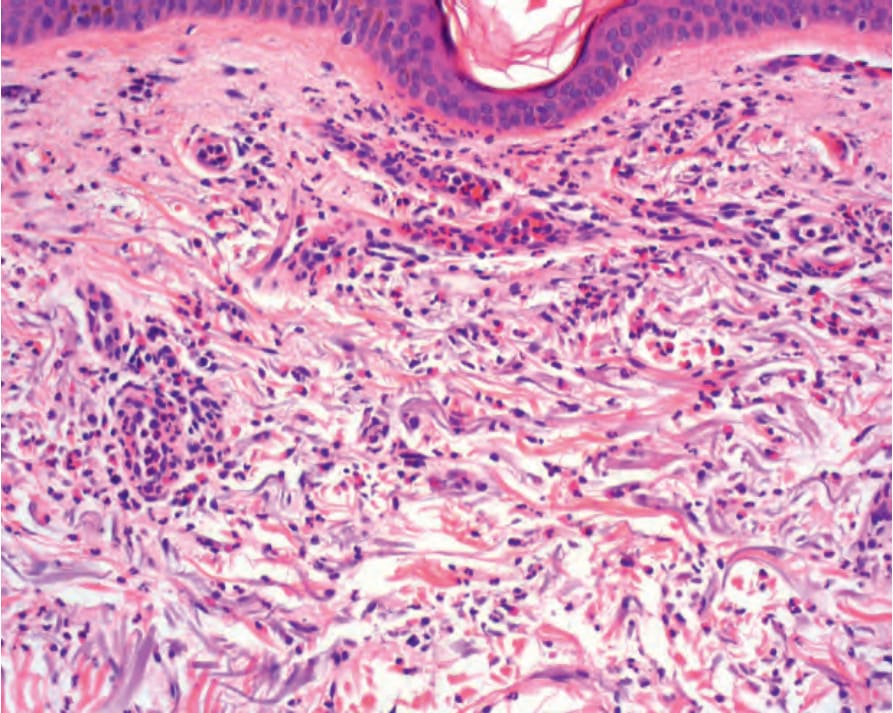
Fig. 15.45 Urticarial vasculitis: in this case there is a perivascular infiltrate of neutrophils and eosinophils with leukocytoclasia, subtle extravasation of erythrocytes but no fibrinoid necrosis of blood vessels.