Pyoderma gangrenosum
Pyoderma gangrenosum
Clinical features Pyoderma gangrenosum is an uncommon disease of obscure etiology.1–12 It appears to be somewhat more common in women and, although it may occur at any age, most patients are in their fourth or fifth decade.4 Presentation in children is uncommon, but it has been seen even in infants,13–25 and rare familial cases have been documented.26–29 The disease may also present in pregnancy, and in this setting it is associated with an underlying disease process in about 30–50% of the cases.30–34 Large, necrotic ulcers, often 10 cm or more in diameter, characterize the disease (Fig. 15.1). Lesions may arise from acneiform pustules or on a background of erythematous nodules. Typically, the ulcers have undermined edges and red–purple borders (Fig. 15.2). They may be solitary or multiple, and occur most often on the lower limbs, although other sites such as the trunk, face, arms, hands, and buttocks are sometimes affected (Fig. 15.3).4,5,35–37 Rare sites of involvement include the oropharyngeal region, hand, eyelid, eye, vulva, penis, scrotum, and the cervix.38–55 The ulcers are painful and tender, and may persist for months or years. Complications usually result from the site of the lesion and can include cranial osteolysis, nasal perforation, and tendon rupture.18,56,57 Recurrent attacks are not uncommon.2 Cribriform scarring often follows healing. Systemic involvement has rarely been documented, affecting the lungs, liver, bone, joints, pancreas, heart, and spleen.58–66
intravenous access site, arteriovenous dialysis shunt, blood-drawing, acupuncture, or a tattoo.4,120–125 Pressure from use of seat belts in automobiles has been associated with subsequent lesion development.126 Presentation has even been documented at the location of a spider bite.127 One case reports involvement of the scalp after receiving hair highlights at a salon, which could be due to physical and/or chemical trauma.128
A variety of drugs have been implicated as potential triggers, including, alpha-2b interferon (IFN-α2b), isotretinoin, sulpiride, propylthiouracil, lenalidomide, rituximab, sunitinib, imatinib, gefitinib, pazopanib, ipilimumab, and adalimumab.128–147 Paradoxically, some of these medications (e.g., rituximab, ipilimumab, and adalimumab) have been used to treat pyoderma gangrenosum.
Pyoderma gangrenosum after combination therapy with cytosine arabinoside, aclarubicin, and granulocyte colony-stimulating factor for myelodysplastic syndrome has been reported.148 Pyoderma gangrenosum has also been linked to levamisole-adulterated cocaine abuse.149–151. A granulomatous and suppurative dermatitis that may mimic pyoderma gangrenosum has been documented at the site of interferon-alpha (IFN-α) injections.152 Sclerotherapy has also been complicated by pyoderma gangrenosum on rare occasions.153 Of particular importance is the known association of pyoderma gangrenosum with a variety of conditions4,11,12,154 (in up to 50% of patients2) as outlined in Table 15.1. Of these, inflammatory bowel disease (both Crohn disease and ulcerative colitis) and arthritis show the most well-established links.155–158 Pyoderma gangrenosum is reported to complicate around 1–2% of inflammatory bowel disease patients.158–161 In one study, 27% of patients had associated inflammatory bowel disease and 20% of patients had arthritis.4 In this same study, 27% of patients with superficial ‘atypical’ pyoderma gangrenosum had an associated hematological disorder.4 In another large study, idiopathic pyoderma gangrenosum and that associated with chronic inflammatory bowel disease were found to be more common in females, whereas pyoderma gangrenosum associated with hematological malignancy was more common in males.5 While pyoderma gangrenosum can fluctuate with inflammatory bowel disease activity, it may also be a presenting or heralding feature. The presence of pyoderma gangrenosum as a complication of inflammatory bowel disease does not appear to be an independent predictor of severity of the bowel disease.162,163 Although pyoderma gangrenosum lesions may improve as inflammatory bowel disease is brought under control, specific treatment is usually required.163 Most of the other numerous, rare associations mentioned in Table 15.1 are likely to be fortuitous, as a report of simple coexistence does not strictly imply
Occasionally, bullous or pustular variants are encountered.4,67–83 One large study found that bullous lesions are more common on the upper extremities, and they appear to be more frequently associated with hematological malignancy.4 Such lesions are sometimes designated atypical pyoderma gangrenosum.4,68 A vegetative form has also been described.84–89 Some patients have more than one clinical type concurrently.80,82,86
A particularly interesting feature seen in 20–50% of cases is development of lesions in traumatized areas (pathergy).4,10,90,91 Lesions may occur at sites of surgery and have been reported after cholecystectomy, breast reduction or augmentation, splenectomy, hysterectomy, cesarean section, appendectomy, cardiac surgery, orthopedic surgery, herniorrhaphy, bowel bypass procedure, excision of anal condyloma, at the site of a fasciocutaneous flap, a laparoscopic port insertion site, and in an amputation stump (Fig. 15.4).92–119 In the postoperative setting, women appear to be disproportionately affected, with breast reconstruction surgery being the most common inciting incident.119 They also occur following rather trivial trauma such as injection or
683 Pyoderma gangrenosum
a meaningful association.164 In any event, a diagnosis of pyoderma gangrenosum should always prompt an evaluation for an underlying disease association. Pyoderma gangrenosum-like lesions have been reported as the presenting feature of antiphospholipid antibody syndrome.165 Other underlying conditions causing lesions that mimic pyoderma gangrenosum are also well described including inflammatory and infectious processes, vasculopathies, and malignancies, stressing the importance of careful clinical investigation.166–176
The disease may also occur in association with other neutrophilic dermatoses including Sweet syndrome and other dermatological diseases, such as lupus erythematosus and erythema nodosum, the latter typically in the background of concomitant inflammatory bowel disease.177–182 Pyoderma
gangrenosum is one of the components of an autosomal dominant syndrome known as PAPA (pyogenic sterile arthritis, pyoderma gangrenosum and acne).183 This syndrome has been mapped to chromosome 15q and is associated with mutations in the gene CD2BP1/PSTPIP1.184–194 These mutations increase the binding affinity of this gene product to pyrin, overcoming the autoinhibition of this homotrimer and allowing activation of the downstream innate immune response.189–191 Ultimately, this mutation leads to an increase in caspase-1 activation, an underlying feature of multiple inherited autoinflammatory syndromes.195 These findings indicate that pyoderma gangrenosum may be best regarded as an autoinflammatory or autoimmune disease, and the pathways being studied in PAPA syndrome may also eventually shed light onto the pathogenic mechanisms of sporadic
684 Neutrophilic and eosinophilic dermatoses
• Acne fulminans, acne conglobata and hidradenitis suppurativa265–269
• Acquired ichthyosis270
• Acute myeloid leukemia271
• Allergic contact dermatitis from rubber272
• Anaplastic large cell lymphoma273
• Antineutrophil cytoplasmic antibodies274–276
• Arthritis (either seronegative or rheumatoid arthritis), ankylosing spondylitis, and osteoarthrosis 4,277–279
• Autoimmune neutropenia of infancy280
• Behçet disease281
• Bullous systemic lupus erythematosus282
• Burns/scalding283,284
• C7 deficiency285
• Chronic idiopathic myelofibrosis286
• Chronic myelomonocytic leukemia287
• Chronic renal failure288
• Chlamydia pneumoniae289
• Cogan syndrome (interstitial keratitis and vestibuloauditory dysfunction) 290
• Collagenous colitis291,292
• Colorectal carcinoma293
• Cutaneous T-cell lymphoma294
• Cryofibrinogenemia295
• Cryoglobulinemia6
• Diverticular disease296
• Essential thrombocythemia 297
• Fanconi anemia298
• Factor V Leiden deficiency295
• Gastric carcinoma227,299
• Graves disease300
• Glomerulonephritis301
• Hepatitis, autoimmune and viral229,302–306
• Human immunodeficiency virus (HIV) infection307–309
• Hypertrophic osteoarthropathy310
• Hypogammaglobulinemia311,312
• Inflammatory bowel disease: both ulcerative colitis and Crohn disease2,4,159
• Juvenile idiopathic arthritis313
• Kartagener syndrome314
• Klinefelter syndrome315
• Lupus anticoagulant316
• Monoclonal gammopathy (most often IgA); usually benign but may lead to multiple myeloma2,69,279,317
• Multiple sclerosis318
• Myelodysplastic syndrome319,320
• Myelofibrosis321
• Myeloid leukemia70,72,228,322
• Osteomyelitis12,323
• Paroxysmal nocturnal hemoglobulinuria324
• Polycythemia rubra vera279
• Psoriasis325
• Renal transplant328,326
• SAPHO syndrome (synovitis, acne, pustulosis, hyperostosis, osteitis)327,328
• Sarcoidosis329
• Sjogren syndrome330
• Subcorneal pustular dermatosis331,332
• Systemic lupus erythematosus333
• Systemic sclerosis334
• Tuberculosis335
• Varicella (chickenpox)336
• Vasculitis, including Takayasu disease, erythema elevatum diutinum, and cutaneous granulomatosis337–343
described, and a patient with a mutation in NCSTN, a gene implicated in hidradenitis suppurativa, has been reported.200,201 Pyoderma gangrenosum has also been associated with LAD-1 (leukocyte adhesion deficiency-1) secondary to mutation of ITGB2.202–204
Para- and peristomal involvement in patients with ileostomy or colostomy for inflammatory bowel disease is a well-recognized phenomenon.4,205–211 In a large series, 13% of patients had peristomal pyoderma.4 Both Crohn disease and ulcerative colitis are associated with this complication.4,208–212 It should be noted that peristomal pyoderma gangrenosum has been seen in the absence of inflammatory bowel disease.205,206 It has been documented in patients with ostomy for gastrointestinal carcinoma and diverticular disease.205,206 Pyoderma gangrenosum may also occur at urostomy sites following cystectomy for bladder carcinoma.206,
Superficial granulomatous pyoderma is believed to represent a superficial and rare variant of pyoderma gangrenosum.3,212–218 However, the latter is controversial as patients with this condition usually do not have associated systemic disease and the histologic features are different with predominance of suppurative granulomas (see below). Patients develop single or sometimes multiple superficial ulcerated lesions with vegetative borders (for this reason, this variant is sometimes referred to as ‘vegetative variant of pyoderma gangrenosum’) as a consequence of trauma, frequently surgical (Fig. 15.5). Pain is an occasional feature. The ulcers have a cleaner base than those seen in classic pyoderma. Lesions are most commonly found on the trunk and upper extremities, and heal with cribriform scarring (Fig. 15.6). Draining sinuses are occasionally evident. Often there is no evidence of underlying systemic disease. Superficial granulomatous pyoderma is more likely to follow a chronic course compared with classic pyoderma gangrenosum.218 Rare cases involving the face, eye, and vulva have been reported.219–222

Fig. 15.1 Pyoderma gangrenosum: this unusually severe example is associated with very extensive tissue destruction resembling necrotizing fasciitis. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 15.2 Pyoderma gangrenosum: this shows an area of ulceration with a typical undermined purplish border. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 15.3 Pyoderma gangrenosum: an extensive lesion with marked crusting and undermining in the proximal and medial margins. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 15.4 Pyoderma gangrenosum: multiple early lesions at the site of previous surgery. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 15.5 Superficial granulomatous pyoderma: crusted superficial lesion with a cribriform appearance. By courtesy of the Institute of Dermatology, London, UK.

Fig. 15.6 Superficial granulomatous pyoderma: this field shows extensive ulceration of the breast. By courtesy of R.K. Winkelmann, MD, Mayo Clinic, Scottsdale, Arizona, USA.
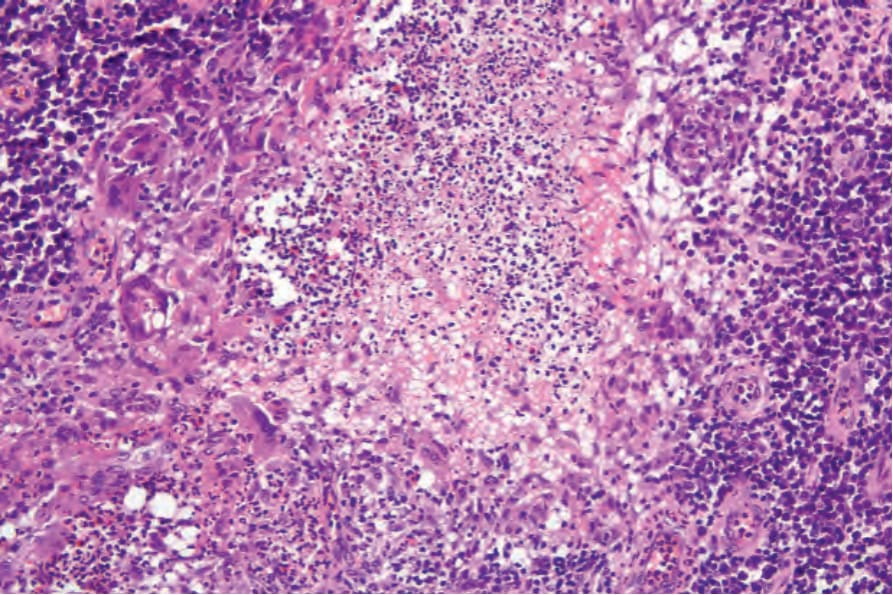
Fig. 15.11 Superficial granulomatous pyoderma: the zoned inflammatory reaction is clearly seen. Note the central abscess and surrounding granulomatous inflammation.
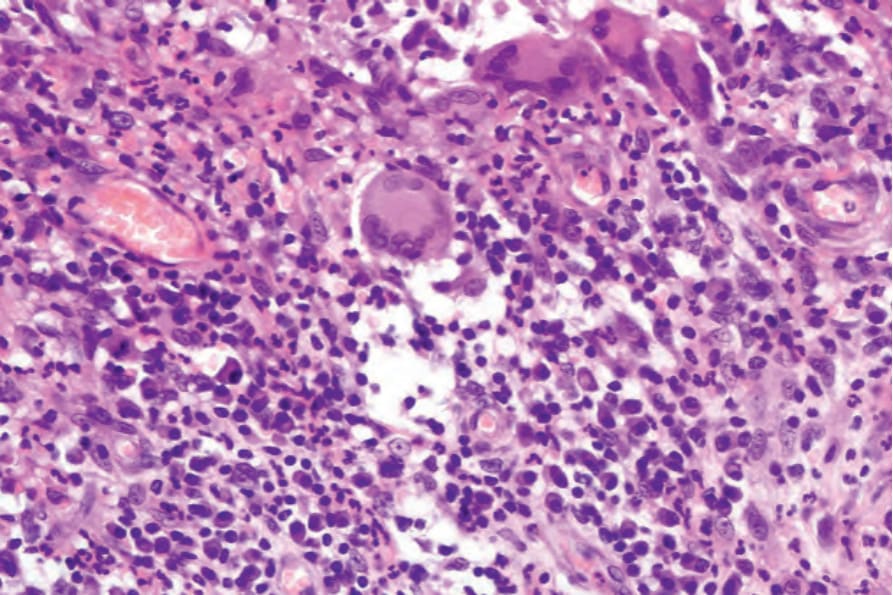
Fig. 15.12 Superficial granulomatous pyoderma: high-power view showing multinucleate giant cells. There are also conspicuous plasma cells.
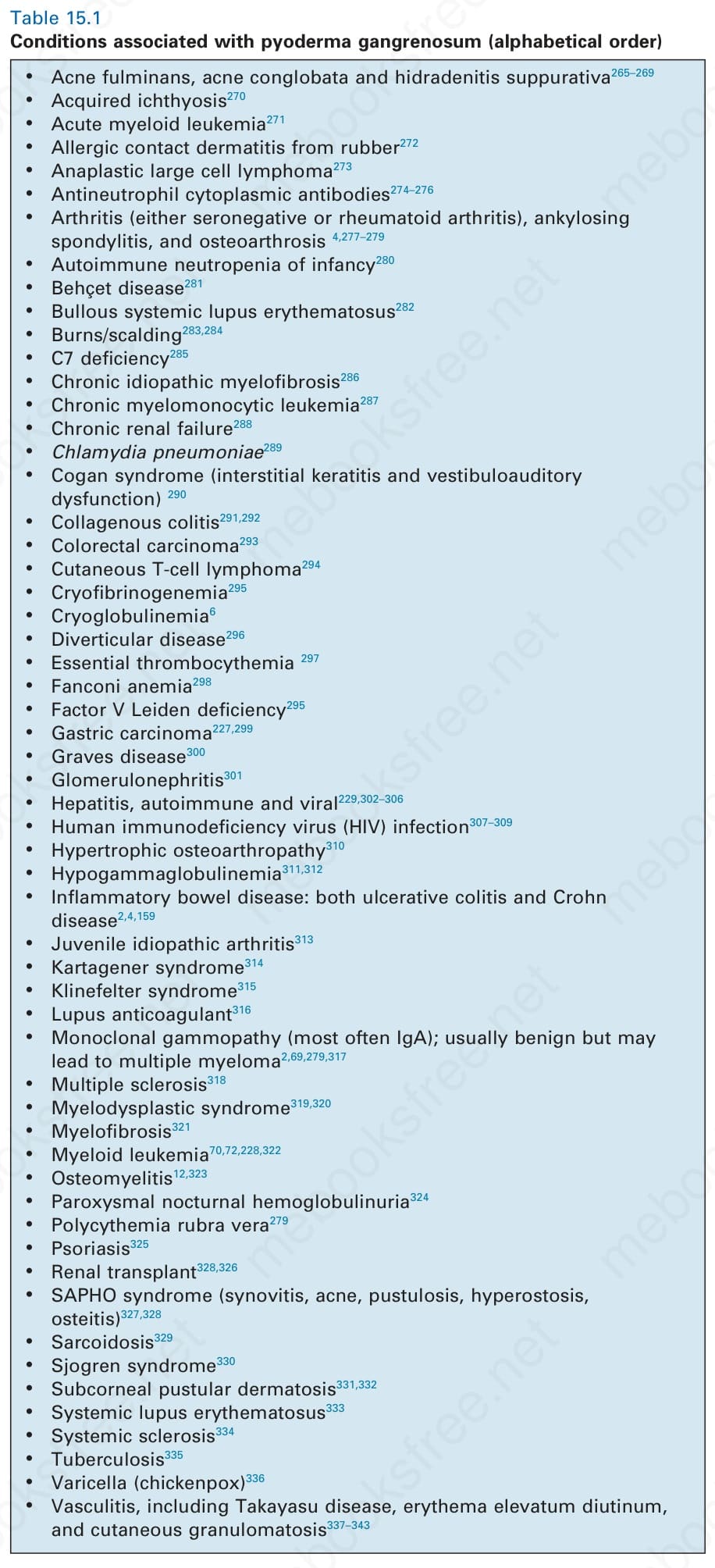
Table 15.1 Conditions associated with pyoderma gangrenosum (alphabetical order)
pyoderma gangrenosum.196 A related syndrome with hidradenitis instead of pyogenic arthritis (PASH) associated with mutations in PSTPIP1 has been described.197–199 Some patients have hidradenitis with arthritis (PAPASH).200 The genetics of pyoderma gangrenosum and these related syndromes is more complex than is appreciated. Cases lacking mutations in PSTPIP1 have been
So-called ‘malignant pyoderma’ is a controversial designation which we believe should be avoided. Some authors have used the term to describe a variant of pyoderma gangrenosum predominantly affecting the head and neck.223–226 It has been postulated that at least some cases of so-called malignant pyoderma more likely represent cutaneous granulomatosis with polyangiitis (cutaneous granulomatosis).226
One study found that over 50% of patients with pyoderma gangrenosum required long-term therapy to control their disease.5 The disease may be fatal in some cases, particularly if diagnosis is delayed.6,227 In another study, 2 of the 21 patients reported died of pyoderma gangrenosum secondary to pulmonary involvement.6
Pathogenesis and histologic features The precise pathogenesis of pyoderma gangrenosum is uncertain. The current state of knowledge suggests that it is due to immune dysfunction,
685 Pyoderma gangrenosum
A
perhaps innate, and/or that it develops on a vasculitic basis.10,12,186,228–233 A variety of immunological abnormalities have been described including:
• absent delayed hypersensitivity reactions to common antigens such as mycobacteria and Candida albicans
• defective neutrophil chemotaxis and irregular neutrophil trafficking
• impaired neutrophil phagocytosis
• diminished lymphokine (migration inhibition factor) production12,228,229,231
• overexpression of interleukin (IL)-8, a potent chemotactic polypeptide for neutrophils, has been reported in lesional tissue and may be an important pathogenetic factor234,235
• reduction in IL-8 and related molecules has been noted following successful therapy236
• overexpression of IL-17 and 23237–239
• aberrant neutrophil trafficking and metabolic integrin β2-CR3 and -CR4 oscillations in lesional tissue240,241
• elevated levels of HIF2a and downstream effectors vascular endothelial growth factor (VEGF) and Ang-2 have been noted in disseminated disease, suggesting that angiogenesis in improper control of the neutrophil oxidative burst may be involved242
• elevated tumor necrosis factor-alpha (TNF-α), MMP-9, and MMP-10 have also been noted237,243
• TNF-α may have some of its effects mediated by keratinocyte secretion of elafin, an elastase inhibitor.244 Indeed, anti-TNF-α therapy has been described to show some efficacy245–251; however, a case has also been described in association with TNF-α antagonists used to treat rheumatoid arthritis and the relationship may be complex.252
B
The results of immunofluorescence studies in large series of patients have revealed both immunoglobulins (usually IgM) and complement in blood vessel walls in the dermis of the leading edge of the ulcer.253,254 Another study, however, failed to substantiate this finding, and immunofluorescence should not be considered and ancillary diagnostic test.2 There is no evidence to support an infective pathogenesis.255
Expanding T-cell clones in both the skin and circulation have been described in a small series of patients, indicating that T-cell response plays a role in the disease and may be triggered by a local stimulus in the skin.256 T-cell clonality has been described in pyoderma gangrenosum in the absence of an underlying myeloproliferative disease.257
In general, the histopathology is that of non-specific ulceration with abscess formation (Fig. 15.7). The adjacent dermis shows acute and chronic inflammation. A pseudo-Pelger-Huet phenomenon with hyposegmented neutrophils making recognition difficult has been described in one patient.258 Early lesions may present with subcorneal pustulation (Fig. 15.8). Although the histologic features of both leukocytoclastic and lymphocyte-mediated
vasculitis have been described, it is our experience that any vasculitis present is usually located within the floor of the ulcer or in the immediate adjacent tissues and is, therefore, more likely to be a consequence, rather than a cause, of the lesion (Fig. 15.9).1,259 It has been suggested by some that some lesions of pyoderma gangrenosum may be initiated by acute folliculitis.260
686 Neutrophilic and eosinophilic dermatoses
Giant cells appear to be a common feature of pyoderma gangrenosum in patients with Crohn disease.7 In one study, they were present in 6 of 13 patients with associated inflammatory bowel disease; of these, 5 had Crohn disease and 1 had ulcerative colitis.7 Giant cells were not found in any biopsies from 22 patients without associated inflammatory bowel disease.
Differential diagnosis The histopathological findings in pyoderma gangrenosum are non-specific, and the diagnosis is primarily one of exclusion.261 Since surgery is used to manage some of the disorders considered in the histologic and clinical differential diagnosis – but is contraindicated in the treatment of pyoderma gangrenosum – early and accurate diagnosis is critical. Surgery, which tends to exacerbate the disease, is generally contraindicated in pyoderma cases because of the pathergic response. The mainstay of therapy is medical management, such as corticosteroids and more recently targeted therapies. Unfortunately, patients with pyoderma are often misdiagnosed early in the course of their disease, and the diagnosis is sometimes made only after multiple unsuccessful (and damaging) surgeries have been performed. In one study, an average of five physicians had examined the patient before a correct diagnosis was rendered.35 To avoid this error, obtaining accurate clinical information on wounds and debridement specimens is essential.
Superficial granulomatous pyoderma is characterized by a zoned inflammatory infiltrate in the superficial dermis.3 Focal and sterile abscesses are surrounded by a zone of granulomatous inflammation, mainly suppurative granulomas, bordered by a rim of lymphocytes and plasma cells (Figs 15.10–15.12).3 Hemorrhage is often present and eosinophils may be evident. Any vasculitic change is thought to be secondary. The adjacent tissues may show scarring. Acanthosis and pseudoepitheliomatous hyperplasia predominantly, but not exclusively of the infundibular portion of hair follicles are frequently noted. Foreign material including starch, sutures, vegetable matter, wood, and hair has been identified in a large proportion of these cases.3 It should be noted that not all cases of pyoderma gangrenosum with granulomatous inflammation are limited to the superficial dermis. Some cases show involvement of the deep dermis and even subcutaneous tissue.
Culture is required to exclude infection (bacterial, mycobacterial, fungal). Necrotizing fasciitis tends to affect deeper fascial and subcutaneous tissue, while pyoderma is centered in the dermis (albeit some spillover into the subcutis may be seen). Usually, sheets of bacteria are evident in untreated
necrotizing fasciitis. Distinguishing these two conditions is critical since the treatments are diametrical opposites with surgery and antibiotics for necrotizing fasciitis and avoidance of surgery with systemic anti-immune treatment and supportive wound care for pyoderma gangrenosum.262–264
Sweet syndrome is generally not associated with ulceration and shows more prominent karyorrhexis relative to the number of neutrophils, and the inflammatory cell infiltrate tends to be restricted to the dermis. Bite reactions, particularly resulting from the brown recluse or other spiders, may show similar histologic features, and eosinophils may not be a prominent feature in early lesions of bites. Clinical information is necessary to distinguish pyoderma from many other forms of ulcer such as those due to trauma.
687 Acute febrile neutrophilic dermatosis (Sweet syndrome)
scarring. Recurrences develop in approximately one-third of patients and postinflammatory hyperpigmentation is sometimes seen.47,48 Pathergy and koebnerization are occasional features, and necrosis with ulceration may rarely be encountered.7,49–51 Sweet syndrome may present with lesions mimicking palmoplantar pustulosis and sometimes erythema nodosum-like lesions are present.39,52,53 A Sweet syndrome-like eruption has been described in association with exposure to light.54
Sweet syndrome often follows an upper respiratory tract infection. In some cases, it is a complication of drug treatment, for example, carbamazepine, furosemide, hydralazine, co-trimoxazole, abacavir, azathioprine, ofloxacin, doxycycline, clindamycin, minocycline, trimethoprim–sulfamethoxazole, bortezomib, lenalidomide, imatinib mesylate, nilotinib, etanercept, granulocyte
Although some authors have noted lymphocytic or neutrophilic vasculitis in lesions of pyoderma gangrenosum, this finding, in our experience, is limited to areas adjacent to the ulcer and likely represents a secondary finding.5 Indeed, it has been our experience that ‘secondary’ vasculitis is frequently present at the border of ulcers of many different etiologies in patients without any genuine underlying ‘primary’ vasculitic process. Evaluation for vasculitis as a cause of ulceration, therefore, depends upon examination of blood vessels in areas of dermis and subcutaneous tissue away from the ulcer.
It cannot be overemphasized how important accurate clinical information is in establishing the correct diagnosis. Failing to recognize this disease early in its course can be disastrous for the patient.
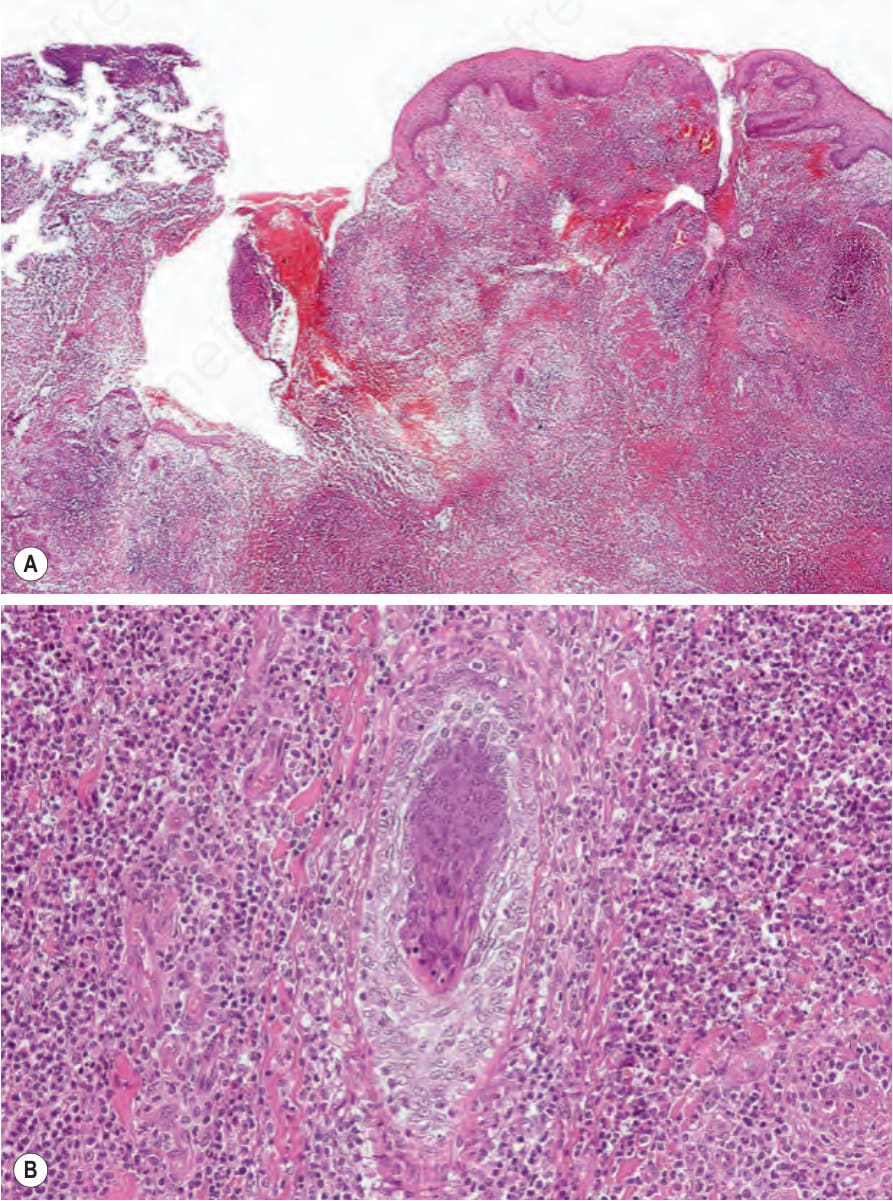
Fig. 15.7 (A, B) Pyoderma gangrenosum: in this biopsy from the edge of an ulcer, there are massive intradermal inflammatory changes, with abscess formation.
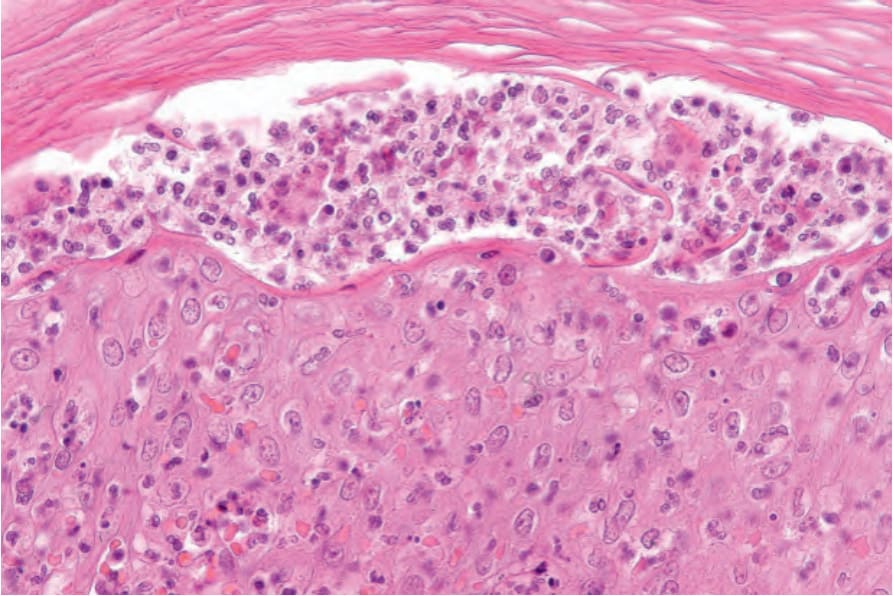
Fig. 15.8 Pyoderma gangrenosum: early acneiform lesion showing a subcorneal pustule.
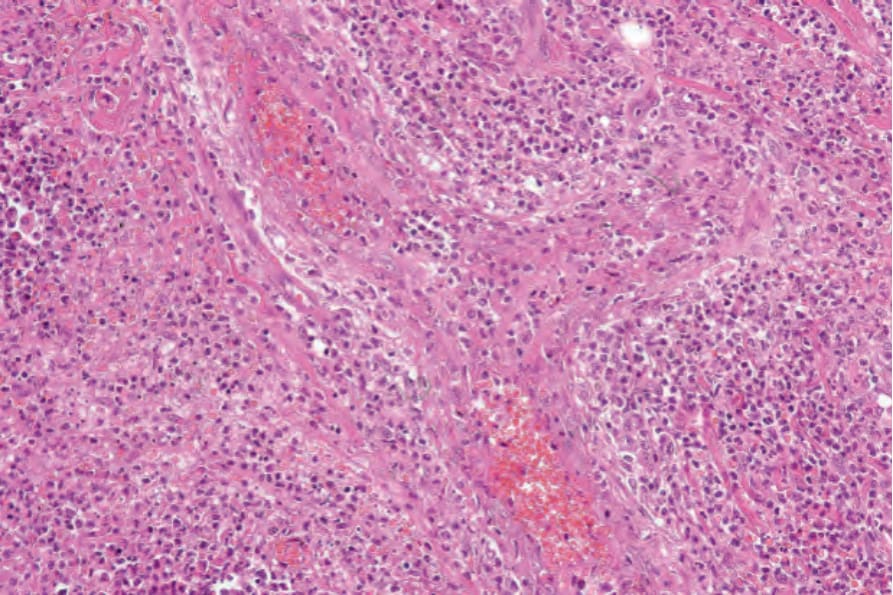
Fig. 15.9 Pyoderma gangrenosum: acute necrotizing vasculitis. It is likely that any active inflammation of the blood vessel walls is a result of the surrounding inflammation rather than its cause.
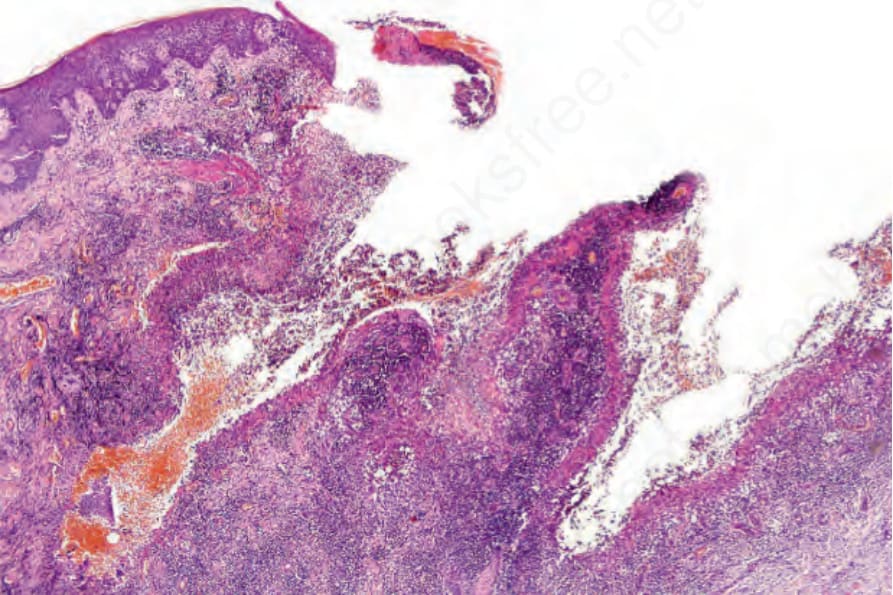
Fig. 15.10 Superficial granulomatous pyoderma: low-power view showing an undermining ulcer.