Aluminum granuloma
Aluminum granuloma
Clinical features Aluminum granuloma refers to the persistent, sometimes painful, subcutaneous nodules that develop at the sites of vaccination or hyposensitization with agents containing aluminum hydroxide as an absorbing agent (Fig. 14.127).1–5 If a vaccine is erroneously applied intradermally, lesions may occur within the dermis.6 The term granuloma is a misnomer as lesions do not usually consist of granulomatous inflammation. The lesions develop after a few weeks or years after the injections and are thought to be secondary to a hypersensitivity reaction to aluminum hydroxide. Often, patients have a contact allergy to aluminum as demonstrated by positive patch tests to aluminum hydroxide.7 The most common vaccine associated with this reaction is tetanus toxoid, but any vaccine containing aluminum hydroxide as an absorbent may induce the reaction, including hepatitis A and C and human papillomavirus vaccines.8
Intramuscular vaccines induce a condition described as macrophagic myofasciitis. This condition has been described both in children and adults.9,10
Pathogenesis and histologic features The occurrence of the nodules appears to be the result of a delayed hypersensitivity reaction to aluminum.
Four histologic patterns, which can overlap, may be found11:
• A predominantly lobular panniculitis with fairly non-specific findings including focal inflammation consisting of lymphocytes, histiocytes, and plasma cells with fat necrosis. Loose subcutaneous collections of histiocytes with a slightly granular, bluish cytoplasm are always found, but their number varies and the change may be subtle.
• A prominent subcutaneous, predominantly mononuclear, inflammatory cell infiltrate with eosinophils and focal formation of germinal centers often mimicking a marginal zone lymphoma (Figs 14.128–14.130). Plasma cells are often prominent. Careful examination reveals scattered grouped histiocytes with bluish granular cytoplasm.
• A deep granuloma annulare-like infiltrate with numerous histiocytes surrounding an area of necrobiosis (Figs 14.131 and 14.132). All the histiocytes show a characteristic bluish granular cytoplasm.
• A pattern with hyaline necrosis of the subcutaneous lobule mimicking lupus profundus. This is associated with lymphocytes, and plasma cells
680 Cutaneous adverse reactions to drugs
Histologic features Atrophic changes include loss and thinning of rete ridges with vascular ectasia.1,3 less commonly, foreign body-type granulomas and rheumatoid nodule/granuloma annulare-like granulomas may develop at injection sites.7–9 Small, elongated spaces are typical, and occasionally birefringment crystals are seen.9 The granulomatous reaction can surround amorphous mucinous material (Fig. 14.133).10,11 This material is not hyaluronic acid and should not be confused with primary dermal mucinosis.10 Titanium dioxide added to topical and injectable steroids like triamcinolone may exceptionally induce blue discoloration at the site of application. 12 Titanium dioxide can only be demonstrated by scanning electron microscopy with energy dispersive X-ray spectroscopy analysis.
and germinal centers may also be seen. Careful examination reveals the presence of typical histiocytes with bluish granular cytoplasm. A case with numerous mast cells and associated with urticaria has been described.12
Alpha-melanocyte stimulating hormone analogues (melanotan I and II)
Melanotan I and II are superpotent analogues of alpha-melanocyte stimulating hormone that have photoprotective effects. They appear to be increasingly used by patients who want to develop a prominent tan. Although they are not licensed for this purpose, they can be obtained through the Internet. Their administration not only induces prominent tanning but also induces enlargement and darkening of pre-existing nevi. Histology of these nevi has not been described in detail, but the few removed lesions in two patients did not show evidence of malignancy.1
The material within the histiocytes represents aluminum. Confirmation of the presence of aluminum can be done histochemically with the use of azurin stain or by energy dispersive X-ray microanalysis.

Fig. 14.127 Aluminum granuloma: multiple depressed nodules with scarring are evident. From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.
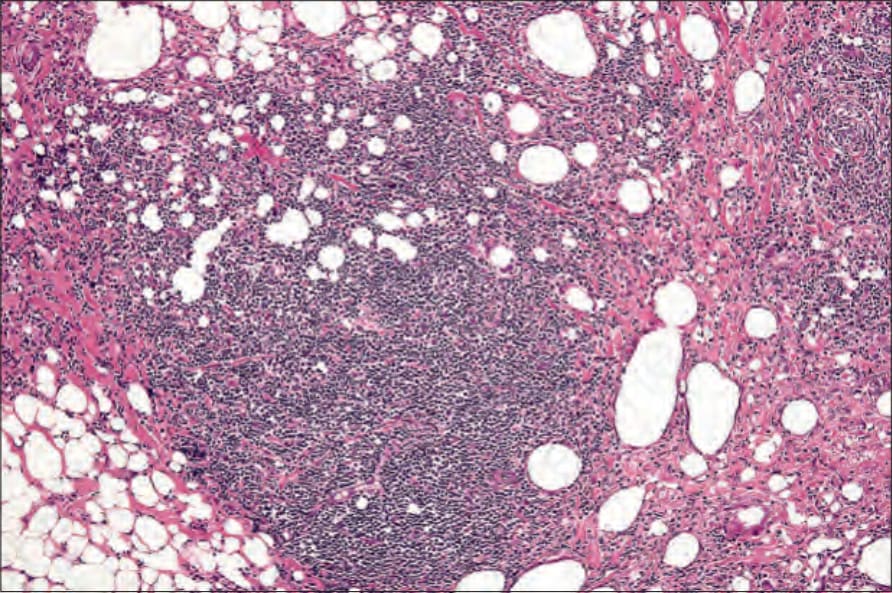
Fig. 14.128 Aluminum granuloma: there is a dense inflammatory cell infiltrate within the subcutaneous fat.
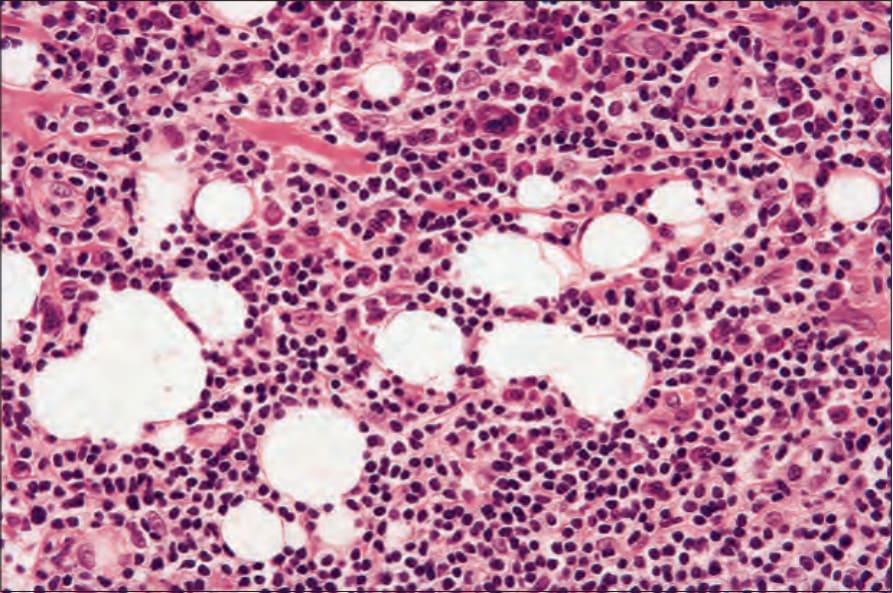
Fig. 14.129 Aluminum granuloma: the infiltrate consists of lymphocytes, histiocytes, and plasma cells.
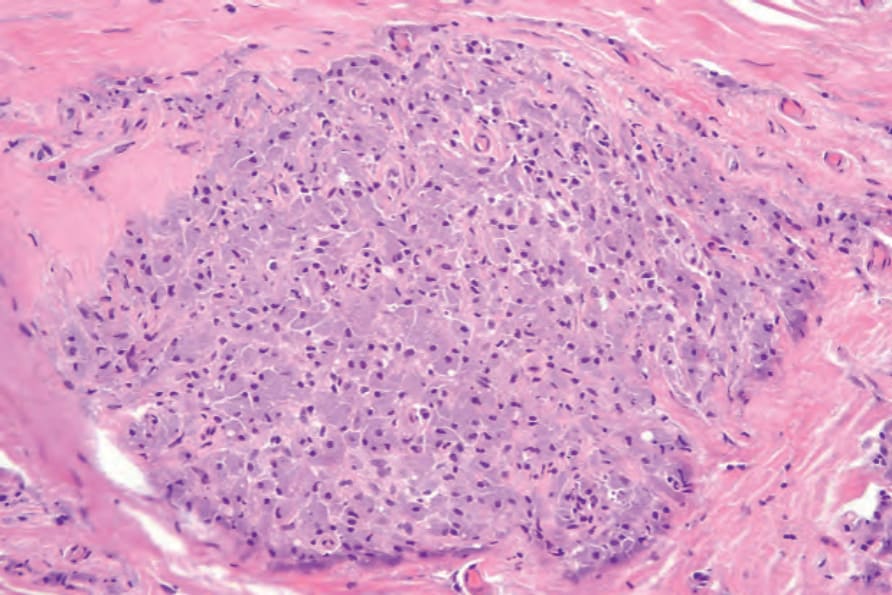
Fig. 14.130 Aluminum granuloma: the histiocytes have markedly granular cytoplasm due to the presence of aluminum.
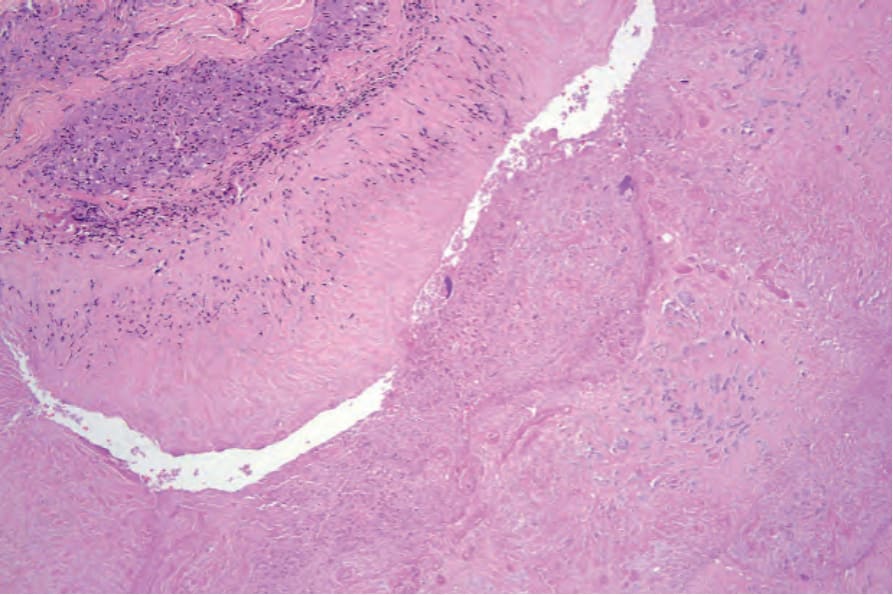
Fig. 14.131 Aluminum granuloma: in this example, there is a palisading granuloma surrounding a necrobiotic nodule.
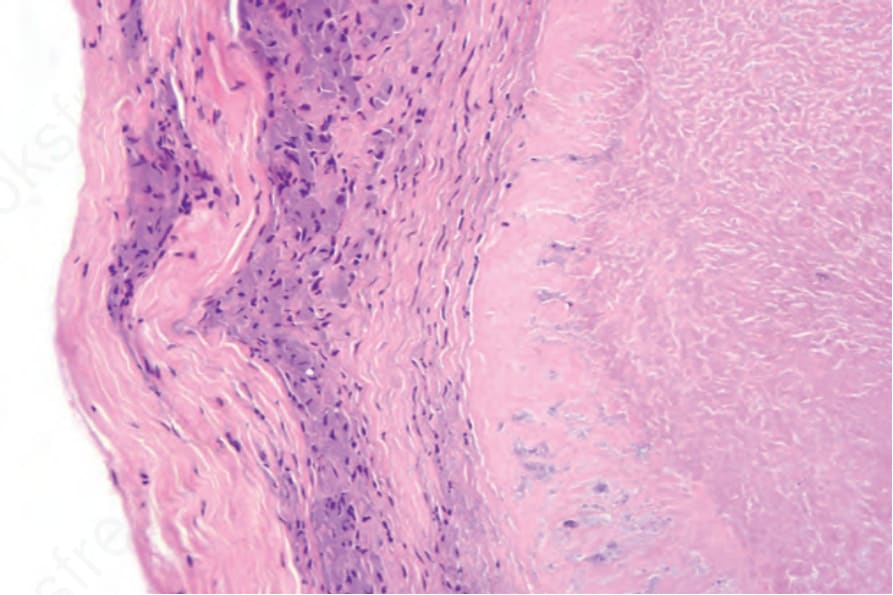
Fig. 14.132 Aluminum granuloma: the histiocytes have finely granular cytoplasm.
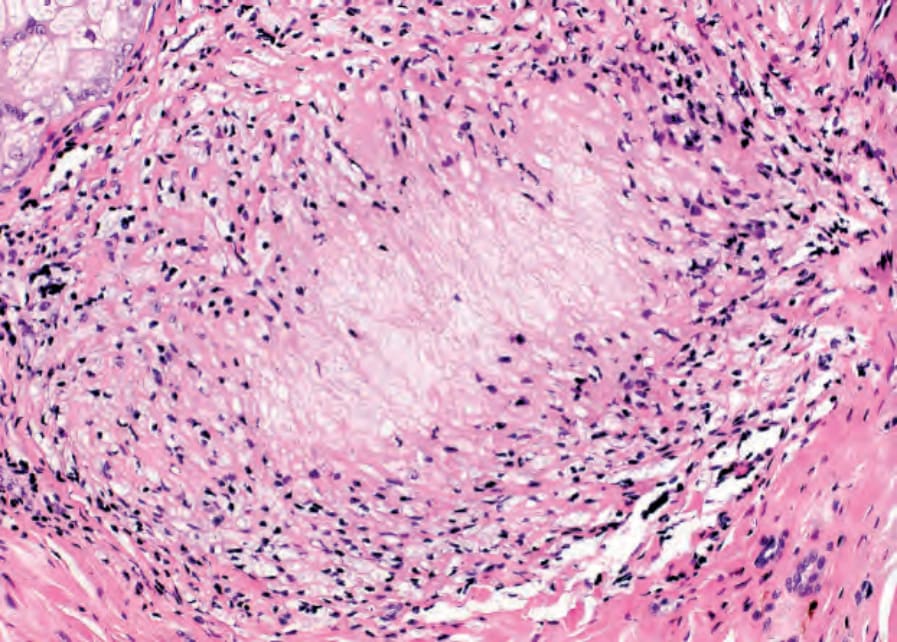
Fig. 14.133 Reaction to steroid injection: mucinous material surrounded by palisaded histiocytes and mimicking granuloma annulare. Courtesy of Dr Isabel Viana, Centro Hospitalar de Lisboa Ocidental, Lisboa, Portugal.