Chemotherapeutic agents
Chemotherapeutic agents
Clinical features The rapid rate of epidermal and mucosal turnover results in a high degree of susceptibility to the effects of chemotherapeutic agents. Among the most commonly encountered adverse responses are stomatitis, alopecia, and pigmentary changes.1–8
Stomatitis is very common and presents as burning erythema, followed by the development of extremely painful erosions and ulcers.2 Commonly implicated drugs include cyclophosphamide, methotrexate, bleomycin, cytarabine, doxorubicin, daunorubicin, dactinomycin, 5-fluorouracil, IL-2, hydroxyurea, and mercaptopurine.5,7 Secondary infection, such as with herpes simplex virus or Candida albicans, is an important complication.
following therapy with methotrexate – the so-called ‘flag sign’ – has also been documented.36
Hand-foot syndrome, also called chemotherapy-induced acral erythema acral erythrodysthesia or palmar-plantar erythrodysthesia, is commonly seen in patients receiving chemotherapy.37–41 The most commonly implicated agents include pegylated liposomal doxorubicin, capecitabine, docetaxel, and doxorubicin.41 Patients develop symmetric erythema, edema, and neuropathic pain involving the hands and feet that can progress to blistering with desquamation and ulceration.41 Hand-foot syndrome can also be accompanied by hyperpigmentation in patients treated with capecitabine. This is discussed in more detail below.
Proliferating hair follicles are highly susceptible to chemotherapeutic agents and as a consequence anagen effluvium (in which there is loss of much of the body hair) is a common and distressing complication.7,8 This is reversible once treatment is completed, although subsequent regrowth of hair may be accompanied by a change in color or texture.1 Concomitant premature catagen and telogen effluvium can result in total baldness.2 Drugs most often implicated include bleomycin, cyclophosphamide, daunorubicin, docetaxel, doxorubicin, etoposide, ifosfamide, mechlorethamine, methotrexate, mitoxantrone, and paclitaxel.1 Nail changes, including pale transverse ridges (Beau lines), develop as a result of mitosis inhibition with consequent temporary growth arrest and may be due to bleomycin, cyclophosphamide, and doxorubicin.5 Onycholysis can follow treatment with docetaxel, fluorouracil, and mitoxantrone.7 Transverse striate leukonychia (Mees lines), which result from periodic disruption of nail plate keratinization, classically have been described in association with arsenic poisoning.9 Similar lesions have been documented with a number of agents including ciclosporine and daunorubicin.10,11
Chemotherapeutic agents may interact with radiation therapy to result in various unusual manifestations including photosensitivity, radiation enhancement, radiation recall, and reactivation.
Photosensitivity may be induced by dacarbazine, 5-fluorouracil, hydroxyurea, and vinblastine.7
Radiation enhancement, which may be a feature of both dactinomycin and doxorubicin therapy, is due to impaired repair of radiation-induced sublethal cellular damage.2,5 As a consequence, the effects of radiation therapy are amplified. Clinical manifestations include increased erythema, hyperpigmentation, erosions, blistering, and necrosis at the site of radiation therapy.32 Radiation enhancement has also been encountered following therapy with adriamycin, bleomycin, cisplatin, 5-fluorouracil, hydroxyurea, and methotrexate.5,7
Maculopapular eruptions may be caused by several chemotherapeutic drugs including azathioprine, 5-fluorouracil, chlorambucil, melphalan, hydroxyurea, fludarabine, cladribine, gemcitabine, and pemetrexed.6,12 These are frequently a source of clinical diagnostic difficulty, as infectious diseases – including viral exanthemas and, in patients who have undergone transplantation, acute GVHD – are often within the differential diagnosis.
Radiation recall presents as erythema, vesiculation, and desquamation at the site of previous irradiation and may develop months or years after completion of treatment.2 The mechanism is unknown. Dactinomycin is particularly incriminated.2 A similar response has also been reported following therapy with adriamycin, bleomycin, cytarabine, doxorubicin, etoposide, 5-fluorouracil, hydroxyurea, melphalan, methotrexate, tamoxifen, and vinblastine.7,42,43 Radiation recall reactions have been described following treatment with paclitaxel, gemcitabine, docetaxel, IFN-α2b, dacarbazine, acyclovir, capecitabine, chlorambucil, and sorafenib.12,44–54
Reactivation of ultraviolet light-induced erythema has been described as a complication of methotrexate and suramin therapy.7,55 Manifestations include vesiculation and erythema.
Inflammatory changes affecting pre-existing actinic keratoses and seborrheic keratoses have been described following treatment with cisplatin, cytarabine, dacarbazine, dactinomycin, doxorubicin, 5-fluorouracil, 6-thioguanine, and vincristine.4,5 The affected keratoses become pruritic and erythematous. It is suggested that such changes are analogous to radiation recall phenomena.4
Cutaneous hyperpigmentation is a common complication of chemotherapeutic agents and often affects the hair, nails, and mucosae in addition to the skin.1–8,12–15 Hypopigmentation is less commonly seen.5 The mechanism for increased melanin synthesis by melanocytes is unknown. Alkylating agents including busulfan, cyclophosphamide, ifosfamide, hydroxyurea, 5-fluorouracil, methotrexate, and thiotepa are among the most often implicated agents.5,12,16,17 Nail changes (including diffuse pigmentation, longitudinal and transverse banding or streaks) are particularly seen with cyclophosphamide, daunorubicin, doxorubicin, 5-fluorouracil, and hydroxyurea.2,9 Cyclophosphamide also causes hyperpigmentation of the palms and fingers.12,15 Immediate or delayed tanning following sun exposure is a frequent complication of 5-fluorouracil. Rarely, patients may develop linear erythema, complicated by pigmentation around an injection site, so-called serpentine supravenous hyperpigmentation.7,17–20 Similar lesions have followed treatment with actinomycin and nitrosourea.21,22 Hair pigmentation can result from tamoxifen therapy.1,23 Bleomycin therapy is associated with cutaneous pigmentation affecting between 30% and 60% of patients.2,24 Pathognomonic linear flagellate streaks may develop on the skin of the trunk and proximal extremities.25–32 This flagellate pattern has also been reported in a patient receiving bendamustine.33 It is suggested that lesions develop as a consequence of trauma-induced vasodilatation with resultant local increased concentration of bleomycin. An early inflammatory phase, due to scratching, has occasionally been documented, suggesting that the pigmentation occurs as a consequence of postinflammatory changes. A similar problem of patterned hyperpigmentation has been documented following treatment with thiotepa (triethylene thiophosphoramide). Localized occlusion during treatment (e.g., with adhesive bandages) may cause retention of thio-TEPA-rich sweat and subsequent reversible hyperpigmentation confined to the occluded surfaces.12,34,35 Transverse banding of hair shafts
Hypersensitivity reactions (including urticaria, angioedema, serum sickness, anaphylaxis, generalized dermatitis, and fixed drug eruption) are uncommon complications of chemotherapy. Although a wide range of agents may result in these responses, L-asparaginase, intravenous melphalan, and cisplatin have been particularly incriminated.2,56,57 Cyclophosphamide, daunorubicin, doxorubicin, methotrexate, and procarbazine have also been implicated.57 Dacarbazine and procarbazine may cause fixed drug reactions.1 Immune complex-mediated reactions including vasculitis and some cases of EM or TEN may rarely be a result of treatment with hydroxyurea and mechlorethamine.5 Contact dermatitis is an uncommon but important complication of topical mechlorethamine (mustard) therapy.58
An interstitial granulomatous maculopapular eruption following low-dose methotrexate in the treatment of collagen vascular diseases including lupus erythematosus and rheumatoid arthritis has been described.59 The buttocks and limbs are commonly affected.
Newer chemotherapeutic agents have emerged that selectively target specific cellular pathways. Their increasing use has also resulted in diverse cutaneous side effects.60,61 One class of such drugs is the epidermal growth factor receptor (EGFR) inhibitors which are used to treat non-small cell lung cancer, breast, colon, pancreatic, and squamous cell carcinoma of the head and neck.62 Examples include cetuximab, gefitinib, erlotinib, and panitumab. Since EGFR is expressed in keratinocytes, follicular epithelium, eccrine glands, and sebaceous cells, adverse effects on the skin and appendages are common.63 Acute folliculitis on the face and trunk is most common (Fig. 14.94).60–62,64,65 Other potential side effects include dry skin (eczema
667 Chemotherapeutic agents
craquelé) (Fig. 14.95) with painful fissures (Fig. 14.96), pruritus, nail alterations (paronychia, ingrown nails, nail fold fissures, onycholysis, splinter hemorrhages, pyogenic granulomas) (Fig. 14.97), hair changes (frontal alopecia, trichomegaly of eyelashes (Fig. 14.98), altered hair texture), and mucositis (Fig. 14.99).60–69 Rare cases of vasculitis have also been reported (Fig. 14.100).70
Tyrosine kinase inhibitors imatinib, dasatinib, and nilotinib are used to treat chronic myeloid leukemia (CML).60 Imatinib is also approved for treatment of gastrointestinal stromal tumor (GIST) and rare cases of inoperable or metastatic dermatofibrosarcoma protuberans. A wide range of cutaneous effects have been reported with these medications, the more common being hyper-, hypo- and de-pigmentation and macular-papular exanthems.60,61,71,72 Patients may also develop edema and, less commonly, urticarial, lichenoid,
pityriasiform, and psoriasiform eruptions.61 SJS, AGEP, Sweet syndrome, neutrophilic eccrine hidradenitis, neutrophilic panniculitis, and lymphomatoid drug reactions have also been reported.61
Sorafenib and sunitinib are multikinase inhibitors currently approved for treatment of a variety of malignancies, including, renal cell carcinoma, hepatocellular carcinoma melanoma, non-small cell lung carcinoma, pancreatic carcinoma, colon cancer, breast cancer, melanoma, and GIST.60,61,73 The hand–foot skin reaction is seen in up to up to two-thirds of patients, typically 2 to 4 weeks after initiating treatment, and characterized by painful erythema and edema of the palms and soles (Fig. 14.101).60,61,63,74–76 There may be associated paresthesia and desquamation. The lesions are discrete
668 Cutaneous adverse reactions to drugs

Fig. 14.100 Vasculitic drug reaction in patient on EGFR inhibitor. By courtesy of Chao-Kai Hsu, MD, Sheau-Chiou Chao and Julia Yu-Yun, National Cheng Kung University Hospital, Tainan, Taiwan.
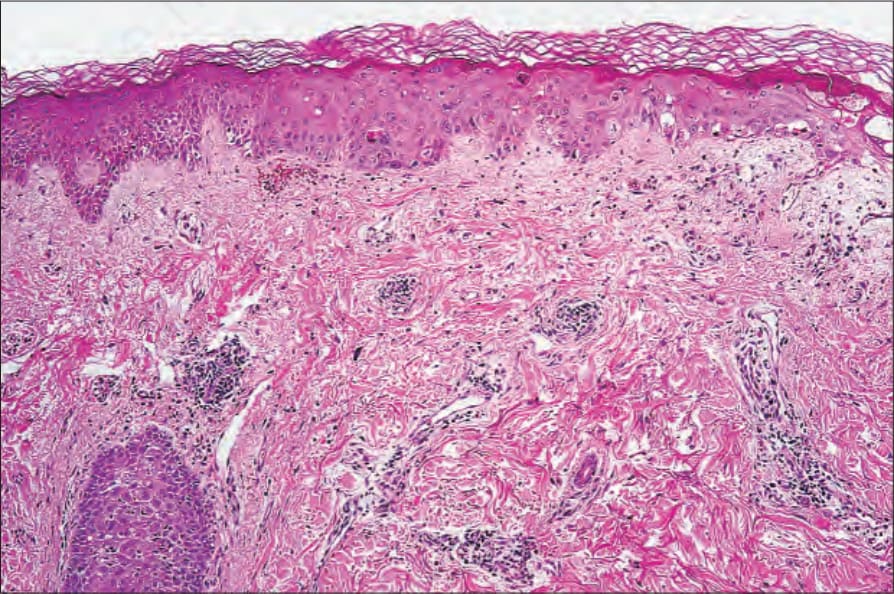
Fig. 14.104 Chemotherapy-related drug reaction: there are interface changes with basal cell hydropic degeneration and apoptosis.
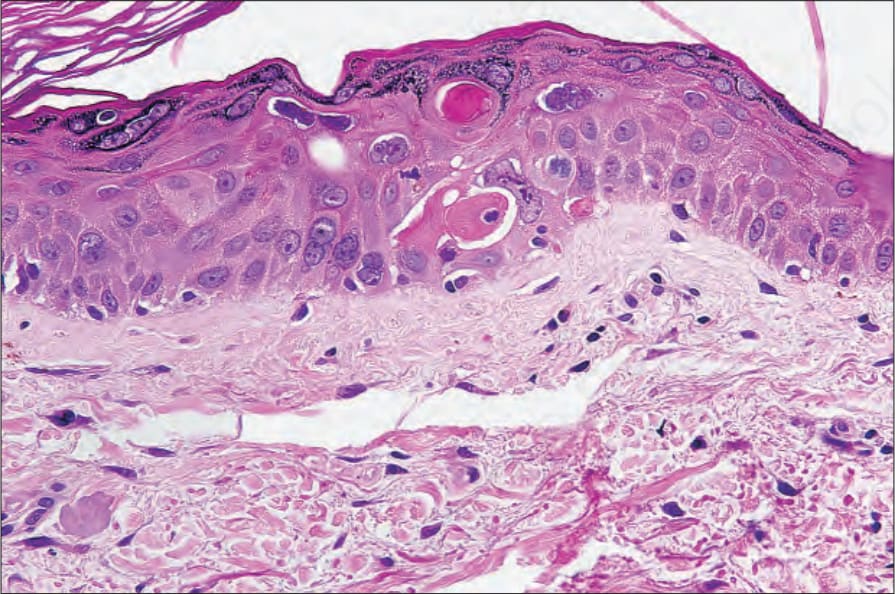
Fig. 14.105 Chemotherapy-related drug reaction: there is striking dyskeratosis and abnormal maturation. The latter is a common feature of chemotherapy reactions.
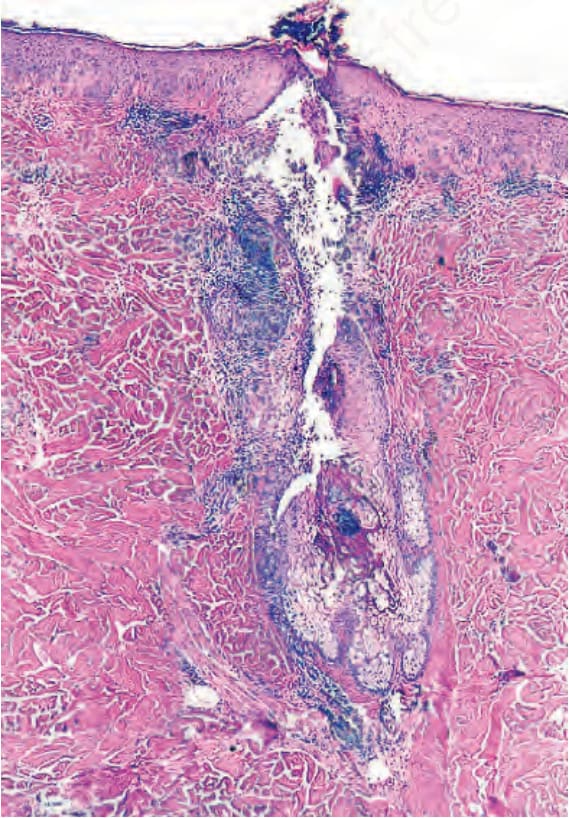
Fig. 14.108 Pustular folliculitis secondary to EGFR inhibitor. By courtesy of Klaus Busam, MD, Memorial Sloan Kettering Cancer Center, New York, New York, USA.

Fig. 14.109 Chemotherapy induced acral erythema characterized by circumscribed erythematous macules on soles. By courtesy of Eduardo Rozas Munoz, MD, Hospital de la Santa Creu I Sant Pau, Barcelona, Spain.

Fig. 14.94 Acneiform eruption in patient on EGFR inhibitor cetuximab. By courtesy of Klaus Busam, MD, Memorial Sloan Kettering Cancer Center, New York, New York, USA.

Fig. 14.95 Severe asteatotic eczema in patient on EGFR inhibitor panitumab.

Fig. 14.96 Painful palmar fissures in patient on EGFR inhibitor cetuximab.

Fig. 14.97 Severe paronychia in patient on EGFR inhibitor cetuximab. By courtesy of Klaus Busam, MD, Memorial Sloan Kettering Cancer Center, New York, New York, USA.

Fig. 14.98 Trichomegalia in patient on EGFR inhibitor panitumab.

Fig. 14.99 Mucositis in patient on EGFR inhibitor panitumab.
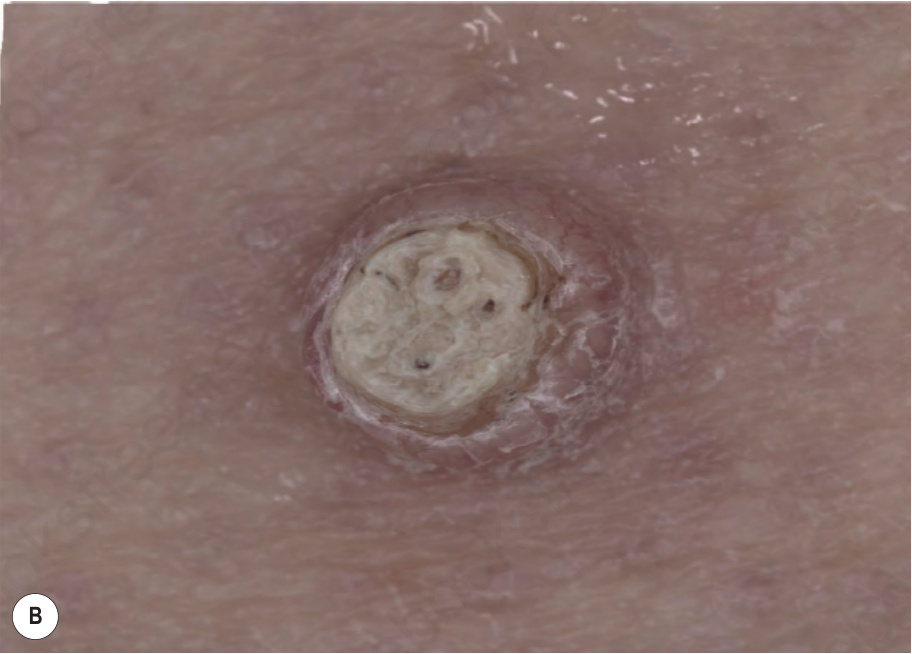
Fig. 14-101 (caption embedded in image / 圖說烘焙於圖內)
and accompanied by hyperkeratosis, a feature not usually seen in acral erythema associated with traditional chemotherapeutic agents.41,63 In contrast to hand-foot syndrome discussed above, hand–foot skin reaction also affects the soles more than the palms, although there is significant clinical overlap.41 Other cutaneous reactions linked to sorafenib include pruritus, alopecia, actinic keratoses, and squamous cell carcinoma.60,61,77,78
Vismodegib is an inhibitor of the smoothened receptor in the hedgehog pathway that is used for the treatment of metastatic and advanced basal cell carcinoma. The most common cutaneous side effect is alopecia, seen in over 60% of patients.61 Patients also may experience muscle spasms, dysgeusia, fatigue, nausea, and diarrhea.
Bortezomib, a proteasome inhibitor used to treat hematopoietic malignances, has been associated with morbilliform eruptions, ulcerations,
Fig. 14. 101 Chemotherapy-related drug reaction: there are discrete palmar bullae with a rim of erythema. The patient had been taking sorafenib. By courtesy of R. Lee, MD, Virginia Commonwealth University, Richmond, Virginia, USA.
CD30-positive lymphomatoid drug reaction, edematous plaques, vasculitis, and interface dermatitis.61,79–82
Vemurafenib and dabrafenib are BRAF inhibitors of the mitogen- activated protein kinase (MAPK) pathway used in the treatment of metastatic melanoma. The most common cutaneous side effects are an exanthematous rash and photsensitivity.61 SJS/TEN, DRESS, seborrheic dermatitis, and acneiform eruptions have also been reported.83–86 Development of verrucal keratoses, keratoacanthomas, squamous cell carcinoma in situ, and invasive squamous cell carcinoma are seen in approximately 10% of
669 Chemotherapeutic agents
A B
C D
patients (Fig. 14.102).61 Trametinib, an inhibitor of MEK1 and MEK2 of the MAPK pathway, is associated with exanthematous rashes and acneiform eruptions, but not cutaneous squamous cell carcinoma.61,87 Erythema nodosum-like lesions have also been associated with this group of drugs.88
Immunotherapy checkpoint inhibitors are a new chemotherapeutic option for treatment of melanoma. Ipilumimab, an anti-CTLA-4 immunotherapy, may be complicated by pruritus, a morbilliform rash, vitiligo, and, less commonly, prurigo nodularis, lichenoid dermatitis, pyoderma-gangrenosum-like ulcerations, photosensitivity, radiation recall, TEN, alopecia, and DRESS.89 Nivolumab and pembrolizumab are anti-PD-1 antibody immunotherapies. Morbilliform drug eruptions, lichenoid dermatitis, and vitiligo are the most common adverse cutaneous reactions.90 Psoriasiform dermatitis, lupus erythematosus, and pemphigoid-like reactions have also been reported as side effects.89,90
from lichen planus-like changes (including hyperkeratosis, hypergranulosis, acanthosis, basal cell hydropic degeneration, and apoptosis) to lupus erythematosus-like reactions in which the epidermis is markedly atrophic. The combination of interface changes with severe maturation arrest (dysmaturation) is pathognomonic of chemotherapy-related reactions. It is particularly a feature of patients receiving long-term chemotherapy, high-dose chemotherapy, and multiagent chemotherapy. In addition to impaired maturation, the epidermis appears disorganized and individual keratinocytes are enlarged with pleomorphic nuclei containing conspicuous nucleoli (Fig. 14.106). These changes are particularly associated with bleomycin, busulfan, and hydroxyurea. Eccrine squamous syringometaplasia (squamous metaplasia of the dermal sweat ducts) may be seen with a variety of chemotherapeutic agents including methotrexate, bleomycin, pegylated liposomal doxorubicin, vincristine, dabrafenib, vemurafenib, tamoxifen, and docetaxel.94–102 Checkpoint inhibitor reactions most frequently result in a lichenoid interface dermatitis that shows significant histologic overlap with lichen planus (Fig. 14.107).103 The epidermis also exhibits acanthosis but lacks the dysmaturation of traditional chemotherapeutic agents.
Histologic features The histologic features largely depend on the type of drug reaction seen in the patient. Interface dermatitis represents the most frequently encountered histologic appearance in chemotherapy adverse drug reactions (Figs 14.103–14.105).90–93 In addition to the epidermis, both follicular and sweat gland/duct epithelium may be affected. Appearances are variable, ranging
Etoposide, a podophyllin derivative, in addition to causing maturation abnormalities, can cause metaphase arrest with characteristic fragmented nuclear chromatin resulting in so-called ‘starburst cells’.104
670 Cutaneous adverse reactions to drugs
Hyperpigmentation complicating busulfan therapy predominantly affects the basal layer of the epidermis but may also extend throughout the full thickness and is often accompanied by pigmentary incontinence due to melanocyte toxicity.105 Similarly, bleomycin-induced hyperpigmentation is characterized by epidermal hyperpigmentation and pigmentary incontinence.106 Melanocytes are present in normal numbers. The early inflammatory phase is characterized by a superficial perivascular infiltrate of lymphocytes, histiocytes, occasional neutrophils, plasma cells, and eosinophils. Some authors, however, have described basal cell pigmentation in the absence of pigmentary incontinence.28,107 Lymphocytic vasculitis has also been reported.29
Thio-TEPA-induced pigmentation is similarly characterized by melanin pigment within all layers of the epidermis including the stratum corneum, accompanied by basal cell hydropic degeneration and pigmentary incontinence.34 A mild perivascular lymphohistiocytic infiltrate is present in the superficial dermis. The melanocyte concentration is normal.
Radiation recall is characterized by epidermal atrophy, basal cell hydropic degeneration, and superficial dermal vascular ectasia.
671 Chemotherapy-associated eccrine gland reactions
In addition to anagen alopecia and interface changes, pustular folliculitis and allergic contact dermatitis (5-fluorouracil) may be a feature of chemotherapy-associated adverse reactions, particularly with dactinomycin and 5-fluorouracil.108,109
Hypersensitivity reactions including urticaria, angioedema, and maculopapular eruptions are histologically no different from other drug-induced lesions (see above).
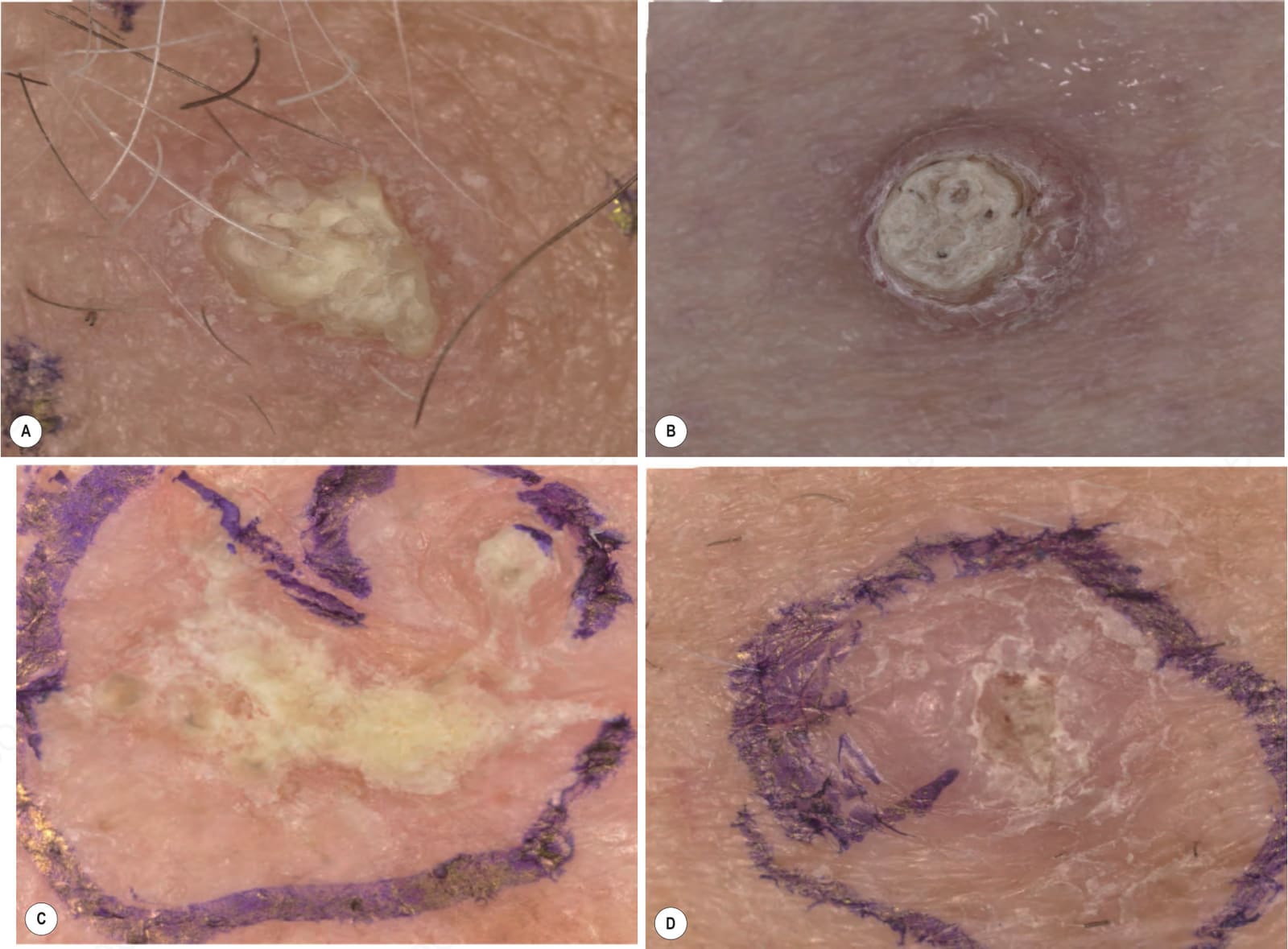
Fig. 14.102 Keratotic lesions seen in patients on vemurafenib including: (A) verrucal keratosis; (B) keratoacanthoma; (C) squamous cell carcinoma in situ; (D) invasive squamous cell carcinoma. By courtesy of Klaus Busam, MD, Memorial Sloan Kettering Cancer Center, New York, New York, USA.

Fig. 14.103 Lichenoid dermatitis secondary to Nivolumab. By courtesy of Adrienne Choksi, MD, MD Anderson Cancer Center, Houston, Texas, USA.
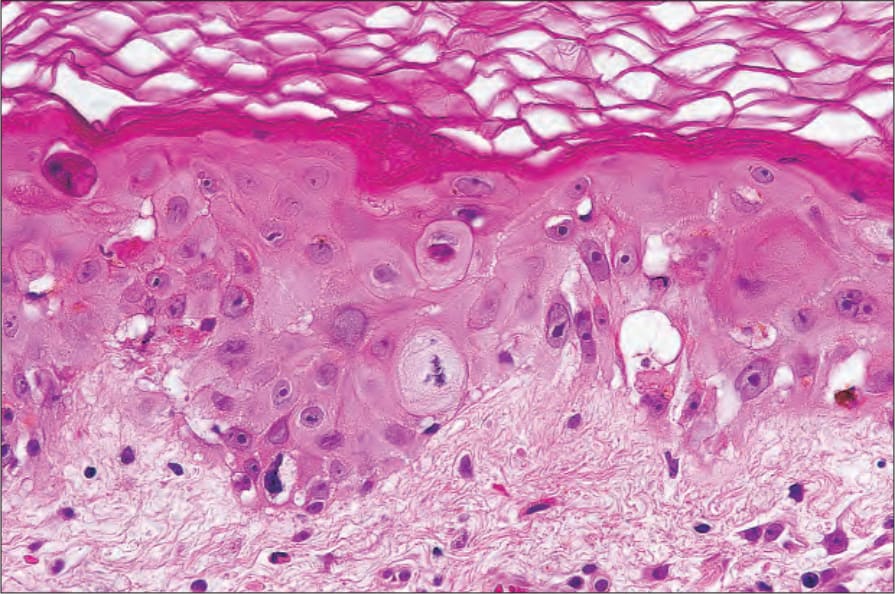
Fig. 14.106 Chemotherapy-related drug reaction: close-up view.
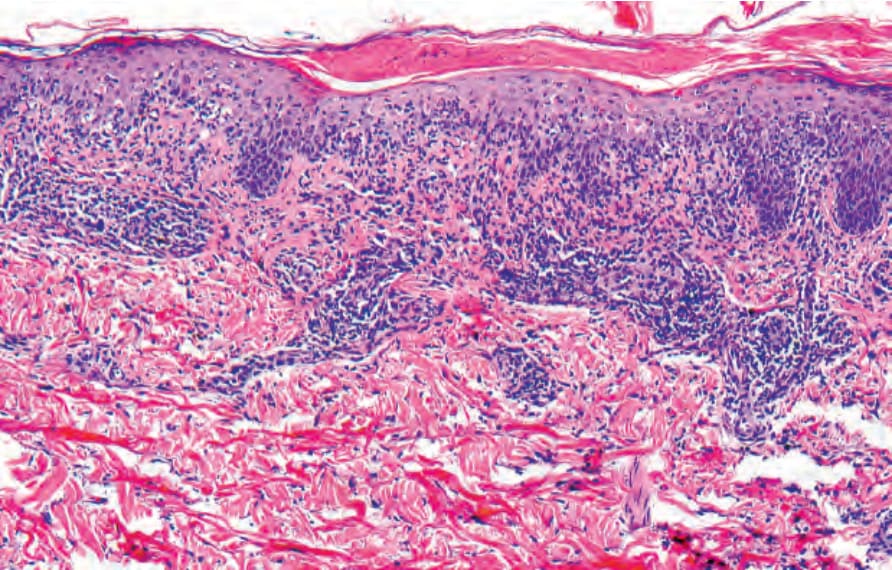
Fig. 14.107 Lichenoid interface drug reaction secondary to PD1 inhibitor. By courtesy of Michael T. Tetzlaff, MD, PhD, The University of MD Anderson Cancer Center, Houston, Texas, USA.