Mercury
Mercury
Clinical features Mercury exposure is encountered under a variety of circumstances.1–3 It occurs in three different forms: metallic, inorganic, and organic mercury.1
• Metallic mercury, which is a liquid at room temperature, is present in vapor from heating amalgam and paints and in mercury thermometers.4
• Inorganic mercurial salts may be present in laxatives, pesticides, antiseptics, and germicides.1,5
• Organomercurials are used as industrial antifungal agents.4
Dermatological reactions to metallic mercury include mercury granuloma and mercury exanthem (mercury-induced AGEP). Mercury granuloma follows penetrating skin wounds as might result from a broken thermometer, attempted homicide, or suicide. Patients present with a flesh-colored to red or hyperpigmented nodule at the site of implantation.6–10 Membranous fat necrosis following subcutaneous mercury injection has also been documented.11 Mercury exanthem follows exposure to metallic mercury (as may follow breaking a thermometer) in a previously sensitized patient.12–22 The eruption presents as a vivid erythema, which particularly affects the flexural sites of the body (so-called ‘Baboon syndrome’).17 An inverted V-shaped erythema affecting the upper anteromedial aspects of both thighs is characteristic.12,16 Sterile pustules commonly develop and a purpuric element may develop. Pyrexia and peripheral leukocytosis are typically present. The dermatosis resolves by desquamation.
Topical mercury cream has been (and is still in some countries) used as a skin-bleaching agent.6,23–26 Continuous and protracted use results in slate-gray pigmentation affecting the flexures. The eyelids, nasolabial folds, and neck creases are sites of predilection.27,28
Parenteral use of mercury results in pigmentation of the gingivae.28 A lichenoid drug reaction has been documented following acute mercury poisoning.29
Dental workers are at risk of allergic contact dermatitis from exposure to mercury or mercury salts.30
Mercury may also be associated with palmar/plantar peeling in children (pink disease, acrodynia, erythredema), palmar/plantar hyperkeratosis, and acanthosis nigricans-like skin lesions.31 Pink disease is rarely encountered nowadays due to control of mercury in medications and in the environment.32–34 The condition is still occasionally seen and may be a problem in developing countries. It presents in infants and young children following chronic mercury exposure, for example, in diaper powders, laxatives, paint, fluorescent light bulbs, or other household sources.1 It is characterized by the development of characteristic painful swelling and pink coloration of the tip of the nose, fingers, and toes.1,11 As the condition resolves, the palms and soles show intense sweating and desquamation.1 Sterility in males is a potential long-term sequel.33
adrenals, muscle, and brain (Fig. 14.90).1 Argyria initially presents in the gingivae as a slate-blue line due to deposition of metallic silver and silver sulfide.1–3 Cutaneous manifestations affect the sun-exposed sites of the face, neck, and backs of hands.6 The nails may also be involved. Ocular involvement presents as a bluish-gray to brownish-black coloration.
Lichenoid and granulomatous inflammatory reactions may complicate use of mercuric sulfide (cinnabar) to provide the red color in tattoos.35–37 Pseudolymphomatous reactions to mercury have also been documented.38,39
Amalgam tattoo reactions are discussed elsewhere.
Localized argyria has been documented due to silver earrings, orthodontic surgery, acupuncture, silver polishing, and the application of topical silver sulfadiazine.10–19 In the absence of clinical information, a diagnosis of blue nevus may mistakenly be made.11,20
Histologic features Argyria results from deposition of metallic silver and silver sulfide. Pigmentation is intensified by sunlight due to silver reduction analogous to photographic processing.6 There is also increased epidermal melanin synthesis.
Silver granules are found in association with the vascular and adnexal basement membranes and adjacent to dermal elastic fibers (Fig. 14.91).2,21 They measure less than 1.0 µm in diameter and appear brown-black in hematoxylin and eosin stained sections.6 Rarely, argyria can have some overlap with ochronosis.22 Ultrastructurally, the silver granules may be membrane bound within macrophage lysosomes or lie freely in the dermis.8 The diagnosis can be confirmed by X-ray microanalysis.6,9,21
Histologic features Mercury pigment is brown-black, round, and opaque, and measures up to 340 µm in diameter (Fig. 14.92).5–7,40 The granules are found within macrophages in addition to extracellular dermal deposition. They are localized around the superficial vasculature and in association with the connective tissue elements.40
Mercury granulomata are characterized by local necrosis associated with free mercury globules surrounded by an intense foreign body granulomatous reaction with lymphocytes, histiocytes, plasma cells, neutrophils, and varying numbers of eosinophils.6,7,9 Ulceration is common, and the epidermis may show pseudoepitheliomatous hyperplasia.
Mercury exanthem is characterized by subcorneal and/or intraepidermal pustules which may contain acantholytic keratinocytes in addition to large numbers of neutrophils.13 Background spongiosis is usually evident. The dermal papillae are often edematous, and occasionally subepidermal vesiculation is a feature. A perivascular infiltrate of lymphocytes and histiocytes
665 Specific drug reactions
with conspicuous neutrophils and variable numbers of eosinophils is present in the superficial dermis. Leukocytoclastic vasculitis may be a feature in a significant proportion of cases.13
Cutaneous pigmentation following chronic local exposure to mercury is characterized by increased melanin pigment in the epidermis accompanied by mercury granules in the papillary dermis.26 Iron stains are negative.1
Pink disease is characterized by sweat gland hyperplasia and a non-specific dermal inflammatory cell infiltrate.1

Fig. 14.90 Argyria: there is striking slate-blue pigmentation; the eyes are also affected. By courtesy of the Institute of Dermatology, London, UK.
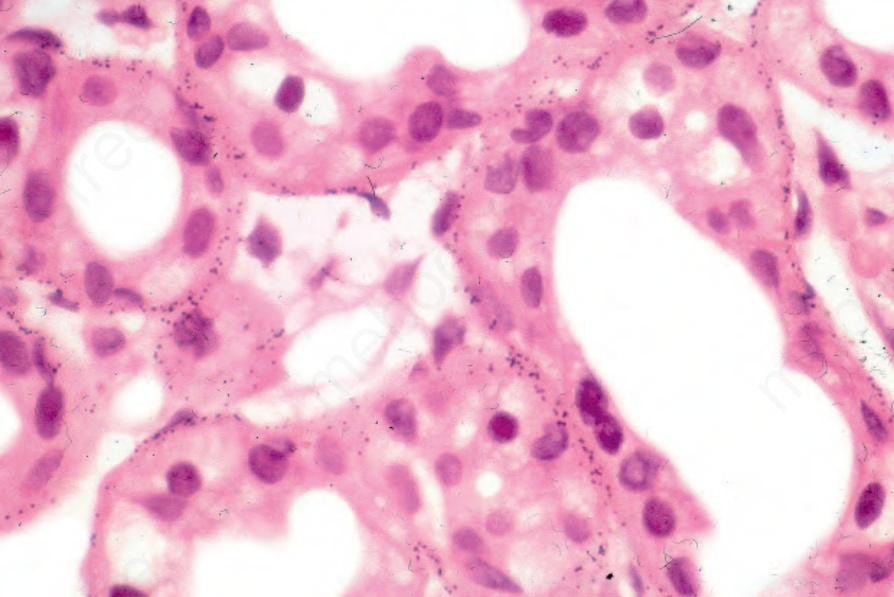
Fig. 14.91 Argyria: note the fine silver granules outlining the basement membrane of the sweat gland epithelium.
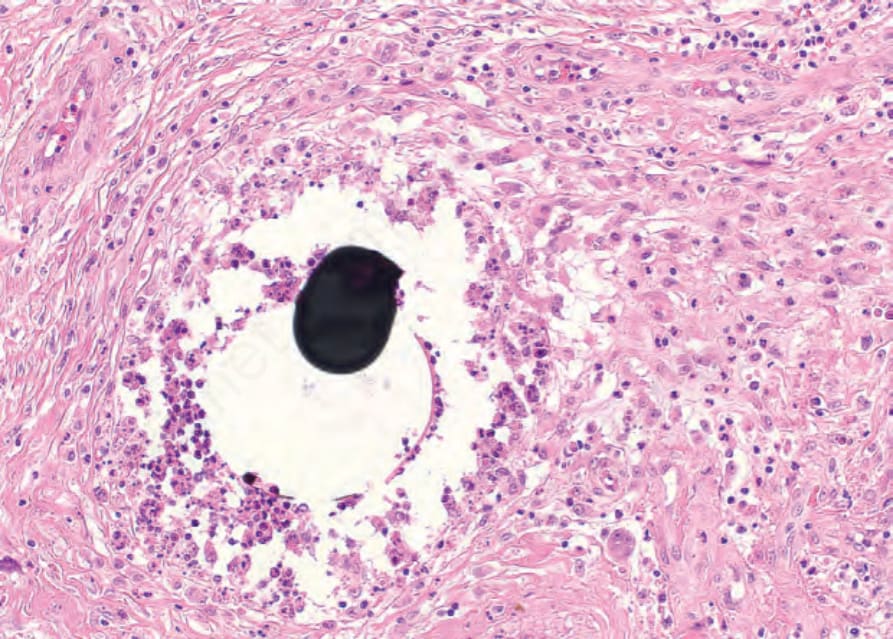
Fig. 14.92 Mercury pigmentation: the round black deposit of mercury is surrounded by a suppurative granuloma.
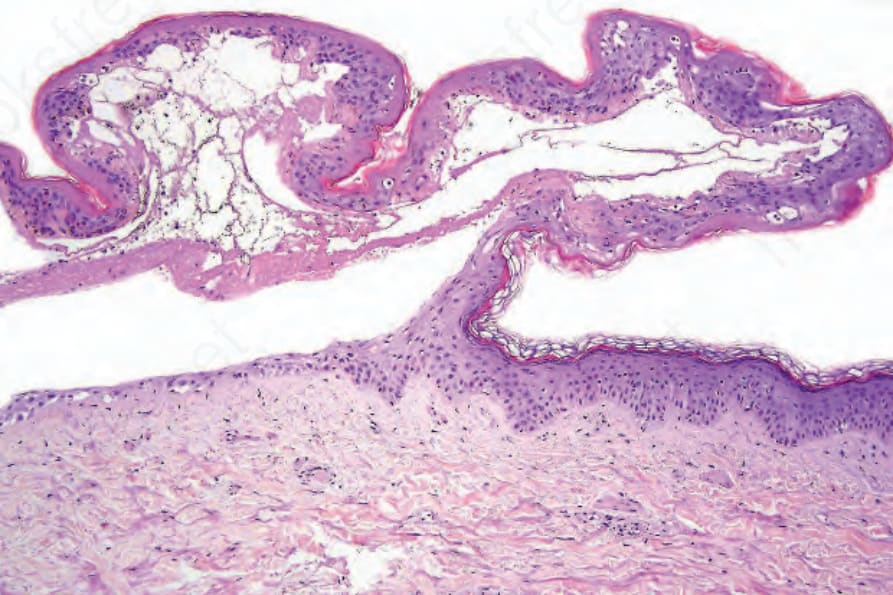
Fig. 14.93 Coma blister: there is a subepidermal blister. Re-epithelialization along the floor is present.