Gold
Gold
Clinical features Gold therapy may result in eczematous, lichenoid, pityriasiform, and psoriasiform dermatoses and stomatitis.
Cutaneous pigmentation that results from parenteral treatment with gold salts is known as chrysiasis (auriasis, chrysoderma, hautaurosis).1–5 It is a photodependent, irreversible condition most often documented in patients with rheumatoid arthritis.2,3 Patients are at risk once a threshold of 50 mg/kg of gold is reached.1 Disease severity correlates with the cumulative dose of gold.6 Coloration varies from mauve/blue to blue to slate-gray.2 The sun-exposed skin of the face is particularly affected. In severe cases, lesions may be seen on the neck, front of chest, and backs of the forearms
663 Specific drug reactions
and hands (Fig. 14.88).2 In bald patients, scalp involvement is sometimes apparent. Pigmentation has also been described in the sclera and buccal mucosa.2
Pathogenesis and histologic features The pathogenesis of chrysiasis is uncertain. It is probably related to an effect of UV radiation on tissue-bound gold particles. Support for this hypothesis is the observation that skin lesions can be induced by UVB irradiation of sunlight-protected skin.7 Similarly, typical skin lesions have been described following Q-switched ruby laser treatment in patients treated with gold.8–11
Differential diagnosis Gold pigment must be distinguished from silver deposits (argyria), mercury, and tattoo pigment.5,10 Silver pigment is predominantly deposited in relation to basement membranes, particularly of the sweat glands. It does not show orange-red birefringence with cross-polarized light.10 Mercury particles are large (up to 340 µm in diameter) and brown-black in color. Tattoo usually consists of a variety of different pigments of varying colors. Clinical history should readily establish the diagnosis in the majority of cases.
Chrysiasis is characterized by deposits of small black macrophage-bound particles surrounding the vessels in the deeper reticular dermis and around the sweat gland coils (Fig. 14.89).2 Perls Prussian blue (hemosiderin) and Masson-Fontana staining for melanin are negative. The gold particles show orange-red birefringence with cross-polarized light.12 There is no inflammatory response. Epidermal melanin pigmentation usually appears normal.2 A localized form of chrysiasis with sclerosing lipogranulomas at injection sites has also been reported.13
By electron microscopy, the gold appears as granular, particulate, and filamentous material, sometimes showing a starlike morphology within phagolysosomes (aurosomes). The diagnosis can be confirmed by electron/Xray probe microanalysis.2,4,13–16
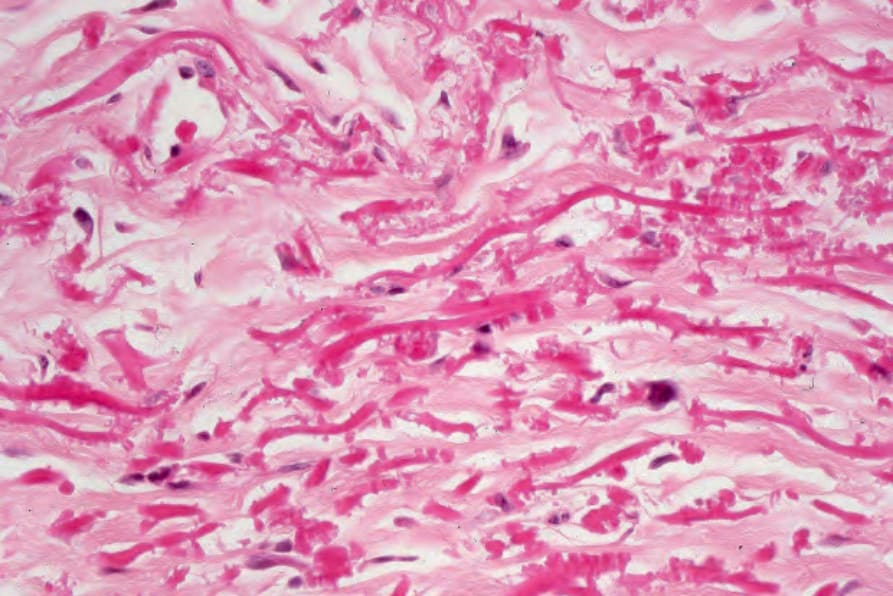
Fig. 14.86 Penicillamine dermopathy: the serrated appearance is characteristic.
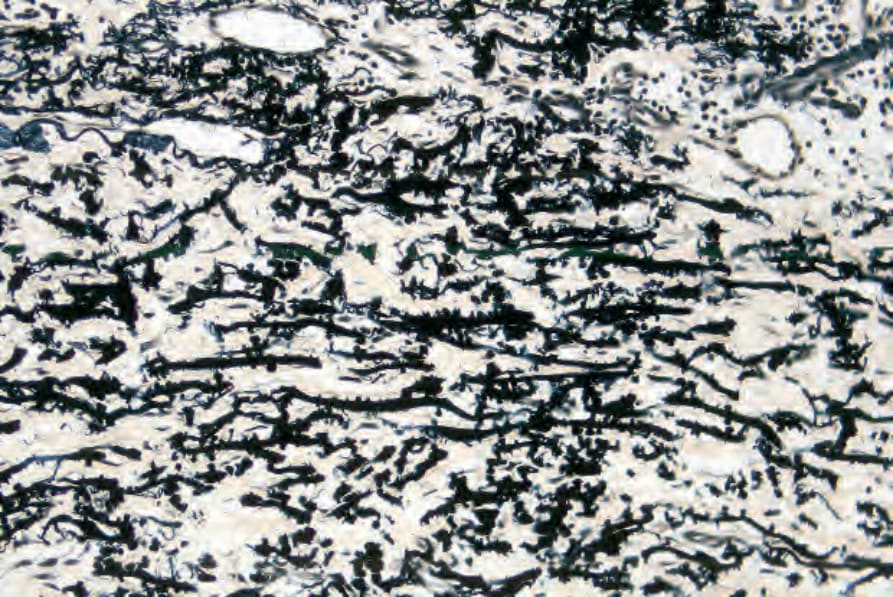
Fig. 14.87 Penicillamine dermopathy: the changes can be highlighted by an elastic tissue stain.

Fig. 14.88 Chrysiasis: multiple foci of blue discoloration are present on the cheek. By courtesy of J. Kerner, MD, Department of Dermatology, Harvard Medical School, Boston, USA.
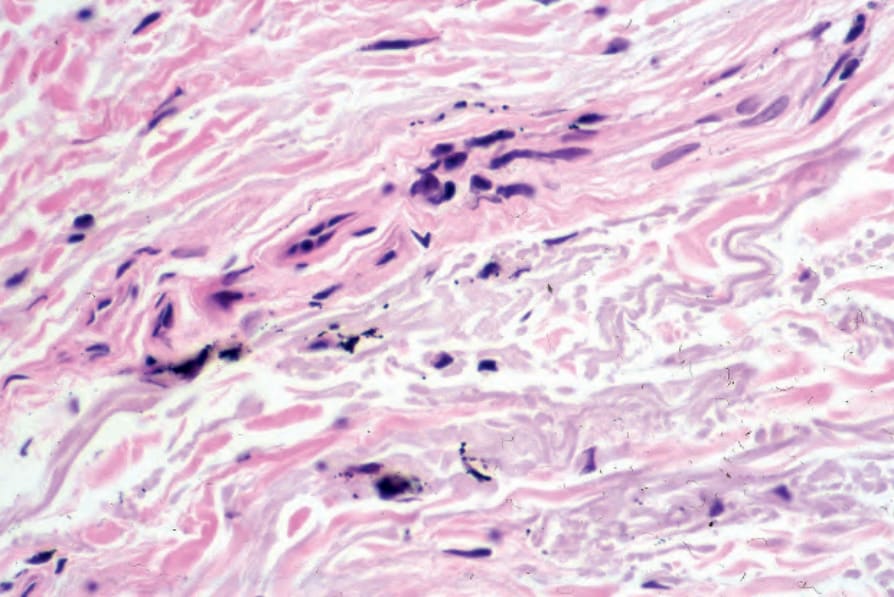
Fig. 14.89 Chrysiasis: there are fine black granules both within macrophages and lying free around the superficial vasculature. By courtesy of S. Lyle, MD, Beth Israel Deaconess Medical Center, Boston, USA.