Heparin
Heparin
Adverse side effects of heparin include hemorrhage, urticaria, anaphylaxis, macular erythema, and alopecia.1–3 Of greater significance, patients may develop thrombocytopenia, paradoxical thrombosis, and skin necrosis – HIT syndrome.1–6
Clinical features Urticarial reactions are exceptionally rare.7–9 Delayed hypersensitivity reactions are the most common of the adverse cutaneous responses to heparin, occurring in 7.5% of patients.9,10 Macular erythema and eczematous lesions occur at the injection site. There is a striking female predominance.2,11 Rarely, blisters may develop, and exceptionally the erythema becomes generalized.10
Hemorrhagic vesicles have also been described in patients given low molecular weight heparin.12,13 Reported patients have been elderly and received the medication while hospitalized. Lesions develop distant from injection sites and occur on the extremities.
HIT syndrome – in addition to definitional thrombocytopenia – is characterized by thrombosis (venous more often than arterial), which accounts for the high morbidity and potential mortality.4,6 Venous thrombosis results in deep venous lesions in the lower legs in up to 50% of patients, and of these 25% may develop pulmonary embolism.6 Additional complications include warfarin-induced limb gangrene, adrenal hemorrhage, and DIC.6 Arterial thrombosis is more likely in catheterized or traumatized arteries and may affect the aorta and ileofemoral arteries, resulting in peripheral gangrene, myocardial infarction, or stroke.4,6,14
Cutaneous necrosis develops in 10–20% of patients with the HIT syndrome.6,15 The injection site is predominantly involved, but more distant areas (thighs, abdomen, and buttocks) may also be affected in a minority of patients.1,2,16–25 Initial lesions are painful or burning erythematous plaques followed by ulceration and tissue necrosis.2 The condition shows a predilection for middle-aged females and the obese.2,16
Thrombocytopenia and thromboembolism are potentially life-threatening complications.
Pathogenesis and histologic features The HIT syndrome results from platelet activating HIT/PF4 antibodies induced in response to a platelet factor 4-heparin complex.1,23,24 The resulting immune complexes bind to platelet Fc receptors and activate platelets. In addition, the antibody reacts with surface endothelial cell platelet factor 4-inducing endothelial cell injury and thrombosis.4,24 Only a minority of patients with HIT antibodies develop skin necrosis, and it is postulated that additional prothrombotic factors such as protein C or S deficiency are necessary for the development of thrombosis and its sequelae.1 Adverse side effects are more common and more severe in patients receiving unfractionated as opposed to low molecular weight heparin.25 Extensive necrosis has been triggered by low molecular weight heparin in a patient with underlying lupus erythematosus and antiphospholipid syndrome.26
dermatoses, alopecia, hypertrichosis, nail changes, dermatomyositis, systemic lupus erythematosus, pemphigus vulgaris, pemphigus foliaceus, pemphigus erythema, and bullous and mucosal pemphigoid.1–13 The autoimmune blistering dermatoses complicating penicillamine therapy are not dose dependent and are seen particularly in patients with other immunologically mediated diseases including rheumatoid arthritis and systemic sclerosis.9 Pemphigus is by far the most common bullous disorder associated with penicillamine, pemphigus foliaceus being the most frequent variant encountered.4,9 Herpetiform pemphigus has also rarely been described as complicating the use of penicillamine.10,11 Additional manifestations – particularly seen in patients taking high doses in the treatment of Wilson disease and cystinuria – include penicillamine dermopathy, elastosis perforans serpiginosa, skin fragility with hemorrhages and milia formation on the extensor surfaces, wrinkling and anetoderma-like changes, cutis laxa, and pseudoxanthoma elasticum-like appearances.13–20 Patients on long-term therapy may present with small yellow papules resembling a plucked-chicken appearance or disfiguring loose folds of skin particularly affecting the flexures.17,18
The histologic features of the macular erythema are those of spongiotic dermatitis. Within the superficial dermis is a perivascular lymphohistiocytic infiltrate with variable numbers of eosinophils. The lymphocytes are predominantly of the T-helper subclass.27
Pathogenesis and histologic features Penicillamine acts by impairing cross-linking in newly formed collagen and elastic fibers.14 It also binds aldehydes to the surfaces of macrophages and amine groups on T cells, and this could represent a mechanism for triggering autoimmune reactions. contributing to an autoimmune reaction.21,22 The histologic features include increased numbers of abnormally formed elastic fibers in the reticular dermis (Fig. 14.85). These are thickened with irregular serrated appearance on cross section. When viewed in a longitudinal plane, the fibers show conspicuous lateral projections (Figs 14.86 and 14.87).
Evidence of similar elastic tissue damage has been documented in the joint capsules, lungs, intestine, and large elastic arteries.14
Heparin-induced cutaneous necrosis is characterized by widespread superficial small vessel (capillary and venule) thrombi accompanied by hemorrhage and necrosis.17,18 The presence of leukocytoclastic vasculitis is variable.2
Bullous hemorrhagic lesions are intraepidermal blisters filled with extravasated red blood cells.12,13 Perivascular lymphocytes, histiocytes, and eosinophils are variably present. Leukocytoclastic vasculitis is absent. Direct immunofluorescence studies are negative.
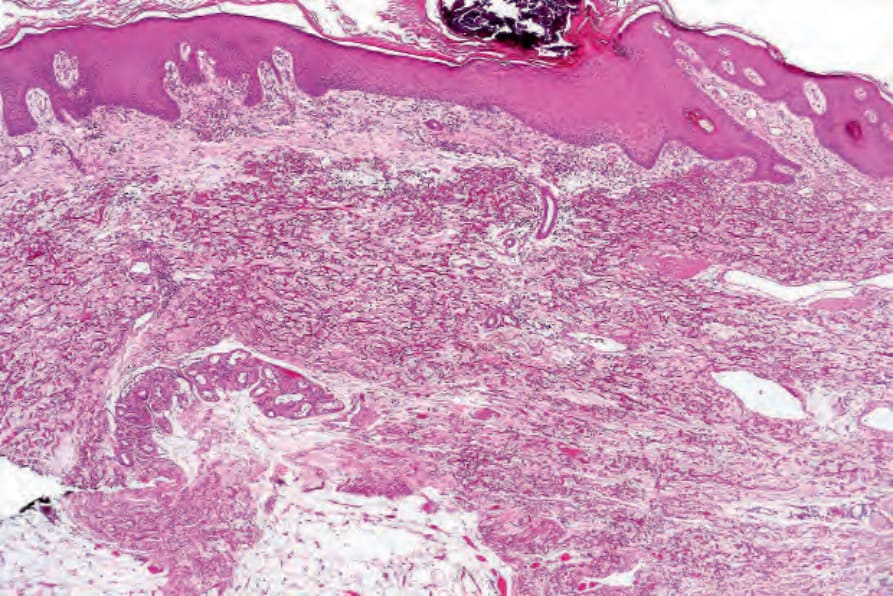
Fig. 14.85 Penicillamine dermopathy: there are thickened, intensely eosinophilic elastic fibers throughout the reticular dermis.
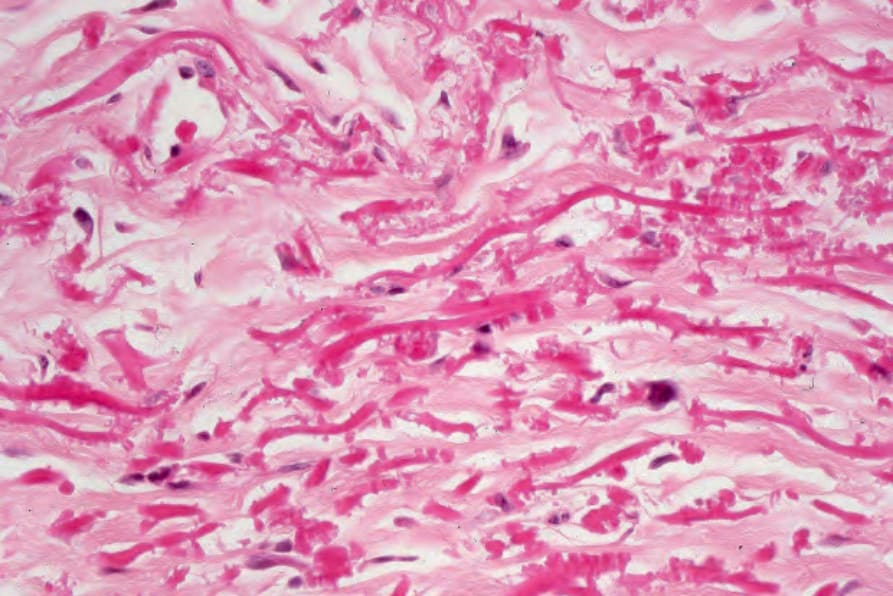
Fig. 14.86 Penicillamine dermopathy: the serrated appearance is characteristic.