Warfarin
Warfarin
Warfarin (coumadin) may be associated with a number of adverse reactions including hemorrhage, alopecia, urticaria, maculopapular eruptions, dermatitis, purple toe syndrome, and leukocytoclastic vasculitis.1–8 Cutaneous necrosis develops in 0.01–0.1% of patients and may cause severe morbidity and significant mortality.5
661 Specific drug reactions
Clinical features Warfarin necrosis typically develops 3 to 6 days after starting anticoagulation therapy. Paresthesia is present initially and is followed by a painful, well-circumscribed, edematous, and erythematous plaque resembling peau d’orange with purpura.1,5 Large blood-filled blisters that rapidly break down, accompanied by progressive necrosis of the underlying dermis and subcutaneous fat, are later sequelae. Tissue destruction is often considerable and the resultant scarring is very disfiguring. Occasionally, the onset of this condition is delayed for weeks or months, although in most instances this reflects an interrupted therapeutic regimen.9–11
The condition shows a predilection for obese females (85%) and predominantly affects the breasts, buttocks, and thighs.2 The reason for the female predominance is unknown. In males, the thighs and buttocks are also affected and sometimes the penis is involved. Occasionally, lesions are seen on the hands. Deeper soft tissues and internal viscera are not affected.
Patients almost invariably have received anticoagulation for thrombophlebitis (deep venous thrombosis) and/or pulmonary embolism. Patients who receive warfarin for treatment of cardiovascular disorders such as atrial fibrillation only very exceptionally develop this condition.5
Pathogenesis and histologic features Cutaneous necrosis rarely complicates therapy with warfarin. Although hypersensitivity reactions and direct toxicity have been postulated as etiological factors, an imbalance in the ratio of procoagulative and anticoagulative factors is currently thought to be most important.5 In addition to depressing the vitamin K-dependent clotting factors II, VII, IX, and X, warfarin reduces the levels of naturally occurring anticoagulants including protein C, protein S, and antithrombin III. It first affects protein C, which has an extremely short half-life, and until the anticoagulative effect comes into play with depressed levels of coagulating factors, the patient is paradoxically at increased risk of thrombosis. Why this should so rarely result in skin necrosis is uncertain.
Congenital protein C deficiency is an important predisposing factor in some patients. This is a relatively common autosomal dominant condition that affects between 1 : 200 and 1 : 300 of the population. Protein C is activated by thrombin under the influence of the cofactor thrombomodulin.5 The activated form inactivates factors VIIIa and Va, which inhibit conversion of factor X to factor Xa and prothrombin to thrombin with resultant inhibition of coagulation.5 Protein C deficiency is, therefore, associated with a thrombotic tendency.12 Approximately 30% of patients who develop warfarin necrosis have an underlying protein C deficiency.2 Warfarin therapy, therefore, tips the balance in an already protein C-deficient patient. The proposed mechanism, however, by no means offers an explanation in the majority of cases.
conditions that predispose to the development of warfarin necrosis include reduced antithrombin III levels, lupus anticoagulant syndrome, factor V Leiden, and prothrombin gene mutation.19–21
Histologically, warfarin-associated skin necrosis is characterized by fibrin thrombi in the small veins and venules of the dermis and subcutaneous fat, with widespread erythrocyte extravasation (Figs 14.83 and 14.84). In advanced lesions, subepidermal blood-filled blisters are seen. In older lesions, the changes of infarction are superimposed; however, vasculitis is not typically a feature. However, warfarin-induced leukocytoclastic vasculitis has been reported.22,23 Arteries are not affected.
Acquired or congenital deficiency of protein S may also be of importance in a small number of cases.13–16 Protein S is a vitamin K-dependent cofactor for activated protein C.5 Acquired protein S deficiency may be encountered in patients with renal failure or antiphospholipid syndrome, or who are undergoing hemodialysis.17,18
An episode of thrombophlebitis and/or pulmonary embolism leading to the warfarin therapy seems to be of major etiological importance.1,2 It is proposed that the vascular inflammatory changes play a role in precipitating the thrombotic tendency by reducing endothelial cell thrombomodulin levels, inactivating protein S and decreasing fibrinolytic activity.1–4 Protein C or protein S deficiency (inherited or developing as a consequence of warfarin therapy) may then represent an additional predisposing factor. Other
Differential diagnosis Identical histologic features may be seen in a number of conditions including antiphospholipid antibodies, hereditary hypercoagulation disorders (factor V Leiden mutations, protein C or S, and antithrombin III deficiencies) in the absence of warfarin therapy, heparin-induced thrombocytopenia (HIT) syndrome, and disseminated intravascular coagulation (DIC). Cryoglobulinemia and cryofibrinogenemia may also have to be excluded. Calciphylaxis can be excluded by the absence of vascular calcification. The diagnosis ultimately depends upon adequate clinicopathological correlation.
662 Cutaneous adverse reactions to drugs
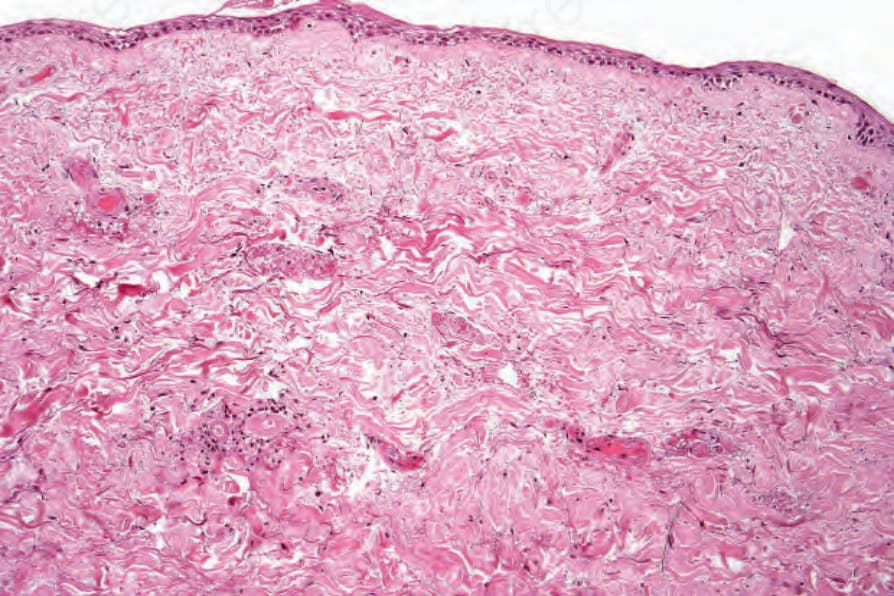
Fig. 14.83 Warfarin necrosis: there are thrombosed vessels throughout the superficial dermis associated with epidermal regeneration.
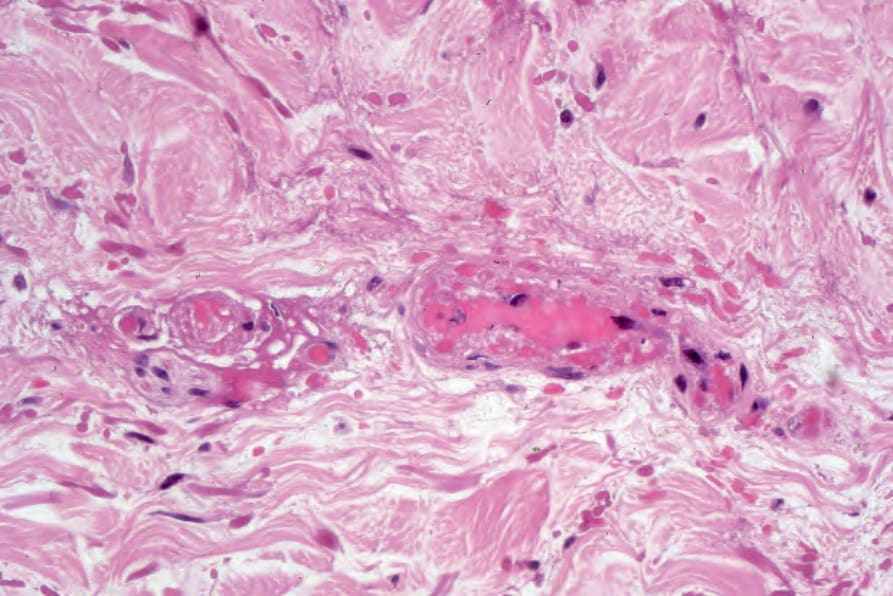
Fig. 14.84 Warfarin necrosis: high-power view of Fig. 14.83.