Bromoderma
Bromoderma
Clinical features Methyl bromide has been used as a pesticide and disinfectant and in the pharmaceutical, film, and dye industries.1–5 It may be found in sedative syrups and expectorants. Although occupational exposure is associated with severe respiratory effects including pulmonary edema, occasional reports of skin contact have also been documented.3,4 Potassium bromide is used as an anticonvulsant in many parts of the world. Other sources of exposure include brominated pool disinfectants and brominated vegetable oil, a product used in citrus-flavored drinks.6 In Japan and other countries, over-the-counter bromide-containing sedatives can be a source of exposure.7 Bromoderma has also been reported in a patient with a pituitary adenoma treated with bromocriptine.8
Patients present with sharply circumscribed erythematous lesions containing vesicles and bullae.4 Intertriginous regions and sites of mechanical pressure are predominantly affected. Ingested bromide may give rise to hyperpigmentation, urticaria, acneiform/pustular lesions (acne bromica), vegetative and ulcerated plaques (vegetant bromoderma, tuberous bromoderma), necrotizing panniculitis, and pyoderma gangrenosum-like ulcers (Fig. 14.82).7,9–14 Lesions may be multiple or solitary. Vegetant bromoderma most often presents on the face, scalp, and legs and predominantly affects infants.8 It is commonly mistaken for an infection. A case which complicated bromine secretion in breast milk has been documented.15
Histologic features Cutaneous lesions that develop following acute exposure to methyl bromide are characterized by spongiosis, keratinocyte necrosis, papillary dermal edema, and subepidermal blister formation.4 A perivascular inflammatory cell infiltrate containing neutrophils, eosinophils, and smaller numbers of lymphocytes and histiocytes is present in the superficial dermis.
characterized by an intense dermal neutrophil-rich infiltrate. With chronicity, pseudoepitheliomatous hyperplasia and ulceration are common. Neutrophil microabscesses may be seen in the epidermis and the dermis; in some cases, there is focal leukocytoclastic vasculitis.3,5
Differential diagnosis Histologically, the nodular lesions of iododerma resemble an infective process such as blastomycosis or an atypical mycobacterial condition. The presence of occasional eosinophils within the infiltrate and epidermal degeneration in association with the abscesses may result in confusion with pemphigus vegetans. In early lesions, when the epidermis is normal thickness, the features can be mistaken for Sweet syndrome and pyoderma gangrenosum.
In vegetating lesions, there is striking pseudoepitheliomatous hyperplasia with intraepidermal and dermal abscesses accompanied by an intense neutrophil, eosinophil, and lymphohistiocytic infiltrate in the underlying dermis. Ulceration resembling pyoderma gangrenosum may be present.7
Urticarial lesions show papillary dermal edema accompanied by a neutrophil and eosinophil-rich infiltrate.4
Differential diagnosis Vegetating lesions may be easily confused with deep fungal and atypical mycobacterial infections. Pemphigus vegetans also enters the differential diagnosis. Sweet syndrome and pyoderma gangrenosum also have some
similarities. The diagnosis may be most easily reached by careful clinicopathological correlation.13

Fig. 14.81 Iododerma: in this patient, nodules are conspicuous. Superimposed pustules are evident. By courtesy of the Institute of Dermatology, London, UK.
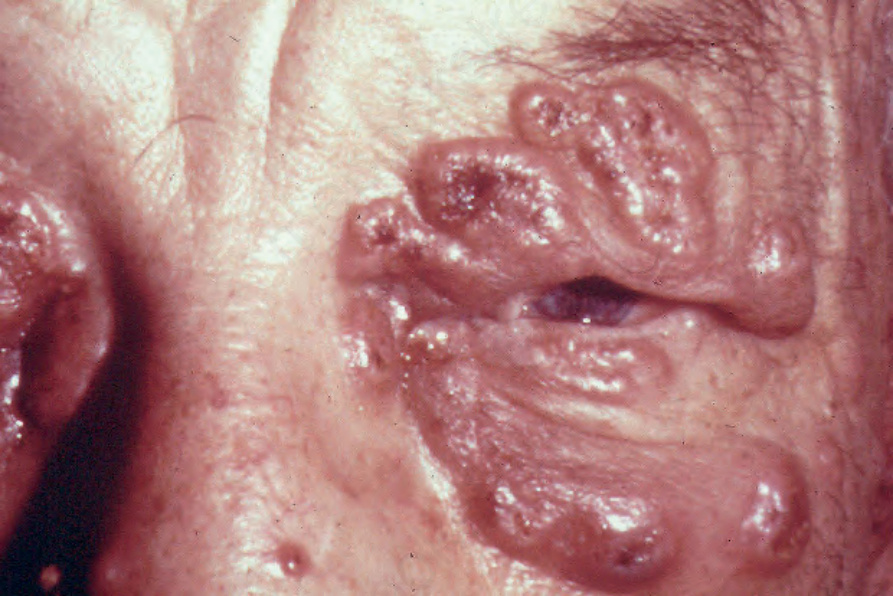
Fig. 14.82 Bromoderma: vegetant plaques and nodules are seen around the eye. Ulceration is present. By courtesy of the late M. Beare, MD, Royal Victoria Hospital, Belfast, N. Ireland.