Drug-induced pseudolymphoma
Drug-induced pseudolymphoma
Clinical features Drug-induced pseudolymphoma includes pseudolymphomatous reactions to systemically administered medications (lymphomatoid drug eruption) and the much less frequent contact variant associated with locally administered agents (lymphomatoid contact dermatitis).1–3
Histologic features The pustules are present in a subcorneal and/or intraepidermal location and sometimes contain a few acantholytic keratinocytes in addition to large numbers of neutrophils (Figs 14.69 and 14.70).3,9 A background of spongiosis is usually evident. The dermal papillae are often edematous, and occasionally subepidermal vesiculation is a feature. A perivascular infiltrate of lymphocytes and histiocytes with conspicuous neutrophils and variable numbers of eosinophils is generally present in the superficial dermis. Leukocytoclastic vasculitis may be a feature in a significant proportion of cases.3,9,11
Differential diagnosis The differential diagnosis includes pustular psoriasis, subcorneal pustular dermatosis, IgA pemphigus, pustular necrotizing angiitis, and acute
Lymphomatoid drug eruptions are commonly a T-cell type, although B-cell lymphomatoid drug eruptions are also recognized. T-cell variants are divided into anticonvulsant-related and nonanticonvulsant-related variants.2
Anticonvulsant-related T-cell lymphomatoid drug eruption typically develops within weeks or months of commencing treatment. Patients present with pyrexia, lymphadenopathy, and an eruption of single or generalized lesions comprising erythematous, morbilliform maculopapules, plaques, nodules or tumors often associated with leukocytosis, circulating Sézary cells, eosinophilia, hepatosplenomegaly, and variable liver dysfunction (Fig. 14.71).2,4–16 Vesicles and purpuric lesions have also been described.14 Sézary syndrome-like features may rarely be seen.17 A number of anticonvulsants have been implicated including phenytoin, primidone, mephenytoin, carbamazepine, phenobarbital, and trimethadione.2
Nonanticonvulsant-related pseudolymphomatous reactions present similarly with single lesions or multiple papules, plaques, and nodules.
657 Drug-induced pseudolymphoma
Associated drugs include antihypertensives, antidepressants, tranquilizers, beta blockers, calcium channel blockers, diuretics, NSAIDs, antibiotics, tyrosine kinase inhibitors, and ciclosporine.2,18–27 Sézary syndrome-like features have also been documented.28
Lymphomatoid contact dermatitis is much less common and usually represents a T-cell reaction to a contact allergen that histologically shows features reminiscent of mycosis fungoides.2,29–41 Patients present with pruritic, localized to generalized scaly papules and plaques.2 A number of antigens have been incriminated including matchbox striking surface antigens, ethylenediamine dihydrochloride, isopropyl-diphenylenediamine, phosphorus, nickel, gold, cobalt naphthenate, para-phenylenediamine, methylisothiazolinone, methylchoroisothiazolinone/methylisothiazolinone and paraben mix, textile dyes, and exotic wood on a toilet seat.
B-cell lymphomatoid drug reaction is rare but has been described in association with fluoxetine hydrochloride, amitriptyline hydrochloride, and levofloxacin.2,21,22,42 Patients present with solitary nodules, multiple infiltrative plaques, or multiple papules.
B-cell lymphomatoid contact reactions may be seen with gold and nickel earrings. Patients present with one or more firm, erythematous nodules at the site of piercing.43–45
B-cell and, less commonly, T-cell pseudolymphomatous reactions may develop within tattoos.46–52 Papules and nodules localized to the tattoo occur months to years after tattoo placement. The most common culprit is red pigment, although reactions to blue, green, and black dyes have been reported.49,50,52 Both metals and organic synthetic pigments are implicated as antigens in such reactions.
Pathogenesis and histologic features The pathogenesis of lymphomatoid drug reactions is not completely understood, but is thought to be secondary to immune dysregulation.27,53 Studies show that medications implicated in drug-induced pseudolymphoma can induce proliferation of T cells and inhibit suppressor T cells, both in vivo and in vitro.53,54 This may lead to an increase in helper T cells as well as B cells, resulting in T-cell and B-cell pseudolymphoma, respectively.
Drug-induced T-cell pseudolymphoma most often presents as a dense superficial perivascular or bandlike infiltrate composed of lymphocytes, histiocytes, and atypical lymphoid cells with irregular, enlarged, and hyperchromatic nuclei (Figs 14.72–14.76).55 Cerebriform variants may be seen, and there is often associated epidermotropism. Pautrier-like microabscesses reminiscent of mycosis fungoides, however, are only occasionally identified. Eosinophils are frequently evident and often the epidermis shows significant spongiosis. Giant cells, collections of histiocytes, and epithelioid granulomata may also be evident. Dense nodular and tumorlike variants
more suggestive of anaplastic T-cell lymphoma may also be encountered (Figs 14.77–14.79). A follicular mucinosis-like variant has rarely been described.22 The infiltrate may also have a prominent angiocentric pattern with numerous immunoblasts.56 A clinical case of AGEP secondary to clindamycin that histologically mimicked a lymphomatoid drug reaction has also been reported.57
658 Cutaneous adverse reactions to drugs
By immunohistochemistry, the infiltrate consists of CD3+ T cells. CD4+ cells most often outnumber CD8+ forms, and CD20+ B cells are either extremely sparse or absent. A CD8+ variant has, however, been described following treatment with gemcitabine and infliximab.58,59 CD30 expression with resultant confusion with an anaplastic large cell lymphoma or lymphomatoid papulosis has also been described.11,24,27,56,59,60
Reported TCR gene rearrangement studies have disclosed a clonal population in only a small minority of patients.5,6,12,14
Lymphomatoid contact dermatitis most often is reminiscent of mycosis fungoides and is characterized by a superficial dermal bandlike infiltrate composed of atypical lymphocytes and histiocytes with variable lymphocyte
epidermotropism. The epidermis is typically acanthotic, and spongiosis may sometimes be present.
Immunohistochemical analysis has been reported in a small number of cases. The atypical lymphocytes usually express CD3 and CD4 with no loss of CD5 and CD7. A CD8 predominant variant has been documented.34
In the limited number of cases in which TCR gene rearrangements have been documented, most disclosed a polyclonal pattern while true monoclonal bands are rare.31,34,36,61
B-cell lymphomatoid drug reactions are characterized by a nodular or diffuse pandermal infiltrate, often accompanied by extension into the subcutaneous fat. The infiltrate consists of lymphocytes and histiocytes with
659 Specific drug reactions
with a diffuse erythematous papular or pustular/bullous dermatosis that can progress to exfoliative dermatitis.5 Transverse white nail striations may be a feature.5 Rarely, TEN can develop.8 Irritant nail dermatitis has also been reported.9 Chronic complications of arsenic exposure include pigmentary disturbances and cutaneous tumors. Patients are also at increased risk of internal malignancies.1,7 Other systemic manifestations include atherosclerosis, hepatic fibrosis, peripheral neuropathy, respiratory disease, and diabetes mellitus.7
Characteristic of arsenicism is the ‘rain drops on a dusty road’ appearance in which patients develop hyperpigmented macules containing foci of hypopigmentation and areas of darker pigmentation.7,10–12 Lesions are often seen on the trunk and in heavily pigmented regions such as the areola and flexural creases.3 The cutaneous pigmentary changes are especially seen in Asian populations.3
Palmar and plantar keratoses are common and present 2 years or more after exposure.5 After many years, they may be associated with malignant transformation.7
Skin tumors are a late manifestation, are often multiple, and are particularly found on non-sun-exposed sites. Bowen disease, squamous cell carcinoma, and superficial basal cell carcinoma may develop.1,2
Patients with evidence of arsenic exposure should be investigated for visceral malignancies, particularly carcinoma of the lung, bladder, and kidney.7,13,14 There are occasional reports documenting an association between arsenic and hepatic angiosarcoma.15,16
variable numbers of plasma cells and eosinophils. Mitoses are sometimes numerous. Blasts are often present and lymphoid follicles with germinal centers may be evident.
By immunohistochemistry, the majority of the lymphocytes are CD20+ B cells although a subpopulation of CD3+ T-cells is also present. Identification of CD21+ follicular dendritic cells may be helpful in confirming the presence of poorly developed follicles. Kappa and lambda immunohistochemistry invariably show no evidence of light chain restriction.
Tattoo-associated pseudolymphomas may be of the B- or T-cell type, with a B-cell pattern being more common. In addition to the features described above, there is tattoo pigment extracellularly and within macrophages. Rarely, a lichenoid infiltrate is present.50
Differential diagnosis Distinction between cutaneous lymphoma and a drug-induced pseudolymphoma can be exceedingly difficult. Features that favor a drug-induced process over mycosis fungoides include vacuolar alteration, keratinocyte necrosis, spongiosis, and papillary dermal edema.53 However, there can be considerable histologic overlap, and rare instances of a TCR gene rearrangement necessitate close clinicopathological correlation. If cutaneous pseudolymphoma is suspected, the most effective way to make the distinction is withdrawal of the suspected drug. It is important that correlation always be undertaken in any case of an unanticipated lymphoma in order that reactive conditions do not receive inappropriate lymphoma treatment. True cutaneous lymphomas may be drug-induced like in the case of CD30(+) anaplastic large cell lymphoma associated with fingolimod used in the treatment of multiple sclerosis.51a
Pathogenesis and histologic features The mechanism of arsenic carcinogenesis is multifactorial. Arsenic is methylated as part of the metabolization process.6 This results in free radicals which damage DNA, contribute to chromosomal aberrations, and increase sister chromatid exchange.7 Arsenic also impairs the DNA repair process and diminishes p53 activity.17 Transcription factors, cytokines, and cell signaling pathways critical to regulation of cellular proliferation and differentiation are also affected by arsenic and lead to uncontrolled cell growth and de-differentiation.7,17,18 Decreased methylation capacities and a specific NALP2 polymorphism are associated with an increased risk of developing arsenic-related skin lesions.19,20
Histologically, cutaneous hyperpigmentation demonstrates increased melanin synthesis, with excess pigment being present at all levels of the epidermis.3 There is no evidence of melanocytic proliferation. Skin cancers arising as a result of arsenic exposure show no distinguishing features histologically and are described elsewhere.
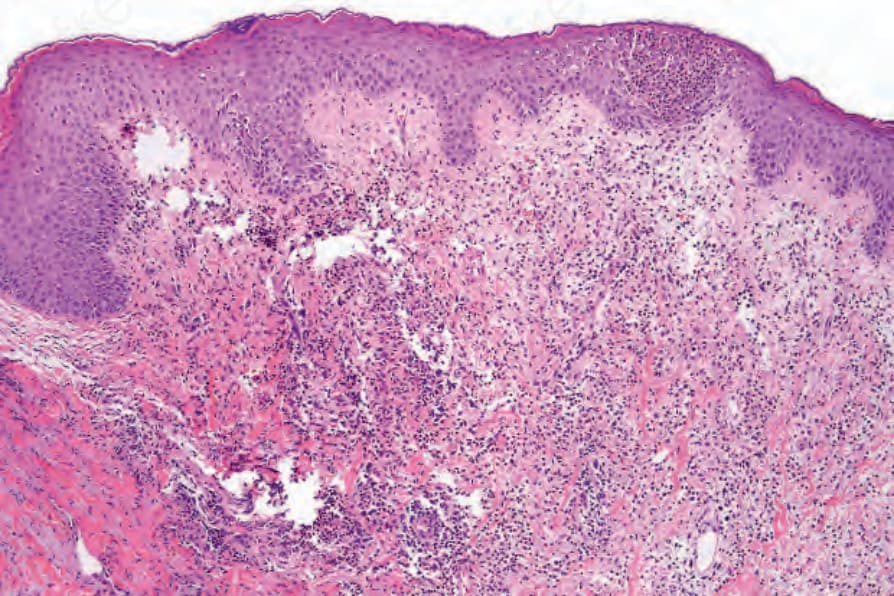
Fig. 14.69 Acute generalized exanthematous pustulosis: there is a subcorneal pustule. The dermis is intensely inflamed.

Fig. 14.71 Drug-induced pseudolymphoma: this patient developed a maculopapular eruption following treatment with phenytoin.
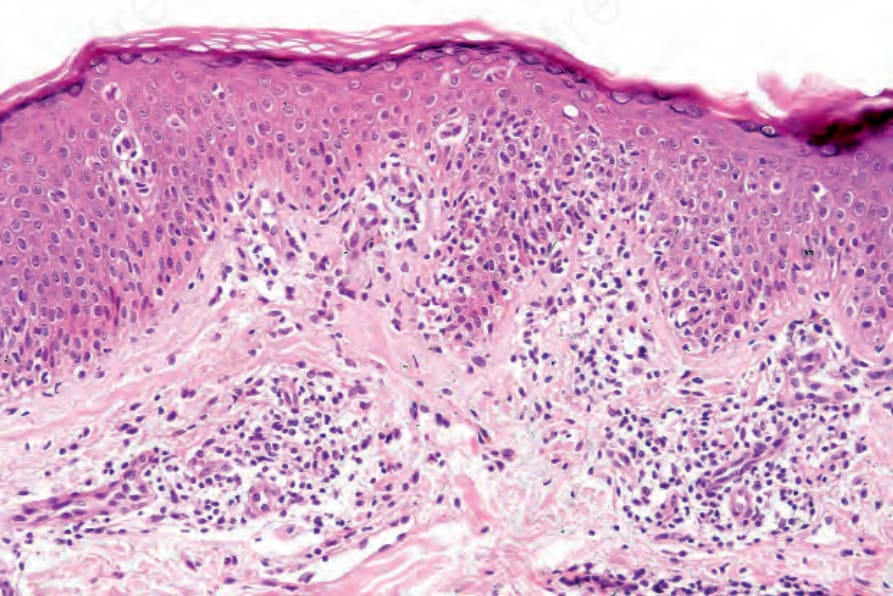
Fig. 14.72 Drug-induced pseudolymphoma: there is an atypical superficial perivascular lymphocytic infiltrate. Note the marked epidermotropism. The histological features are suggestive of mycosis fungoides.
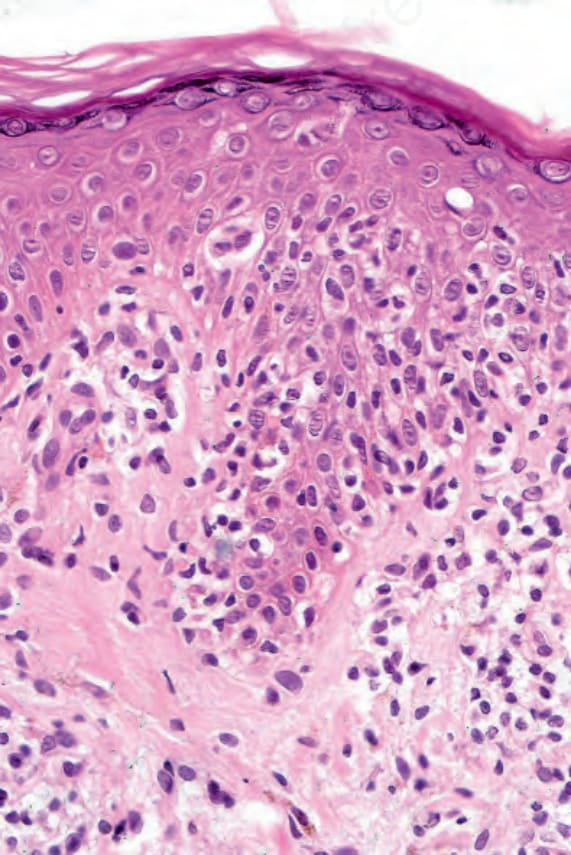
Fig. 14.73 Drug-induced pseudolymphoma: the lymphocytes are surrounded by a welldeveloped retraction artifact and there is a small Pautrier microabscess.
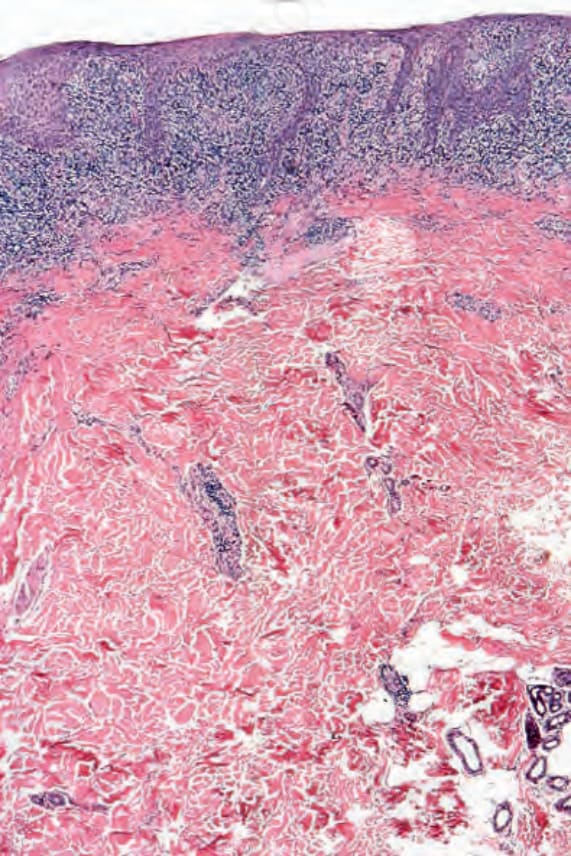
Fig. 14.74 Carbamazepine-induced pseudolymphoma: in this example, there is a dense bandlike upper dermal lymphocytic infiltrate.
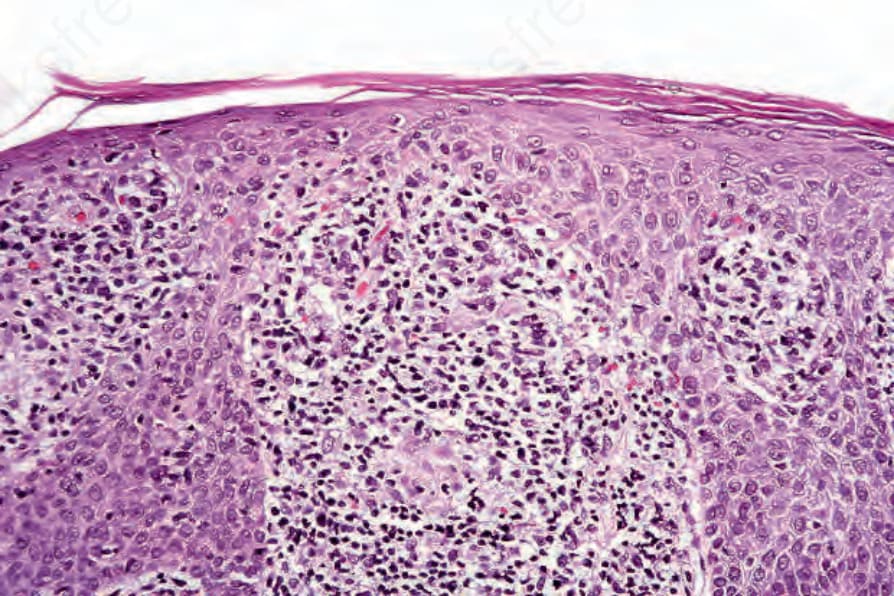
Fig. 14.75 Carbamazepine-induced pseudolymphoma: there is marked lymphocytic atypia. Cerebriform cells are present. The features are very suggestive of plaque stage mycosis fungoides.
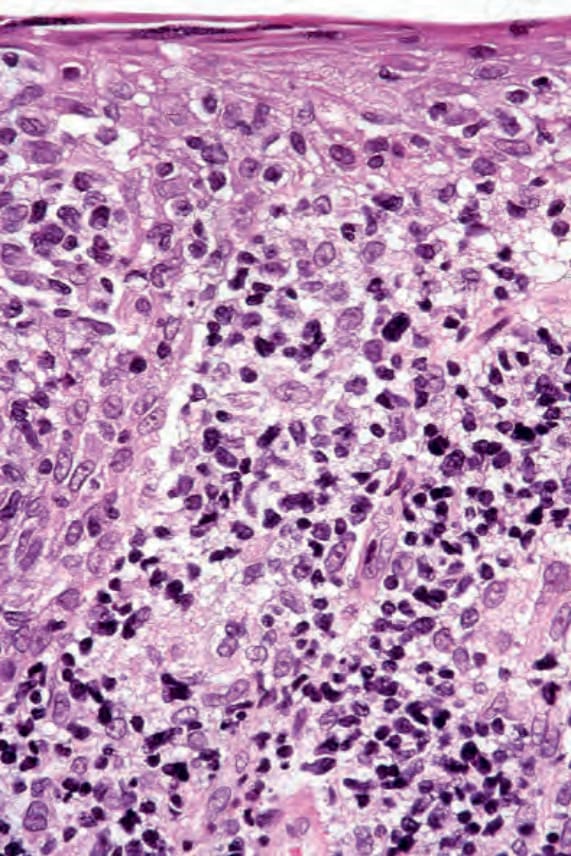
Fig. 14.76 Carbamazepine-induced pseudolymphoma: diagnosis depends on careful clinicopathological correlation.
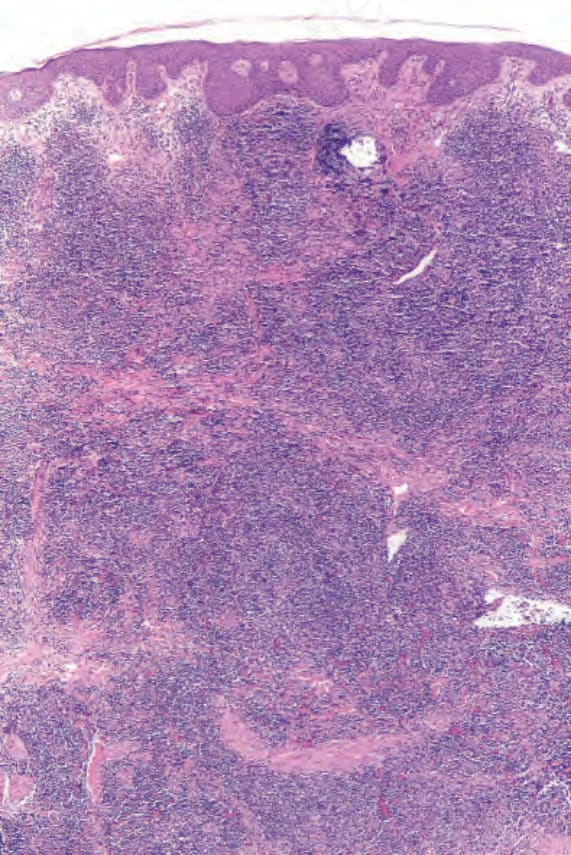
Fig. 14.77 Drug-induced pseudolymphoma: this very dense dermal infiltrate developed following treatment with an antidepressant. Multiple cutaneous nodules were present.
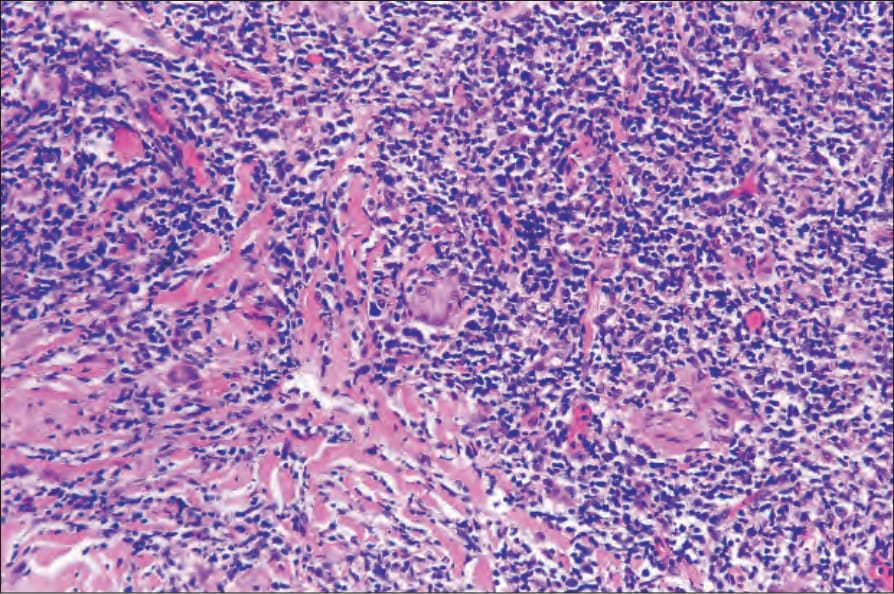
Fig. 14.78 Drug-induced pseudolymphoma: scattered multinucleated giant cells are evident.
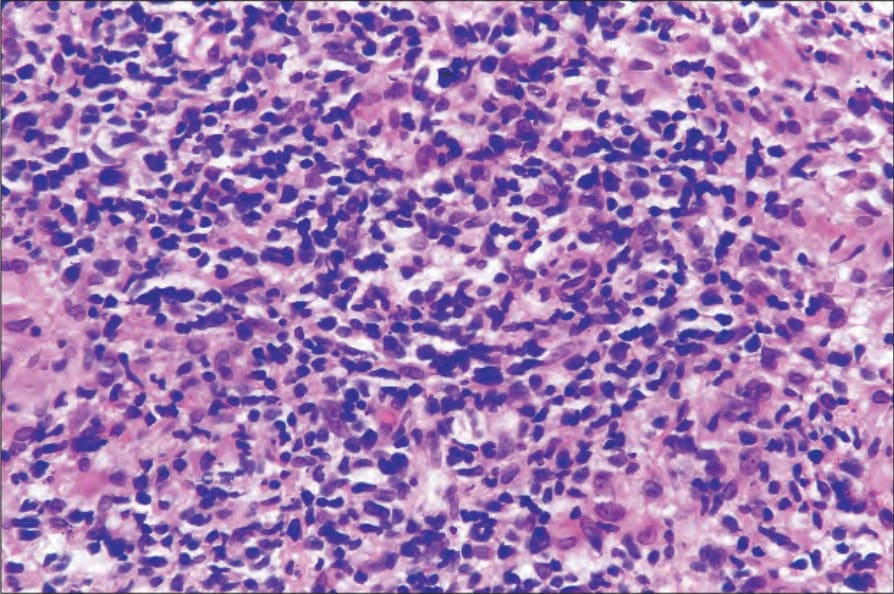
Fig. 14.79 Drug-induced pseudolymphoma: there is marked lymphocytic atypia. The nodules melted away following withdrawal of drug.