Drug-induced hyperpigmentation
Drug-induced hyperpigmentation
Clinical features Cutaneous hyperpigmentation is a frequent complication of drug therapy. It may result from increased melanin synthesis or deposition of the drug or its metabolite within the skin.1–5 Heavy metals can also result in skin
pigmentation.4 Most often, however, it results from postinflammatory hyperpigmentation.3
Long-term treatment with minocycline might result in usually reversible (types I and II) cutaneous pigmentation.6–13 Three clinical variants of cutaneous minocycline pigmentation are generally recognized (Figs 14.34–14.36):
• Type I: blue-black macules localized to areas of scarring and inflammation (e.g., facial acne scars),
• Type II (most common): blue-black, brown or slate-gray pigmentation on the shins, ankles, and arms,
• Type III: generalized muddy-brown pigmentation which may be exacerbated on sunlight-exposed regions. A fourth variant affecting the lips and possibly representing a fixed drug eruption has been described.14
646 Cutaneous adverse reactions to drugs
Minocycline may involve the teeth (causing a green-gray or blue-gray discoloration), predominantly affecting the middle and occasionally the incisal thirds of the crown.18 Lesions of the oral mucosa are rare although pigmentation has been described on the buccal mucosa, gingiva, tongue, and lips.19–23 The bones underlying the oral cavity (black bone disease) represent the single site most commonly affected by minocycline pigmentation.24 This is best visualized by inspecting the maxillary and mandibular anterior alveolar mucosa.14 The hard palate and lingual alveolar bone are also commonly affected.14
The conjunctiva, sclera, thyroid (black thyroid), aorta, endocardium, and atherosclerotic plaques may also be involved in minocycline pigmentation.25–34 Minocycline pigmentation may also affect the vulvar/ vaginal mucosa and may clinically mimic a melanocytic lesion.35
Many other tetracyclines including methacycline and tetracycline hydrochloride have also been associated with cutaneous pigmentation.36,37
Amiodarone, which is used primarily in the treatment of cardiac arrhythmias, is associated with a phototoxic/photosensitivity reaction in up to 50% of patients.38–44 In addition, cutaneous golden-brown to slate-gray or blue/violaceous pigmentation predominantly affecting the exposed surfaces including the face and the backs of the hands may develop, especially in those receiving high doses over a protracted period of time (Fig. 14.37).38 Pigmentation is also sometimes seen in the sclera and cornea.41
Antimalarials also result in abnormal skin pigmentation.45–48 Mepacrine (quinacrine) typically produces a yellow coloration although localized blue-black mucocutaneous lesions have been described (Figs 14.38 and 14.39).48 Chloroquine and hydroxychloroquine cause yellow-brown to gray pigmentation.2,45–47 Sun-exposed skin is predominantly affected, although mucosal pigmentation may also occur.49
Localized minocycline pigmentation as a complication of cosmetic laser procedures have also been reported.15,16
Nail pigmentation most often presents as a persistent slate-gray coloration of the proximal nail bed.17 Additional features include longitudinal melanonychia, diffuse nail pigmentation, and photo-onycholysis.17
In addition to causing photosensitivity and contact dermatitis, chlorpromazine therapy (particularly when protracted and in high doses) can result in cutaneous pigmentation, especially on sun-exposed skin such as the face, dorsum of the hands, and the neck.2,50–53 Patients may present with a golden brown, tanned appearance while others develop a slate-gray, bluish, or purple appearance. The cornea and lens of the eye can also be involved.2
Long-term treatment with imipramine may result in photodistributed hyperpigmentation affecting the face, neck, ‘V’ of chest, arms, and hands (Fig. 14.40).54–56 The coloration varies from golden brown to blue-gray or slate-gray. The irises may also darken.
Photodistributed blue-gray pigmentation has been documented following treatment with desipramine.57
Heavy metals including gold, silver, and mercury can all result in cutaneous pigmentation (see below).
647 Drug-induced hyperpigmentation
Pathogenesis and histologic features The histologic features of minocycline pigmentation are variable.7,10,11,14 In types I and II variants, golden brown to brown-black granules are found predominantly within macrophages distributed mainly around the vasculature and sweat gland coils (Fig. 14.41). The pigment, which fluoresces yellow under ultraviolet light, stains positively with both Masson-Fontana and Perls Prussian blue reactions in type II variants (Figs 14.42 and 14.43).11 The pigment is periodic acid-Schiff (PAS) negative. In contrast, in type I, the pigment only stains with Perls reaction. It is believed to represent minocycline or its breakdown product chelated with hemosiderin, ferritin, or iron.7 Calcium, sulfur, and chlorine are also present, but melanin is absent.11 Melanocytes and the epidermis show no increase in melanin pigmentation in types I and II variants. Type III hyperpigmentation is characterized by
648 Cutaneous adverse reactions to drugs
an increase in epidermal basal cell melanin pigmentation.6 The Perls stain is negative. Minocycline pigmentation of the subcutaneous fat has been described in the clinical setting of type II disease.58,59 Histologically, there is pigment within macrophages and giant cells in the subcutaneous fat, with positive staining for Masson-Fontana and variable staining with Perls reaction. One study also described green-gray nonrefractile globules within macrophages in the fat.59
These granules are nonrefractile and stain positively with Masson-Fontana and are negative for iron.60
Histologically, chlorpromazine hyperpigmentation is characterized by golden brown macrophage-bound granules surrounding the superficial vasculature. The granules are positive with the Masson-Fontana reaction but do not stain with Perls Prussian blue.53 Ultrastructurally, the pigment is lysosome bound and present in endothelial cells, fibroblasts, Schwann, and smooth muscle cells, in addition to macrophages.50,51 Increased melanin also contributes to the cutaneous pigmentation.50
Histologically, amiodarone pigmentation is characterized by macrophages containing PAS-positive, yellow-brown lipofuscin-like granules located in a perivascular distribution (Figs 14.44 and 14.45).38 Melanin pigmentation of the epidermis is not increased; indeed, its absence in involved skin has recently been documented.44 By electron microscopy, the granules are located within lysosomes.39,43 Lamellar myelin bodies may also be identified.25 Similar inclusions may be found in the hepatocytes, Kupffer cells, pulmonary macrophages, and neutrophils.
In mepacrine (quinacrine) pigmentation, yellow-brown pigment is found within the cytoplasm of histiocytes throughout the dermis.48 The pigment is weakly positive with the Perls Prussian blue reaction for iron and is Masson-Fontana negative.44,49 The histologic findings in hydroxychloroquine-related pigmentation have been described as yellow-brown granular deposits within macrophages and extracellularly.60
Histologically, imipramine and desipramine hyperpigmentation contain Masson-Fontana positive golden brown granules within the upper dermis, lying both free and within macrophages (Fig. 14.46).54,55,57 Perls Prussian blue is negative. Ultrastructurally, histiocytes contain melanosomes in addition to lysosomal-bound electron-dense granules.54
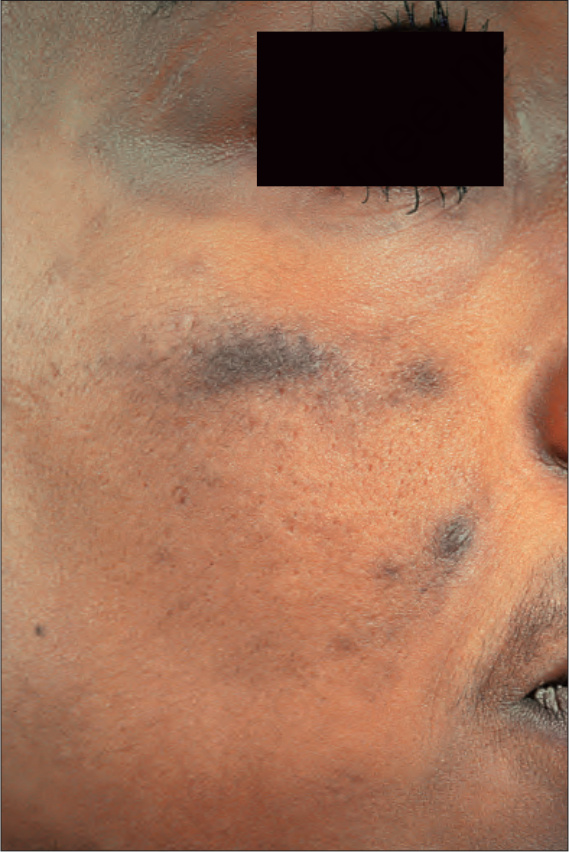
Fig. 14.34 Minocycline pigmentation: extensive lesions involving the cheek and periorbital region. By courtesy of the Institute of Dermatology, London, UK.

Fig. 14.35 Minocycline pigmentation: these blue-black lesions have developed in a patient with pyoderma gangrenosum. By courtesy of the Institute of Dermatology, London, UK.
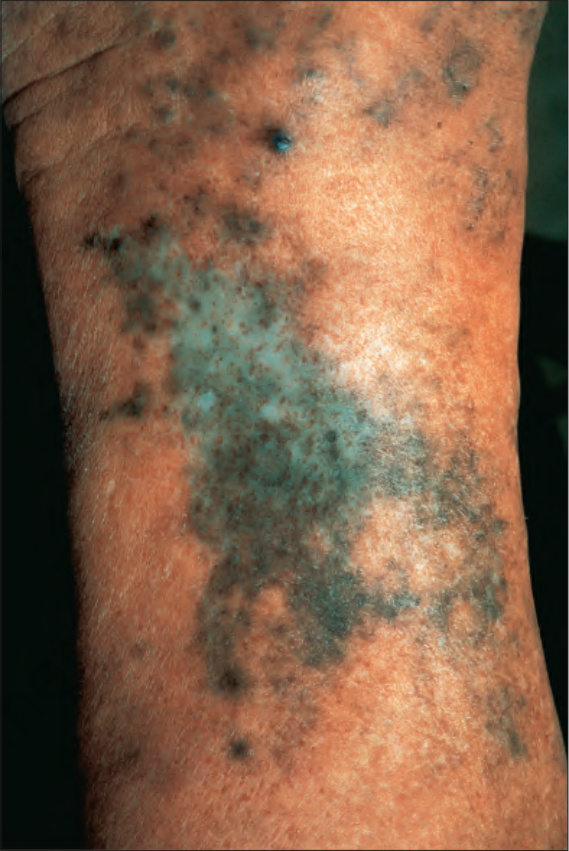
Fig. 14.36 Minocycline pigmentation; typical pigmentation affecting the shin. By courtesy of the Institute of Dermatology, London, UK.
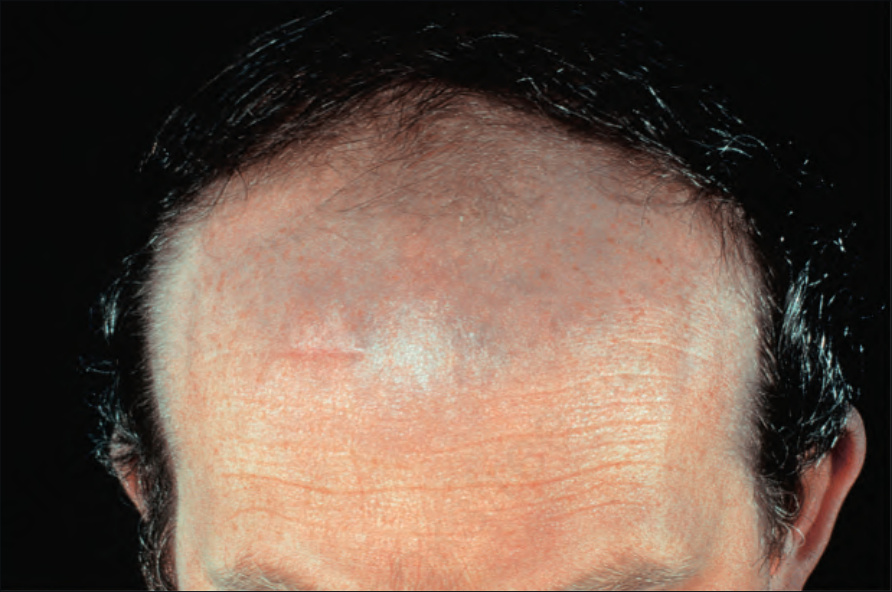
Fig. 14.37 Amiodarone pigmentation: note the slate-gray discoloration on the forehead, a characteristic site. By courtesy of the Institute of Dermatology, London, UK.

Fig. 14.38 Mepacrine pigmentation: a yellow discoloration is characteristic. By courtesy of the Institute of Dermatology, London, UK.
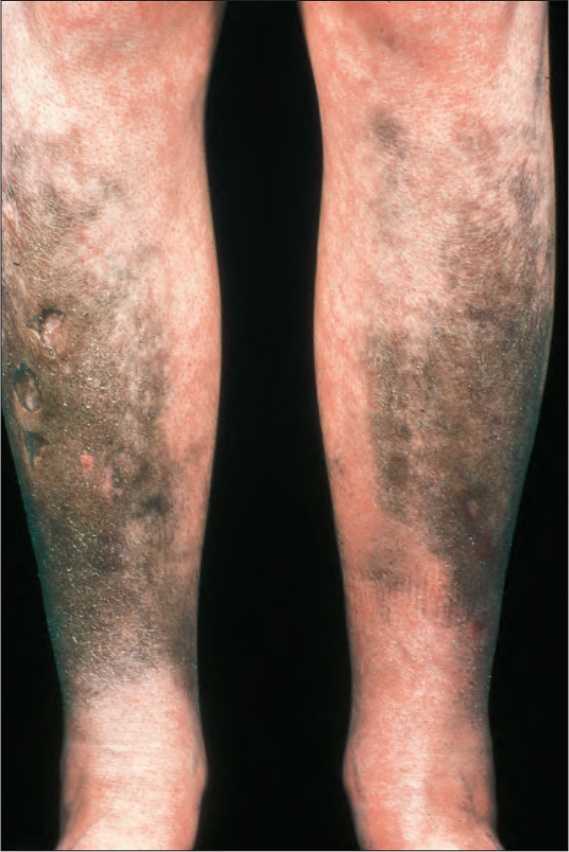
Fig. 14.39 Mepacrine pigmentation: in this patient, the drug resulted in black lesions. By courtesy of the Institute of Dermatology, London, UK.

Fig. 14.40 Imipramine pigmentation: note the intense brown pigment of the hands and forearms in comparison with the chest. By courtesy of L. Cohen, MD, Cohen Dermatopathology, Massachusetts, USA.
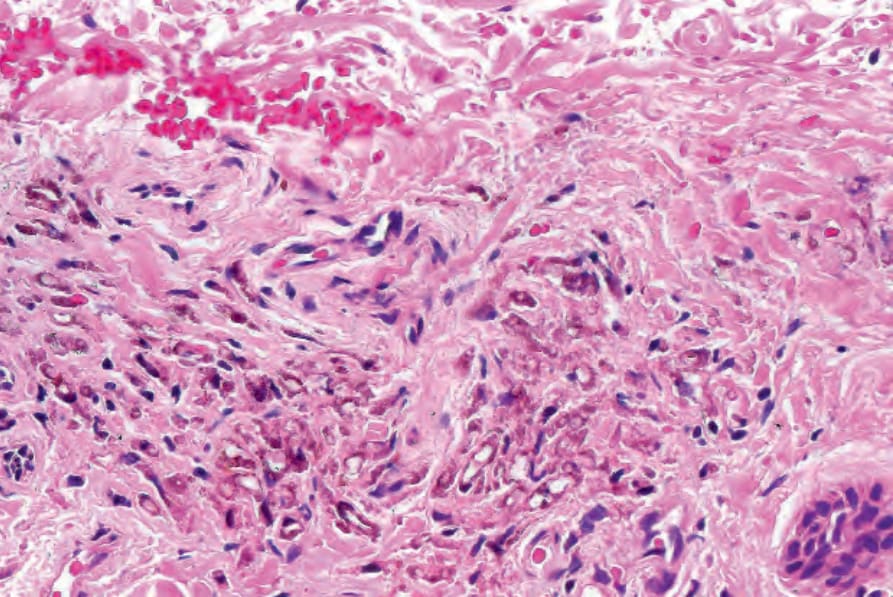
Fig. 14.41 Minocycline pigmentation: note the presence of perivascular granular brown pigment.
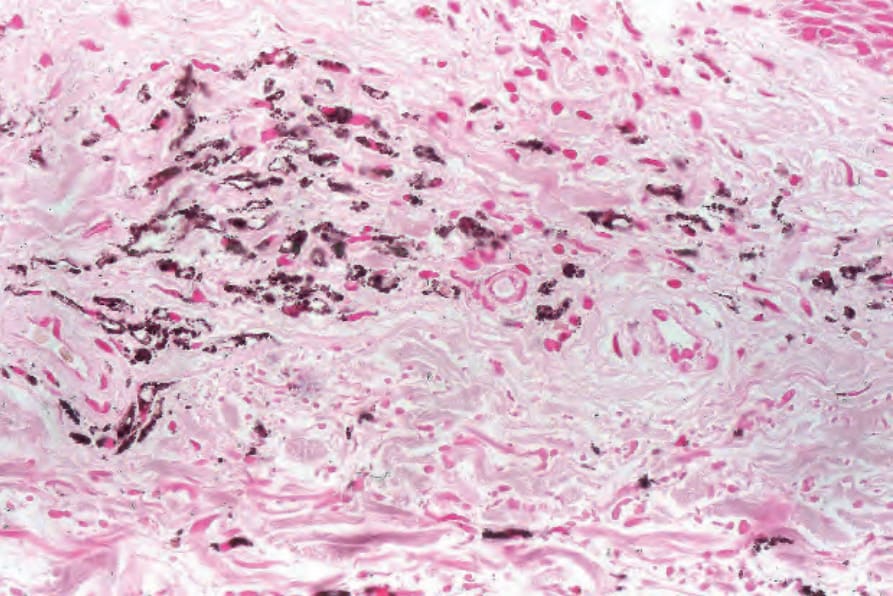
Fig. 14.42 Minocycline pigmentation: the pigment stains positively with Masson-Fontana.
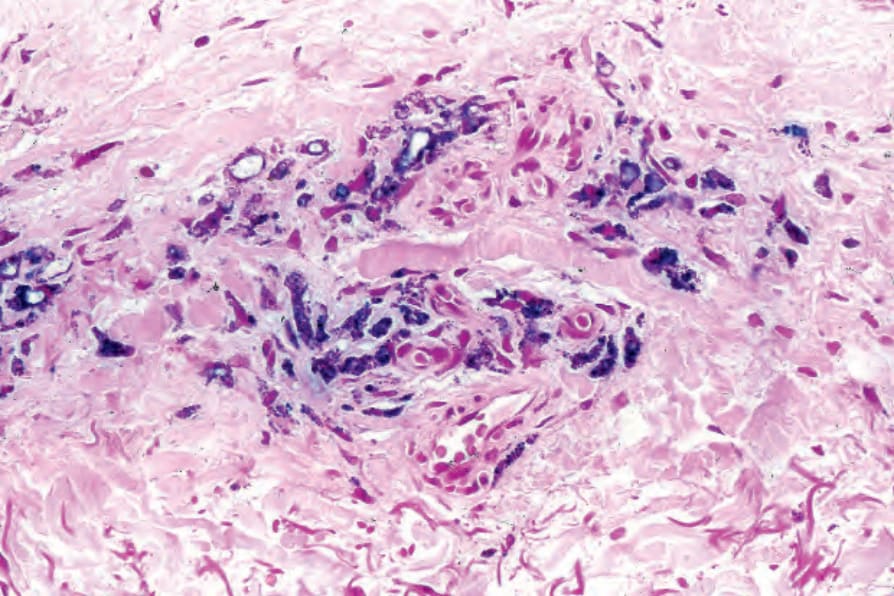
Fig. 14.43 Minocycline pigmentation: the pigment also stains with Prussian blue.
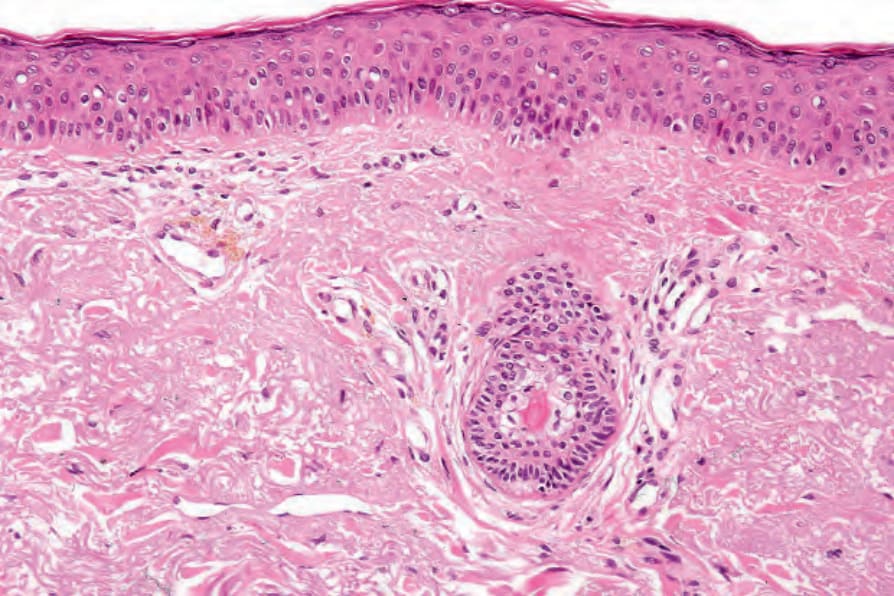
Fig. 14.44 Amiodarone pigmentation: pigmented macrophages are present in a perivascular distribution.
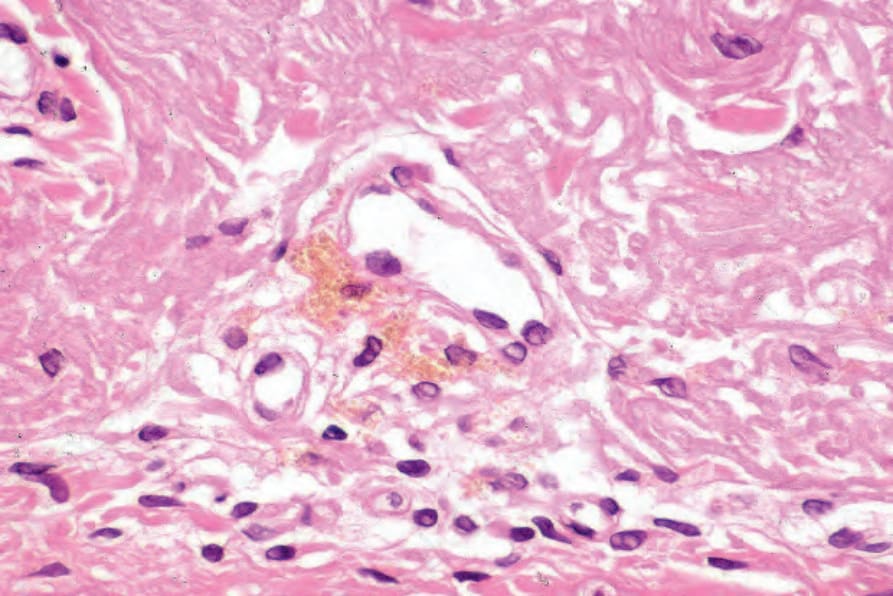
Fig. 14.45 Amiodarone pigmentation: high-power view.
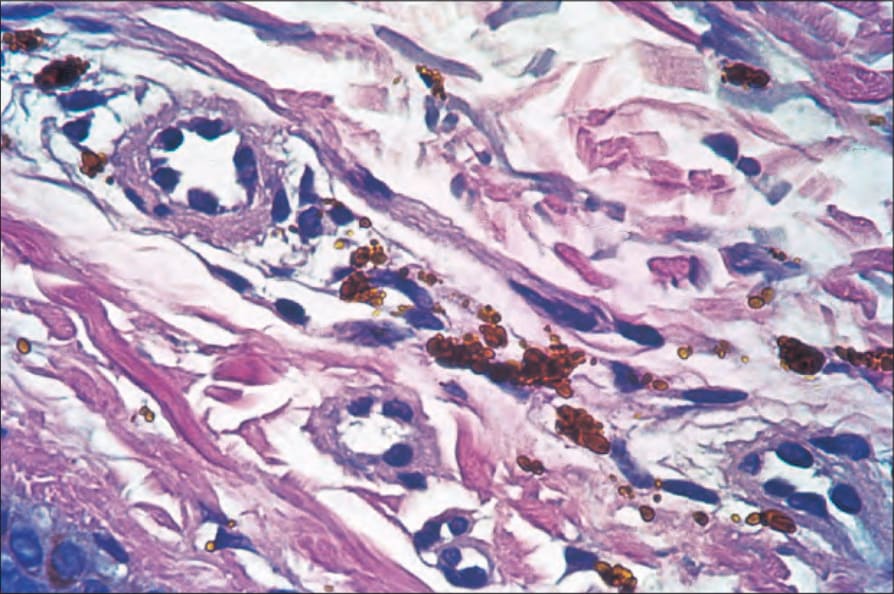
Fig. 14.46 Imipramine pigmentation: typical golden-brown granules. Note that the Prussian blue reaction is negative. By courtesy of L. Cohen, MD, Cohen Dermatopathology, Massachusetts, USA.