Acrodermatitis enteropathica
Acrodermatitis enteropathica
Clinical features Acrodermatitis enteropathica is a rare autosomal recessive inherited disorder of zinc malabsorption, which predominantly affects infants and responds dramatically to dietary zinc supplements.1–4 It presents with diarrhea, stomatitis, irritability, and failure to thrive, accompanied by erythematous scaly and crusted lesions with vesicles, pustules, and erosions, predominantly affecting the extremities, perineal, and periorificial region (Figs 13.199 and 13.200). Frankly bullous lesions have been described.5 Nonscarring alopecia may also be present. Additional features include nail dystrophy, prolonged wound healing, impetiginization, short stature, psychiatric symptoms, and photophobia.1–7 Corneal lesions and decreased visual acuity have also exceptionally been reported.8,9 Patients are also prone to developing infections, particularly by bacteria and fungi, illustrating the importance of
629 Acrodermatitis enteropathica
The changes are due not only to zinc deficiency, but also to a deficiency in branched chain amino acids including isoleucine.63,64 This is induced by the low protein diet that these patients receive. Acrodermatitis enteropathica has also been described in relation to HIV infection.65
Pathogenesis and histologic features The manifestations of acrodermatitis enteropathica result from insufficient absorption of zinc by the intestine. The mechanism of the disease involves a defect in a zinc transporting protein. Initial studies of genes that encode for proteins important in the transport of zinc including SLC30A4 and ZNT4 did not show association with the disease.66–68 More recently, the gene for acrodermatitis enteropathica has been identified on chromosome 8q24.3.69 This gene, designated SLC39A4, encodes a histidine-rich transmembrane protein known as hZIP4 which is involved in zinc uptake.70–76 The mutation in acrodermatitis enteropathica also affects zinc metabolism in fibroblasts and reduces the activity of 5′-nucleotidase.78,79 Over 30 different mutations in this gene have been described thus far in association with acrodermatitis enteropathica.75–77,80–84 The vast majority of patients carry a homozygous or compound heterozygous mutation in SLC39A4. However, there are some without such an identifiable genetic mutation, indicating that other genetic factors may possibly play a causative role in the disease.75
normal zinc levels in maintaining the integrity of the immune system.10–13 The disease can persist into adulthood or rarely be diagnosed for the first time in adult life.14–16 An acquired variant may complicate artificially fed or, rarely, breast-fed infants either full term or premature.17–28 This is due to the low concentration of zinc in breast milk secondary to a defect in zinc uptake from maternal serum into the breast.28 In premature infants, the problem is aggravated by the low gastrointestinal absorption of zinc and low body stores of zinc that were transferred from mother to fetus in the last 10 weeks of pregnancy.28,29
Many other conditions with acquired zinc deficiency have been associated with signs and symptoms of acrodermatitis enteropathica including Crohn disease, alcoholic cirrhosis, alcoholic pancreatitis, intestinal bypass operation, chemotherapy for hematological malignancies, anorexia nervosa, lymphoma, biotin deficiency, dialysis, cystic fibrosis, Hartnup disease, essential fatty acid deficiency, citrullinemia, deficiency of ornithine transcarbamylase, following total intravenous hyperalimentation, and celiac disease.9,30–55 A similar picture has also been described in a number of aminoacidopathies and organic acidemias. The latter include methylmalonic acidemia, propionic acidemia, glutaric aciduria type I, and nonketotic hyperglycinemia.56–62
The mechanism of infections in acrodermatitis enteropathica is related to alterations in the immune system due to zinc deficiency.12,13 Zinc is critical to the development and function of lymphocytes, neutrophils, macrophages, NK cells, and cytokine production. It also functions as an antioxidant and prevents cellular damage by free radicals.13 Lymphopenia and thymic atrophy are frequent findings in acrodermatitis enteropathica and are due to the loss of B- and T-cell precursors in the bone marrow. The zinc deficiency induces apoptosis mediated by glucocorticoids with resultant decrease in lymphopoiesis.
The histopathology varies according to the stage of evolution.85 Very early lesions show subtle changes consisting of focal parakeratosis alternating with orthokeratosis. As lesions advance, the parakeratosis becomes more prominent and confluent and the stratum granulosum is decreased or absent. The keratinocytes in the upper layers of the epidermis display marked cytoplasmic pallor (Figs 13.201 and 13.202). In addition there is focal spongiosis. Dyskeratotic cells are rarely seen.
630 Degenerative and metabolic diseases
In late stages there is cytoplasmic vacuolation and necrosis which may result in intraepidermal vesicles or occasionally progress to blister formation.86,87 Subcorneal pustules may be seen and usually indicate secondary infection. An atypical case of bullous acrodermatitis enteropathica with a lichenoid infiltrate has been reported.88
buttocks, and distal limbs (Fig. 13.203).3 Patients most often present in their sixth decade (median 52 years) with intense erythema, which progresses to flaccid bullae that rupture readily and develop crusting.11,15 A rare pediatric case has been described.16 Pressure, friction, and trauma have occasionally been noted to precipitate the eruption.8 Central healing with active borders gives rise to annular and serpiginous lesions. Lesions are often painful and pruritic.
Postinflammatory hyperpigmentation follows resolution. Individual lesions usually last 1–2 weeks and, characteristically, lesions in varying stages of evolution are evident at any one time.8,15
Additional features may include stomatitis, angular cheilitis, blepharitis, conjunctivitis, hair loss, and nail changes.9–11 Laboratory investigations commonly reveal an abnormal glucose tolerance test, normochromic normocytic anemia, hypoproteinemia, hypoalbuminemia, and hypoaminoacidemia.9,17 Low amino acid levels were detected in 96% of patients in one reported series.18 However, in larger series, the percentage of patients with low amino acid levels has been lower, ranging between 41% and 78%.10,11 Patients with low amino acid levels may respond to intravenous replacement.19
Differential diagnosis Histologically, acrodermatitis enteropathica is indistinguishable from necrolytic migratory erythema and pellagra. Very similar histologic features are also seen in necrolytic acral erythema, a condition that occurs on the dorsum of the feet and legs of patients with hepatitis C infection.89–91 Lesions are erythematous and psoriasiform plaques and decreased serum and lesional zinc levels have been associated with this condition.91,92 Prominent pallor of keratinocytes in the upper layers of the epidermis is also seen in deficiency of the M subunit of lactate dehydrogenase.93,94 The cutaneous manifestation of the latter condition has been described as annually recurring acroerythema.95

Fig. 13.199 Acrodermatitis enteropathica: extensive crusted erosions in a characteristic distribution. By courtesy of Z.S. Tannous, MD, Harvard Medical School, Boston, USA.

Fig. 13.200 Acrodermatitis enteropathica: in this infant, there is very extensive involvement with widespread erosion. By courtesy of Z.S. Tannous, MD, Harvard Medical School, Boston, USA.
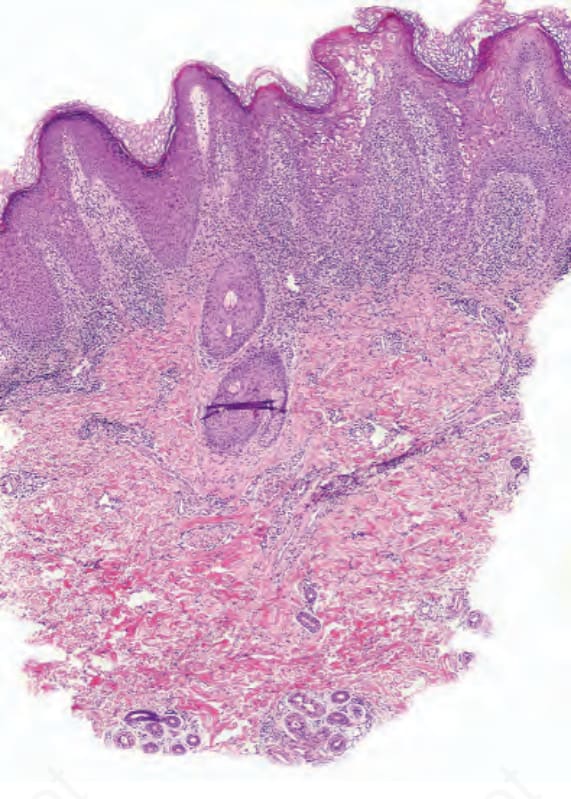
Fig. 13.201 Acrodermatitis enteropathica: low-power view showing hyperkeratosis and marked epidermal eosinophilia on the right side.
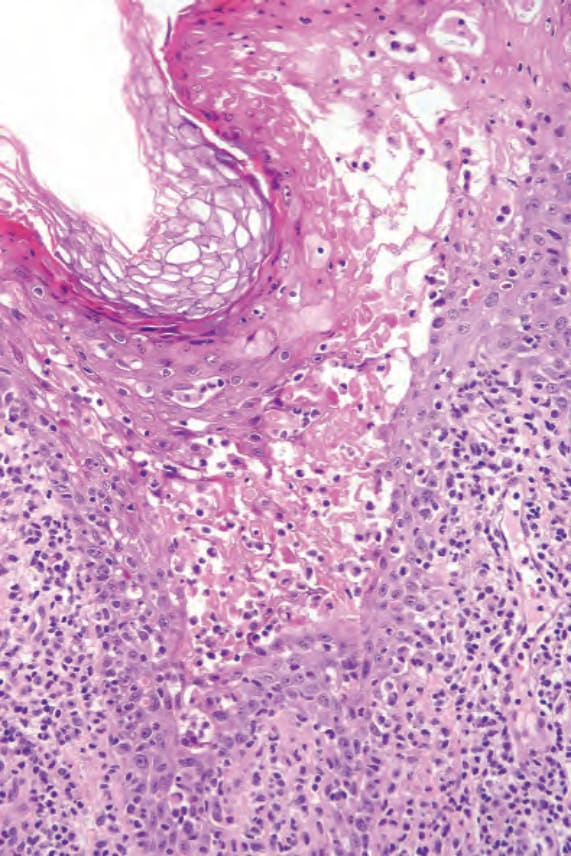
Fig. 13.202 Acrodermatitis enteropathica: keratinocyte necrosis is seen in this high-power view.

Fig. 13.203 Necrolytic migratory erythema: note the intense erythema in a characteristic distribution. By courtesy of the Institute of Dermatology, London, UK.