Acanthosis nigricans
Acanthosis nigricans
Clinical features Acanthosis nigricans develops under a variety of circumstances.1–3 In addition to the well-recognized tumor-associated variant, acanthosis nigricans may present with benign familial forms, endocrinopathy and drug-related variants, and the condition can be seen in association with a range of congenital conditions including lipoatrophy, leprechaunism, and the type A and type B syndromes described below. Genetic conditions associated with acanthosis nigricans include:
• Alstrom syndrome (retinopathy, progressive sensorineural hearing loss, and truncal obesity),
• Crouzon syndrome (facial palsy, sensorineural hearing loss with skeletal and mental retardation),
• Seip-Lawrence syndrome (congenital lipodystrophic diabetes),
• Costello syndrome (postnatal growth deficiency, coarse facies, redundant skin of the neck, palms, soles, and fingers, dark skin, and papillomas),
• Bannayan-Riley-Ruvalcaba syndrome (subcutaneous lipomas, vascular malformations, lentigines of the penis and vulva, warty lesions, macrocephaly, mental retardation, intestinal polyposis, skeletal abnormalities, vascular malformations of the central nervous system, and thyroid tumors),4–8
• Lelis syndrome (ectodermal dysplasia with hypotrichosis, hypohidrosis, hypodontia, palmoplantar hyperkeratosis, and perioral furrows).9
for S100 protein and CD1a. The dermal mucin can be highlighted with Alcian blue at pH 2.5 or toluidine blue cytochemical stains.1,8,10
Ultrastructural examination reveals intracellular structures reminiscent of lysosomal storage diseases. Within the cytoplasm of the histiocytes, there are circular osmophilic myelin bodies and zebra bodies.1–11
Differential diagnosis Clinically the differential diagnosis includes generalized eruptive histiocytoma, xanthoma disseminatum, and progressive nodular histiocytosis. None of these entities is associated with increased dermal mucin. Histologically, the differential diagnosis includes acral persistent mucinosis, focal dermal mucinosis, superficial angiomyxoma, scleromyxedema, granuloma annulare and myxoid dermatofibroma. Acral persistent mucinosis is not familial and lacks a histiocytic proliferation. Focal dermal mucinosis and superficial angiomyxoma are typically solitary lesions and do not have a histiocytic
Acanthosis nigricans has been described in association with a missense mutation of the fibroblast growth factor receptor.4 This disease is also associated with severe neurological impairment and severe achondroplasia.10 Additional rare associations include Wilson disease (hepatolenticular degeneration) and primary biliary cirrhosis.11,12 In the latter case, the acanthosis nigricans resolved after liver transplantation. In an exceptional family with several members affected by acanthosis nigricans, absence of the eyebrows and eyelashes and sparse hair elsewhere has been reported.13
Development of acanthosis nigricans may also antedate or present concomitantly with a variety of connective tissue diseases including systemic lupus erythematosus, systemic sclerosis, and dermatomyositis.14–17 The condition is characterized by the presence of symmetrical brown velvety or verrucous plaques with a predilection for intertriginous sites, such as the back
627 Acanthosis nigricans
epidermal ridges and deep sulci giving the skin a velvety rugose texture.22 Tripe palms are frequently associated with a variety of internal malignancies and often (but not invariably) accompany acanthosis nigricans.23–29 However, the lesion may also represent a benign reversible phenomenon unassociated with neoplasia. Less frequently, there are similar changes on mucosal surfaces, such as the mouth (particularly the tongue and upper lip) or genitalia (Fig. 13.197).30,31 The latter changes are more common in cases related to malignancy.
of the neck, groin, and axillae (Figs 13.194 and 13.195). In more extreme forms the changes may be generalized.18 Involvement of the eyelids also rarely occurs.19–21 In addition, there is sometimes brown thickening of the skin over the dorsum of the fingers or, rarely, the palms of the hands (tripe palms) (Fig. 13.196). The latter is a distinctive appearance due to broadened
Oral lesions have been reported in 25% to 50% of all cases of acanthosis nigricans and this presentation is a marker for potential underlying malignancy.29,30,32–34 At least 35% of patients with oral acanthosis nigricans have an associated malignancy.30,32,35 The tongue lesions consist of hypertrophied filiform papillae producing a deeply fissured papillomatous surface and the lips develop papillary and verrucous lesions.30 The palate and buccal mucosa may also be involved.35 Oral lesions are usually nonpigmented. Involvement of the esophagus is rare and is almost invariably associated with malignancy, particularly in the gastrointestinal tract.36
A drug-induced variant has been documented, and glucocorticoids, nicotinic acid, oral contraceptives, and diethylstilbestrol have been implicated.37 Acanthosis nigricans has also been reported in association with
628 Degenerative and metabolic diseases
somatotrophin therapy.38 It has also been seen as a complication of testosterone injections and at insulin injection sites.39,40
Rarely, the disease presents as an autosomal dominant nevoid lesion, which may present at birth, in childhood, or at puberty.41,42 The condition has also been reported in association with Cohen syndrome (truncal obesity, hypotonia, mental retardation, microcephaly, and ocular abnormalities).43
So-called benign familial acanthosis nigricans occurs more commonly in females. This autosomal dominantly inherited condition usually presents in early childhood with lesions that particularly affect the face, dorsal surfaces of the fingers, and the flexures.44 There are usually no associated endocrinopathies or congenital abnormalities.
Acanthosis nigricans presents in up to 51% of patients with Down syndrome and is probably due to insulin resistance.45 It has also been described in up to 5% of patients with severe atopic dermatitis, but the pathogenesis in this setting is unknown.45
It may occur in the setting of malignancy, as discussed above, and may be the presenting sign of occult neoplasms. The sex incidence is equal. Malignant acanthosis nigricans is often severe, widely disseminated, and has a rapid course. Lesions may also be pruritic and are more difficult to treat. Tumors that are particularly associated include gastric adenocarcinoma and, less often, malignancies of the extrahepatic biliary tree, breast, pancreas, bladder, and colon.23,25,27,29,34,36,46,47 Ovarian and uterine tumors, bronchial squamous and adenocarcinoma, and lymphoma have also been implicated.26,33,48
Acanthosis nigricans as an indicator of insulin resistance has been reported in HIV-positive patients receiving treatment with protease inhibitors.49
The malignant form sometimes develops in association with other cutaneous markers of internal malignancy, including palmoplantar hyperkeratosis, eruptive seborrheic keratoses (Leser-Trélat sign), and florid cutaneous papillomatosis.26,50 The last condition presents as numerous viral wartlike itchy papillomata, which show a predilection for the trunk and extremities and invariably accompany an internal malignancy, most often gastric adenocarcinoma. The course of malignant acanthosis nigricans usually parallels that of the underlying neoplasm, which is generally aggressive and associated with a high mortality. Lesions may sometimes abate following surgical removal of the tumor, only to return with its recurrence.
Acanthosis nigricans is also associated with a wide range of endocrine diseases, including Cushing disease, acromegaly, gigantism, Addison disease, polycystic ovary syndrome, diabetes mellitus, and thyroid disorders. The association between hyperandrogenism (HA), insulin resistance (IR), and acanthosis nigricans (AN) is known as HAIR-AN syndrome. There appears to be an association between acanthosis nigricans, obesity, hypertension, ischemic heart disease, and type 2 diabetes, the inheritance of which is autosomal dominant.51 Acanthosis nigricans may also occur in nonobese patients in association with diabetes mellitus and insulin resistance due to diminished receptor binding.52–57 Patients with this sporadic syndrome are divided into two groups:
• In type A, the patients are young (particularly black) women with acanthosis nigricans, primary amenorrhea with hypertestosteronemia, virilization, increased somatic growth, hyperglycemia and hyperinsulinemia, with insulin resistance due to a congenital defect of insulin receptors.
• In type B, the patients are older and have features suggesting other autoimmune diseases, including raised erythrocyte sedimentation rate (ESR), proteinuria, and hypocomplementemia with antinuclear and anti-DNA antibodies. Antibodies directed against the insulin receptor may be detected.
• A third type, type C, has recently been proposed, in which acanthosis nigricans and insulin resistance are associated with a postinsulin receptor defect. Studies have found that the presence of acanthosis nigricans in African-Americans and Native Americans is a cutaneous marker of hyperinsulinemia and insulin resistance.58,59
Transient acanthosis nigricans-like lesions have been described at the sites of healing lesions of pemphigus vulgaris and pemphigus foliaceous.64,65
Acanthosis nigricans-like lesions have been described after local application of fusidic acid.66
Pathogenesis and histologic features The pathogenesis is uncertain, although in the diabetes-associated patients hyperinsulinemia is likely to be of importance.55 In malignancy-related acanthosis nigricans, peptide or hormonal secretion appears to be of significance in at least a proportion of cases.46 It has been demonstrated that some malignant tumors secrete transforming growth factor alpha (TGF-α) in large quantities and this stimulates proliferation of keratinocytes.67
The histopathological findings are subtle, comprising delicate, elongate papillomatosis, hyperkeratosis and slight acanthosis, sometimes alternating with foci of atrophy (Fig. 13.198). The occasional presence of keratin-filled cysts may result in a seborrheic keratosis-like appearance.30 Despite the clinically obvious brown appearance of the lesions, there is normally little increase in the amount of melanin present. A non-specific perivascular chronic inflammatory cell infiltrate is sometimes evident in the superficial dermis. Distinguishing this type of benign acanthosis from others, such as epidermal nevi may be difficult.
Oral lesions show hyperkeratosis and patchy parakeratosis associated with marked acanthosis and epithelial papillary hyperplasia.30
Tripe palms are characterized by hyperkeratosis, acanthosis, and papillary dermal hypertrophy.22
Florid cutaneous papillomatosis is also characterized by hyperkeratosis, papillomatosis, and acanthosis.50
Obesity-associated acanthosis nigricans, previously called pseudoacanthosis nigricans, develops in the flexures of obese patients. This is the most common type of acanthosis nigricans in children and adults and is associated with insulin resistance.60–63
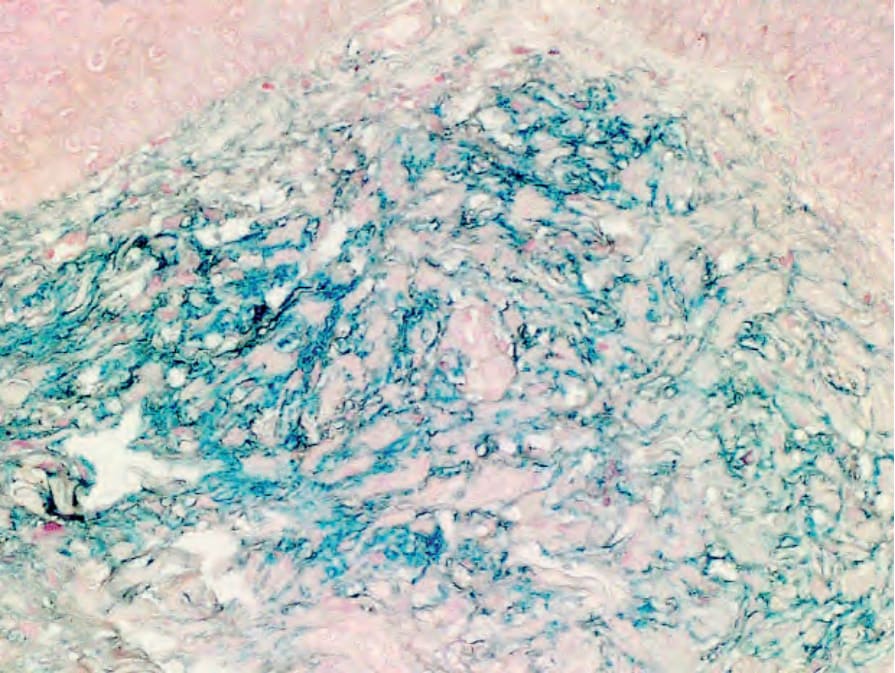
Fig. 13.193 Hereditary progressive mucinous histiocytosis. Colloidal iron highlighting prominent dermal mucin. By courtesy of C-K Sui, S-C Chao and J. Y-Y Lee, Tainan, Taiwan.

Fig. 13.194 Acanthosis nigricans: thickening of the skin of the groin. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.195 Acanthosis nigricans: there is velvety thickening of the axillary skin. By courtesy of the Institute of Dermatology, London, UK.

Fig. 13.196 Acanthosis nigricans: tripe palms. The palmar skin is thickened and the creases are accentuated. By courtesy of the Institute of Dermatology, London, UK.

Fig. 13.197 Acanthosis nigricans: the skin of the groins and vulva is thickened and hyperpigmented. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.198 Acanthosis nigricans: there is hyperkeratosis, papillomatosis, and slight acanthosis.