Mucinous nevus
Mucinous nevus
Clinical features Mucinous nevus (nevus mucinosis) is a rare lesion that may be congenital or acquired.1–8 The most common sites affected are either the trunk or lower limbs. Patients present with papules, nodules and/or plaquelike lesions, usually with a linear or dermatomal distribution.4 Large pedunculated lesions are rare.8,9 A familial case has been described in two young brothers.10
Pathogenesis and histologic features The pathogenesis is uncertain. Though no specific gene defect has been described, the familial clustering suggests either an autosomal dominant pattern of inheritance influenced by female hormones or, less likely, X-linked dominant inheritance that is lethal in utero to males. The fact that the eruption usually begins in the second decade and the occasional cases in males supports the former hypothesis.
Histologically, the lesion is characterized by a well-circumscribed proliferation of epithelioid histiocytes to spindled cells in the upper to mid dermis associated with increased dermal mucin (Figs 13.192 and 13.193).1–13 Dilated vessels may be present and occasional cases have increased mast cells.1,6 The cellular constituents may vary somewhat depending on the age of the individual lesion. In early lesions, the epithelioid cells may predominate while the spindled cells tend to be more numerous in older lesions.1,6 It has been hypothesized that cytokine production by the histiocytes results in fibroblast proliferation and angiogenesis, leading to the proliferation of spindled cells in older lesions.3
Histologic features Histologically, the mucin is located in the superficial dermis where it replaces the collagen and elastic fibers.5 Some cases are associated with epidermal hyperplasia and these may represent a combined epidermal and mucinous nevus.3,11 A case with dilated pores, termed follicular mucinous nevus, has been reported.12 A recent immunohistochemical evaluation demonstrated that the stromal cells are CD34 positive, with rare cells staining for factor XIIIA.13
Differential diagnosis These lesions must be distinguished from the mucinous eccrine nevus, which comprises abundant mucin surrounding eccrine glands and ducts.14
The immunophenotype is somewhat variable. The lesional cells are usually positive for lysozyme, but inconsistently positive for CD68.3,5,6,8–10 Generally, the histiocytic cells are positive for CD68, while the spindled cells are often negative. The histiocytic cells are also positive for alpha-1 antitrypsin, alpha-1antichymotrypsin, and CD31.1,6,9 The spindled cells may be positive for CD34.3 Variable positivity for factor XIIIa has been reported.6,8,10 Importantly, both the histiocytic and spindled cells are consistently negative
626 Degenerative and metabolic diseases
proliferation. Scleromyxedema is more widespread, less well circumscribed, has plasma cells, and is associated with a paraproteinemia. Although palisading has been reported in hereditary progressive mucinosis potentially causing confusion with granuloma annulare, necrobiotic collagen is not a feature of hereditary progressive mucinosis. Myxoid dermatofibromas are actually quite rare and would not present as multiple lesions.
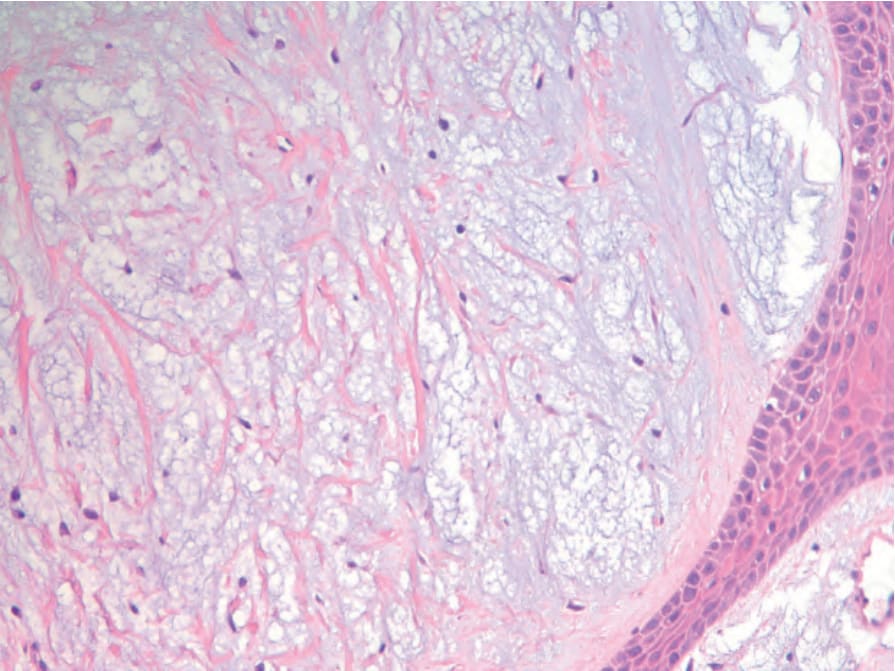
Fig. 13.192 Hereditary progressive mucinous histiocytosis. Nodular dermal infiltrate of histiocytes in a mucinous/myxoid background. By courtesy of C-K Sui, S-C Chao and J. Y-Y Lee, Tainan, Taiwan.