Lichen myxedematosus/scleromyxedema
Lichen myxedematosus/scleromyxedema
Clinical features As originally classified, there were four variants of this rare disease of adults.1 These were:
• generalized lichenoid papular eruption (Figs 13.169 and 13.170),
• discrete papular variant presenting as much smaller numbers of flesh-colored papules on the trunk and extremities (Fig. 13.171),
• localized and generalized lichenoid plaques mimicking lichen planus,
• urticarial or nodular lesions, which often evolved into the generalized papular form.2,3
With the subsequent delineation of new entities, the validity of this classification was called into question.4 Lichen myxedematosus is now divided into three forms:5–8
• a localized form, which includes several variants: discrete papular lesions occurring at any site, acral persistent papular mucinosis (see
below), self-healing papular mucinosis (see below), papular mucinosis of infancy (see below), and nodular mucinosis,
• a generalized form (scleromyxedema) characterized by lichenoid papules, indurated and thickened skin, and a monoclonal gammopathy; by definition, thyroid function is invariably normal,
617 The mucinoses
in tethering and limitation of movement, so that sclerodactyly, microstomia, and a mask-like facies may result (Fig. 13.172).4,11 Gross involvement of the glabellar skin sometimes causes a leonine appearance.11,13 A rare patient with leonine facies and tumor-like nodules mimicking lymphoma has been reported.14 The lack of acral calcification and absence of Raynaud phenomenon help to distinguish this condition from scleroderma. The mucous membranes are not usually affected.3 The lesions are variably pruritic.
There are occasional reports of systemic symptoms. Esophageal aperistalsis, peripheral neuropathy, proximal myopathy, and cardiac and cerebrovascular diseases have all been described.4,11,15,16 There has been little postmortem confirmation of visceral involvement and therefore it is likely that many of these associations are no more than coincidental. Neurological manifestations have, however, been reported most often and are probably of significance. They have included acute psychoses, encephalopathy and coma, epileptiform seizures, aphasia, memory loss, depression, and motor dysfunction.9,15–18 Dermatoneuro syndrome describes a rare manifestation of CNS disease where patients develop high fever, flulike symptoms followed by seizures, and coma.16,19,20 Carpal tunnel syndrome has also been reported fairly frequently.21–23 Pulmonary involvement is not uncommon and consists of restrictive or obstructive disease and pulmonary hypertension.16,24 Renal disease similar to that seen in scleroderma is rare.25,26 There is usually no relationship between lichen myxedematosus and neoplasia, but patients with underlying Hodgkin lymphoma, myeloid leukemia, hepatocellular carcinoma, thymic carcinoma, and seminoma has been reported.16,27–29 Rare cases associated with HIV infection have also been documented.30,31 Further associations include chronic hepatitis C and dermatomyositis.32–34 The latter finding is interesting because in the past, inflammatory myopathy not dermatomyositis has been described in association with scleromyxedema.35 It has been suggested that the development of myopathy is associated with a poor prognosis.35 A case associated with immune thrombocytopenia and atypical nodular lesions has been reported.36
• an atypical or intermediate form where patients may have generalized lesions without systemic symptoms/gammopathy, localized lesions with systemic symptoms/gammopathy or other manifestations that do not strictly fulfill criteria for either the localized or generalized variants. The generalized form of lichen myxedematosus (scleromyxedema) occurs equally in males and females and is seen most often in the fourth and fifth decades.3 It often presents on the hands and wrists, but soon becomes generalized although lesions are particularly seen on the hands, elbows, neck, face, and upper trunk.9–11 Prominent linear papules may be evident on the forehead, neck, axillae, and behind the ears.12 The papules are small, 2–3 mm in diameter, white or erythematous, and often have a waxy consistency. They tend to coalesce to form infiltrated plaques and, when associated with hardening and thickening of the underlying skin (scleromyxedema), result
Scleromyxedema is usually (but not invariably) associated with a paraproteinemia; most often this is IgG with lambda light chains.11,17,37–40 Occasionally it has been of the IgM or IgA class.3 An occasional association
618 Degenerative and metabolic diseases
A
The epidermis may be normal, acanthotic, or atrophic, and sometimes hyperkeratosis with parakeratosis is evident. In early lesions stellate fibroblasts are seen between disorganized collagen fibers in the reticular dermis (Figs 13.173 and 13.174).3,7 The papillary dermis is not affected. Increased numbers of mast cells are sometimes present.29 Focal deposits of mucin are readily identifiable (Fig. 13.175).2 A slight perivascular chronic inflammatory cell infiltrate is often seen in the superficial dermis.
B
In the more severe scleromyxedema variant, fibroblasts are numerous and there is consequent fibrosis and thickening of the dermis (Figs 13.176–13.178).4,45 Mucin deposits may be less evident or even absent.12 Decreased elastic fibers have occasionally been reported.3 A chronic inflammatory cell infiltrate is frequently present surrounding the superficial vasculature.
A less common granulomatous variant of scleromyxedema has been described in which there is an interstitial histiocytic infiltrate with giant cells, similar to granuloma annulare or interstitial granulomatous dermatitis.45–49 Although there is increased mucin, prominent stellate fibroblasts and dense bundles of collagen are not a feature. This variant may be more common than previously realized, representing close to 30% of cases in one series.45
Ultrastructural studies show active fibroblasts characterized by abundant rough endoplasmic reticulum and Golgi apparatus, increased numbers of mitochondria, and cytoplasmic inclusions accompanied by collagen deposition.50
with multiple myeloma has also been noted but occurs in less than 10% of patients.5,9
Pathogenesis and histologic features The pathogenesis of lichen myxedematosus is unknown. There is no evidence to suggest that the paraprotein is responsible for the fibroblastic proliferation. However, serum from scleromyxedema patients has been shown to contain a nonparaprotein-associated fibroblast growth factor. This requires further characterization.8,41 There is some evidence to suggest that the paraprotein may, however, have mucinogenic properties.42,43 Fibroblasts grown in tissue culture produce greater quantities of hyaluronic acid and sulfated glycosaminoglycans than normal controls.44 Collagen synthesis, as determined by H3-hydroxyproline estimations, is diminished.
Immunofluorescent studies have revealed immunoglobulin (IgG and to a lesser extent IgM) in the reticular dermis or just below the epidermis in 35% of cases.13 Indirect immunofluorescence is invariably negative.
Systemic involvement has only rarely been documented. Mucin deposition has been described in the adventitia of visceral blood vessels and in the renal papillae in single case reports.9,50 It has also been described within rectal mucosa and in muscle in one patient with scleromyxedema. Whether this represents true primary involvement or a secondary unrelated phenomenon is uncertain. In a particularly unusual case the features of systemic sclerosis were found in the kidney.9 In the absence of any autopsy evidence of further sclerodermatous lesions, it may be that the renal vascular and glomerular changes reflected unrecognized scleromyxedematous pathology. Demyelination and focal gliosis have also been reported.13,51 Nevertheless, autopsy studies have usually shown no evidence of widespread mucinosis, and it is likely that in the great majority of cases the pathological changes are limited to the skin.
619 The mucinoses
A
B
Differential diagnosis It may be impossible to distinguish scleromyxedema from nephrogenic systemic fibrosis based solely on histopathological features.52 Both conditions demonstrate an intradermal proliferation of spindled cells associated with increased mucin. The spindled cells stain for CD34, factor XIIIa, and procollagen I in both disorders. Although correlation with clinical parameters is critical for ultimate distinction between the two disorders, the depth of the infiltrate may be a helpful differentiating feature.53,54 In scleromyxedema the infiltrate is confined to the mid to deep dermis, whereas in nephrogenic
systemic fibrosis the process begins in the dermis but also extends into the septa of the subcutaneous fat. In the absence of adequate clinical information, the changes seen in established lesions of lichen myxedematosus may be confused with those seen in a dermatofibroma. Epidermal changes, polymorphism and hyalinization of collagen bundles at the periphery of the proliferation are absent in the former.
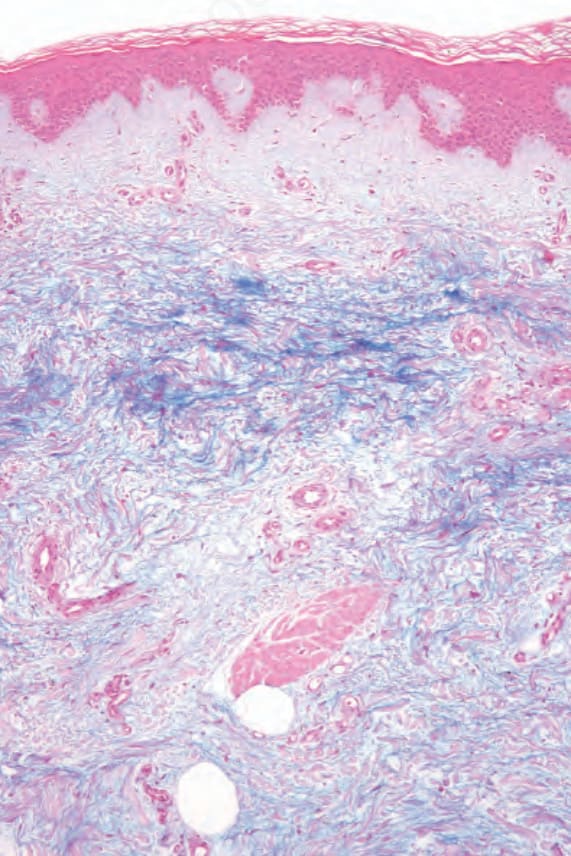
Fig. 13.168 Pretibial myxedema: the mucin (hyaluronic acid) stains positively with Alcian blue.

Fig. 13.169 Lichen myxedematosus: erythematous papules are widely distributed over the forearms. A more diffuse plaque is present over the dorsum of the left hand.
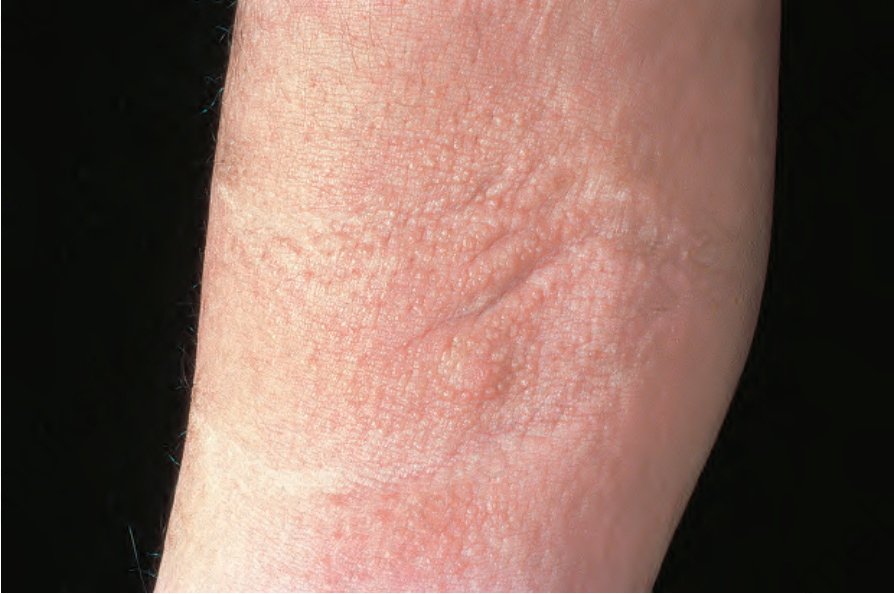
Fig. 13.170 Lichen myxedematosus: numerous papules are present in the antecubital fossa. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.171 Lichen myxedematosus: this is an example of the discrete papular form showing small numbers of papules on the anterior wrist. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.172 (A, B) Scleromyxedema: this severely affected patient shows sclerosis and linear papules on the forehead. Note the pinched, mask-like facies. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
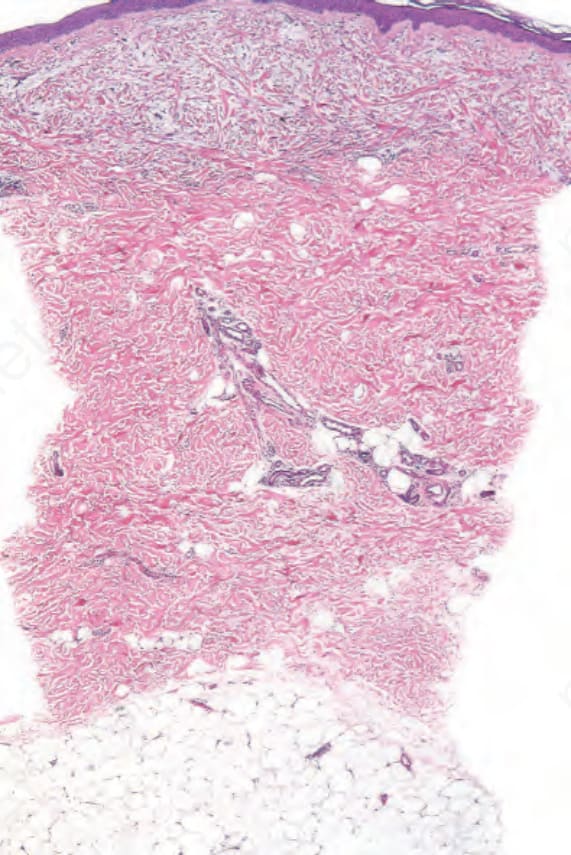
Fig. 13.173 Lichen myxedematosus: increased mucin is evident in the superficial dermis.
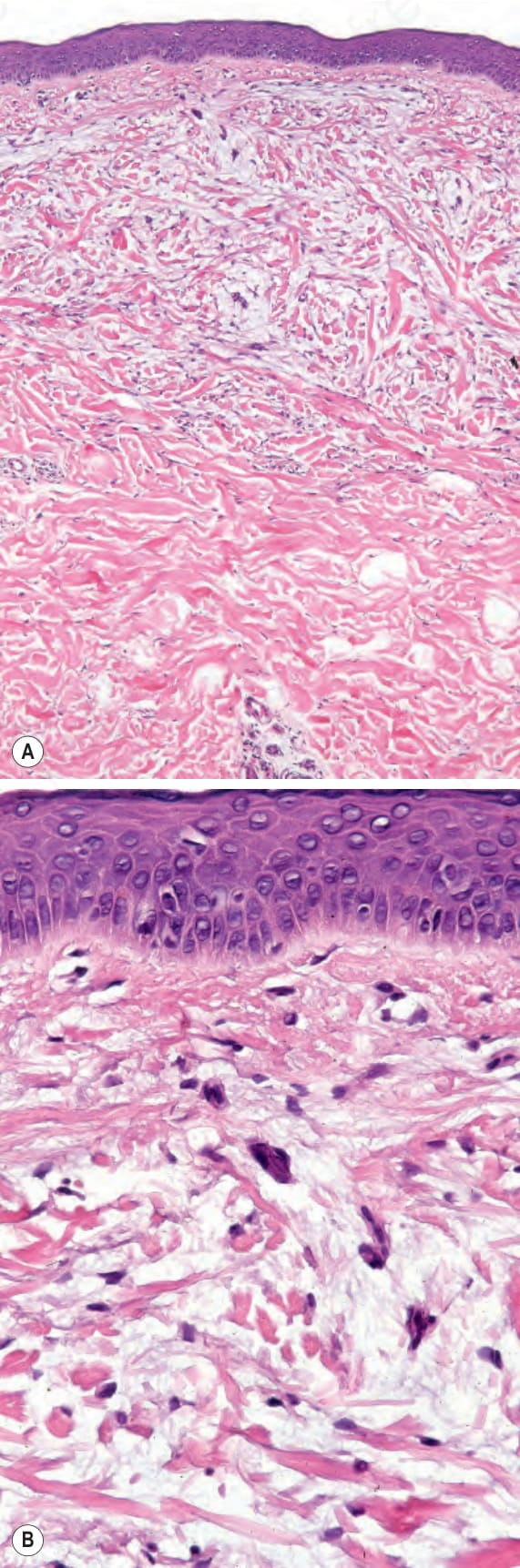
Fig. 13.174 (A, B) Lichen myxedematosus: the collagen fibers are widely separated by mucin deposits. Fibroblasts are increased in number.
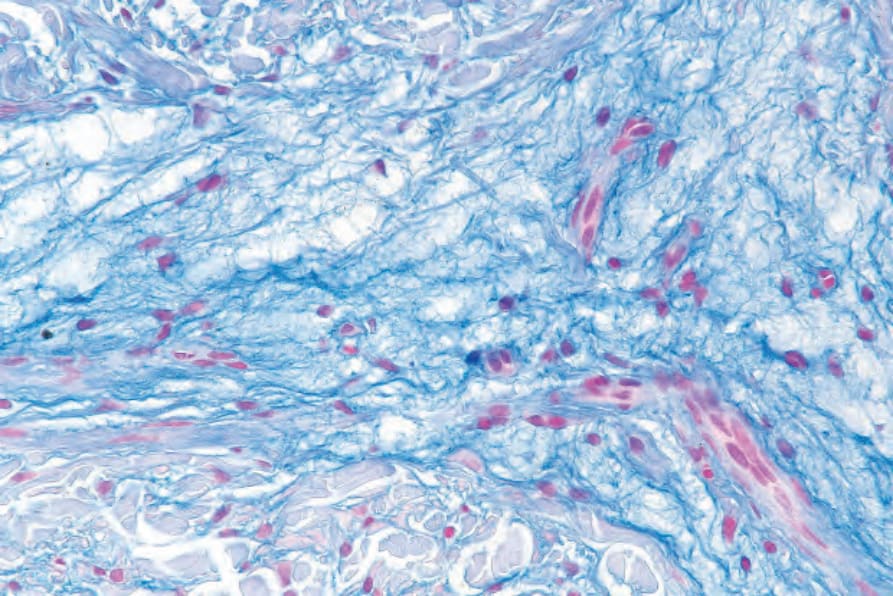
Fig. 13.175 Lichen myxedematosus: staining with colloidal iron emphasizes the mucin deposits.
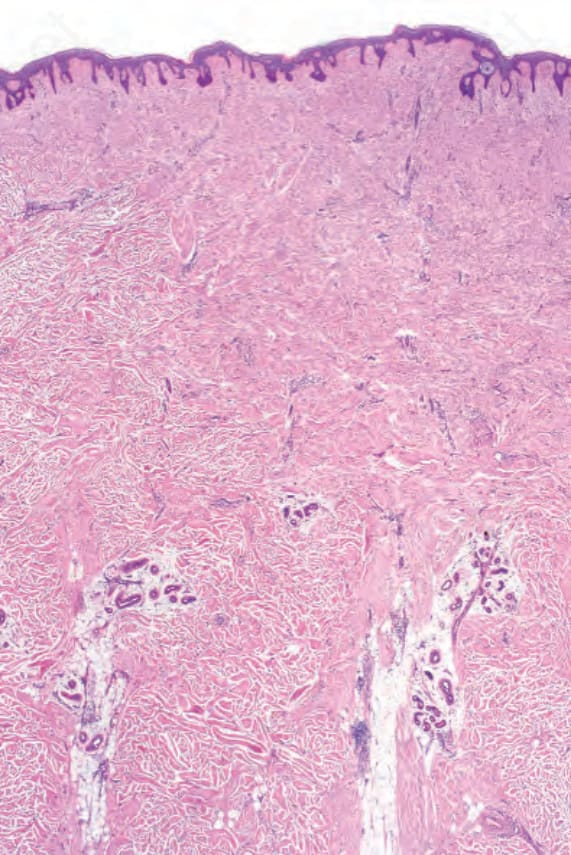
Fig. 13.176 Scleromyxedema: the dermis is markedly thickened. There is fibrosis and increased numbers of fibroblasts are evident.