Localized (pretibial) myxedema
Localized (pretibial) myxedema
B
prominence of the follicles, giving rise to a peau d’orange appearance, and secondary hypertrichosis is occasionally marked. Localized hyperhidrosis at the site of the myxedema may also rarely occur.9 The disease may progress to involve much of the lower leg, which rarely becomes grossly elephantiasiform (Fig. 13.165).2,10–13 The feet and toes sometimes can be involved.12,14 Small lesions are usually asymptomatic or mildly pruritic; the larger plaques are often painful.15 Infrequently, localized myxedema occurs on other sites, such as the arms, shoulders, abdomen, neck, face, and even the ears (Fig. 13.166).16 Nodular lesions rarely occur on the hands.17 Deposition on the forearm has been described as ‘preradial myxedema’.17,18 Occurrence at atypical sites is most likely related to trauma.19–21 For example, it has been described localized to scar tissue.20,22–24 The latter includes the site of a smallpox vaccination scar.25 Presentation at the site of a thigh donor graft site has also been reported.26
Clinical features Localized (pretibial) myxedema is most often associated with hyperthyroidism.1 It occurs in 3–5% of cases.2 It is one of three processes classically seen in autoimmune thyroid (Graves) disease, the other two being exophthalmos and thyroid acropachy (clubbing of the digits associated with subperiosteal new bone formation). Pretibial myxedema, also known as ‘Graves or thyroid dermopathy’, is usually a late manifestation of Graves disease and follows the development of Graves ophthalmopathy.3 It has only been reported exceptionally preceding the diagnosis of Graves disease and in the absence of ophthalmopathy.4 In 10% of cases of Graves disease, patients are not clinically hyperthyroid.5 They may be hypothyroid or euthyroid.5 Pretibial myxedema can rarely be associated with Hashimoto thyroiditis.6–8 Pink or yellow waxy plaques, nodules, and sometimes ‘tumors’ develop, most frequently first on the anterolateral aspects of the lower legs (Fig. 13.164). Lesions are classically nonpitting. In some patients there is induration with
Rare patients with pretibial myxedema have no evidence of thyroid disease. Biopsies from these patients tend to show changes associated with stasis and this feature is useful in the histologic differential diagnosis.27 One
615 The mucinoses
A
serum, but LATS is not believed to be causal.32 It was suggested in 1978 that a fibroblast stimulating factor associated with mucigenic properties isolated from the serum of patients with pretibial myxedema might play a role in the pathogenesis of the disease.33 Subsequent studies have shown that fibroblasts in pretibial skin and in the orbit of affected patients contain sequences identical to those of the thyroid stimulating hormone receptor.34,35 It has also been proposed that the fibroblasts might contain a cross-reacting protein rather than the true receptor, which binds with the autoantibodies against thyroid stimulating factor receptor.36,37 Based on these observations, it has been proposed that autoantibodies against thyroid-stimulating hormone receptor react with fibroblasts containing these sequences, resulting in production of cytokines and induction of increased glycosaminoglycan secretion.36,37
B
Localization to the legs most typically is thought to be due to dependency and mechanical factors.3 Additionally, tobacco is a known risk factor for the development of pretibial myxedema and Graves ophthalmopathy; however, the precise mechanism for this is presently unknown.3
The epidermis is often hyperkeratotic with follicular plugging; in gross cases, it may be papillomatous and acanthotic. The reticular dermis shows separation of collagen bundles by large quantities of mucin (Figs 13.167 and 13.168).1 Fragmentation of collagen fibers can be seen.3 Stellate fibroblasts are evident, but there is usually no increase in their number except perhaps in the more elephantiasiform examples. Lesions seen in the setting of lymphedema and obesity are also characterized by small vessel angiogenesis, vessel wall thickening, edema, and hemosiderin deposition.28,29
such variant has been described in morbidly obese patients with lymphedema.28,29 Lesions occur as papules, vesicles, and nodules on the pretibial surfaces.
Pretibial myxedema is sometimes self-limiting, involution occurring after a number of years. Complete remission occurs in up to 26% of cases but this depends on the severity of the disease.5,30
An exceptional form of pretibial mucin deposition that may be confused with pretibial myxedema associated with Graves disease has been documented in association with Sjögren syndrome under the name acral ichthyosiform mucinosis.31 In the cases described, the patients had normal thyroid function tests and the mucin deposition was predominantly in the papillary dermis.
Pathogenesis and histologic features The etiology is uncertain; the presence of pretibial myxedema is usually associated with detection of long-acting thyroid stimulator (LATS) in the
Immunofluorescent studies are usually negative, although granular deposits of IgM have been identified within the superficial papillary dermis.15
Electron microscopic studies show amorphous granular material both within fibroblast endoplasmic reticulum, coating the surface of the fibroblast, and in the interstitium surrounding the widely separated collagen and elastic fibers.11 Tubuloreticular structures have been identified in the cytoplasm of endothelial cells in one case and in the dermis of another.15,22
616 Degenerative and metabolic diseases
A
B

Fig. 13.163 (A, B) Generalized myxedema: this patient has widespread xanthomata. By courtesy of the Institute of Dermatology, London, UK.
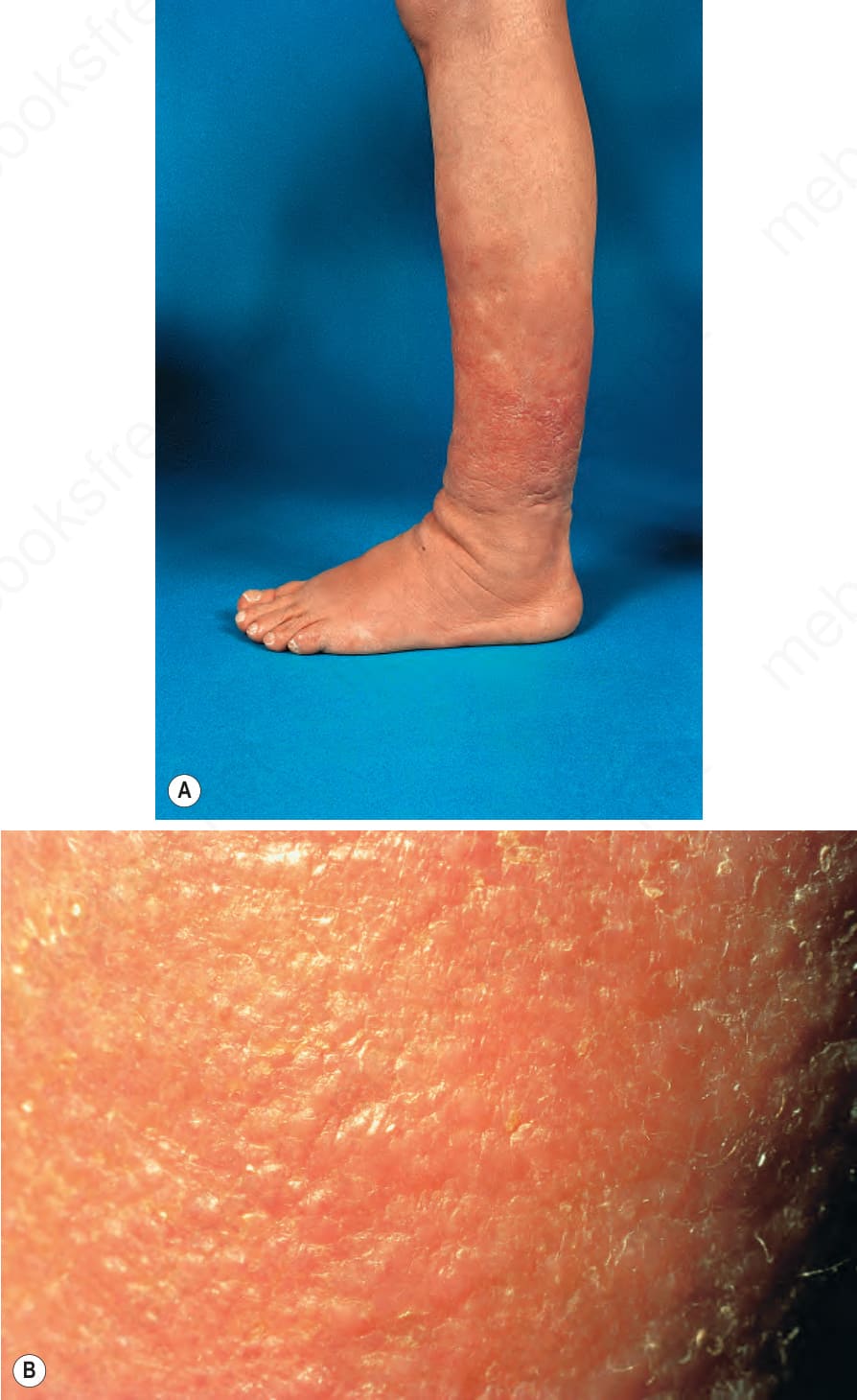
Fig. 13.164 Pretibial myxedema: (A) erythematous, somewhat translucent plaques are present over the shin; (B) close-up view. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.165 Pretibial myxedema: in this extreme example, the features resemble elephantiasis. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.166 (A, B) Localized myxedema: these pictures came from same patient shown in Fig. 13.162. Following a road traffic accident, the patient developed additional mucinous deposits on her arm close to the site of a fracture. By courtesy of P.G. Goodwin, MD, The Royal Bournemouth Hospital, UK.
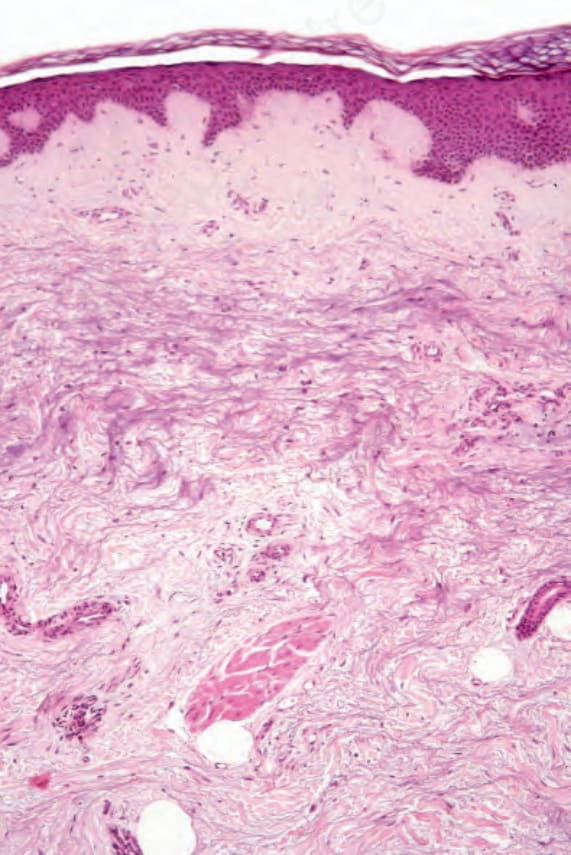
Fig. 13.167 Pretibial myxedema: there is loss of collagen fibers associated with mucin deposition.