Metastatic calcinosis cutis
Metastatic calcinosis cutis
Clinical features Metastatic calcification occurs as a result of hypercalcemia or hyperphosphatemia as may be seen in chronic renal failure, hyperparathyroidism, and sarcoidosis.46–49 It has also been reported secondary to leukemia.50–52 Calcium deposits occur in the skin, subcutaneous tissues, muscle, tendon, and internal organs. In the skin, the clinical appearances are of hard nodules and plaques, which may ulcerate to liberate chalky material and ultimately leave a scar (Fig. 13.148). This may be particularly frequently seen over large joints, the iliac crest or in the flexures. Fingertip lesions are usually very painful. A case report describes a patient with vulvar cystic nodules and hyperphosphatemia.53
610 Degenerative and metabolic diseases
patients have coexisting syringomata. An association with acne is rarely seen. Lesions resolve spontaneously without scarring.
Pathogenesis and histologic features Calcium stains blue with hematoxylin and eosin. In calcinosis cutis a rather homogeneous deep blue material is seen, either as small superficial deposits or as deeper globular ones (Fig. 13.152). Owing to the concomitant presence of phosphate and carbonate, the deposit stains black with the Von Kossa stain (Fig. 13.153).
The presence of calcium in the skin variably excites a foreign body reaction, so giant cells are sometimes seen at the edge of the deposit. On other occasions a chronic inflammatory cell infiltrate is present. Transepidermal elimination of calcified debris is sometimes a feature.4
• In tumoral calcinosis, large deposits of calcium are present in the skin and subcutaneous tissues, typically over bony prominences (hip, elbow, and scapula) (Figs 13.149 and 13.150). It is rare in Europe and North America, but is not uncommon in South, Central and East Africa and Papua New Guinea, where it is known as hip stone. It shows a female preponderance (2 : 1) and affects younger age groups. These deep deposits may be visualized radiologically (Fig. 13.151). Although most cases are idiopathic, there is a genetic defect is a small percentage, discussed below.
• Scrotal calcinosis may occur spontaneously. Patients present in childhood or early adulthood with multiple, asymptomatic, flesh-colored or yellow nodules of varying sizes, which often release granular chalky material.87 A similar finding on the penis has also been reported in young men with no prior history of trauma and without a known underlying adnexal lesion.88
• Finally, milia-like idiopathic calcinosis cutis is a rare condition seen in children (usually under the age of 21 years).89–93 Lesions are multiple, skin colored to whitish papules with a generalized distribution. Perforation may occur. Most cases are idiopathic. Two-thirds of cases have been associated with Down syndrome and up to one-third of
Dystrophic calcification due to extravasation of intravenous solutions containing calcium is characterized by dermal calcium surrounding degenerated collagen bundles.22 Lesions caused by calcium-containing heparin also demonstrate calcium in fat lobules, surrounding adipocytes, in septa as well as within the media of small vessels in the subcutaneous fat and dermis.22 There may be fibrosis of vessel walls; however, thrombosis is not a usual feature.24,26
In calciphylaxis, there is prominent calcification of walls of dermal and subcutaneous small blood vessels (Fig. 13.154).64 Often, the findings also include some degree of intimal proliferation and thrombosis. These changes result in prominent ischemic necrosis with extensive fat necrosis. Calcification of the surrounding fat may also be seen.
The pathogenesis of calciphylaxis is not completely understood. Recent studies point to osteopontin as a possible factor.65,94 Osteopontin is a phosphoprotein adhesion molecule with a high affinity for calcium. It is normally expressed by various cell types, including osteoblasts, osteocytes, fibroblasts, macrophages, and smooth muscle cells. It plays an important role in bone remodeling. Previous studies have suggested a role for osteopontin in calcification of heart valves and pilomatrixoma.95,96 Osteopontin expression in the media and, less often, the intima of vessel walls and surrounding adipocytes in the subcutaneous fat in areas involved by calcification in calciphylaxis has been demonstrated.94 Calciphylaxis may in part be caused by osteogenic differentiation of vascular smooth muscle cells.
Calcification deposits in nephrogenic systemic fibrosis occur in the dermis, associated with CD34-positive spindle-shaped cells and in the media of small arteries in the deep dermis and subcutaneous fat, similar to that seen in calciphylaxis.45
611 Calcinosis cutis
A
In tumoral calcinosis the histologic features depend upon the stage of evolution of the lesion (Figs 13.155–13.157).98 In early examples, multiple cystic spaces lined by epithelioid and giant cells are seen. The cyst lumina contain eosinophilic debris undergoing calcification. In advanced lesions, densely calcified material is seen embedded in hyalinized connective tissue. The occasional finding of necrobiosis and vasculitis may have pathogenetic significance. In the familial form of tumoral calcinosis, mutations in FGF23, GALNT3, or KLOTHO may be seen.99–102 These mutations result in hyperphosphatemia with increased phosphate reabsorption, elevated 1,25-dihydroxyvitamin D(3), and deposition of large calcific masses.
B
A report of an exceptional case of metastatic calcification showed calcification only of sweat ducts.97
There may be histologic evidence of the underlying disease process. In localized dystrophic calcinosis, for example, there is sometimes evidence of a preceding cyst particularly of the trichilemmal variant. In widespread dystrophic calcinosis cutis secondary to connective tissue disease, there is occasionally evidence of preceding collagen degeneration.
In a subepidermal calcified nodule, there is sometimes pseudoepitheliomatous hyperplasia, associated with transepidermal elimination of calcium.
The pathogenesis of the scrotal variant is most probably calcification of the contents of pre-existent dermal cysts, mostly epidermoid, but occasionally pilar.90,103–108 Some authors have failed to detect an epithelial component;54 however, this may be a reflection of the age of the lesion. In two different studies, residual epidermal cysts were present in over 50% of cases.106,108 In many examples, typical epidermoid lining epithelium surrounds the calcified deposit and sometimes residual keratinous contents are visible. A foreign body giant cell reaction is not uncommon.
The etiology of milia-like calcinosis cutis is unclear. Theories include increased calcium content of excreted sweat and calcification of a pre-existing cyst.89 Histologically, there is a focus of calcium in the papillary dermis
612 Degenerative and metabolic diseases
surrounded by a lymphocytic infiltrate and giant cells. Perforation may be present.89–93 Cyst epithelium is not present.

Fig. 13.148 Metastatic calcinosis cutis: there are gross deposits, many ulcerated. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.149 Tumoral calcinosis: bilateral nodules over the elbows, with perforation on the patient’s left. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
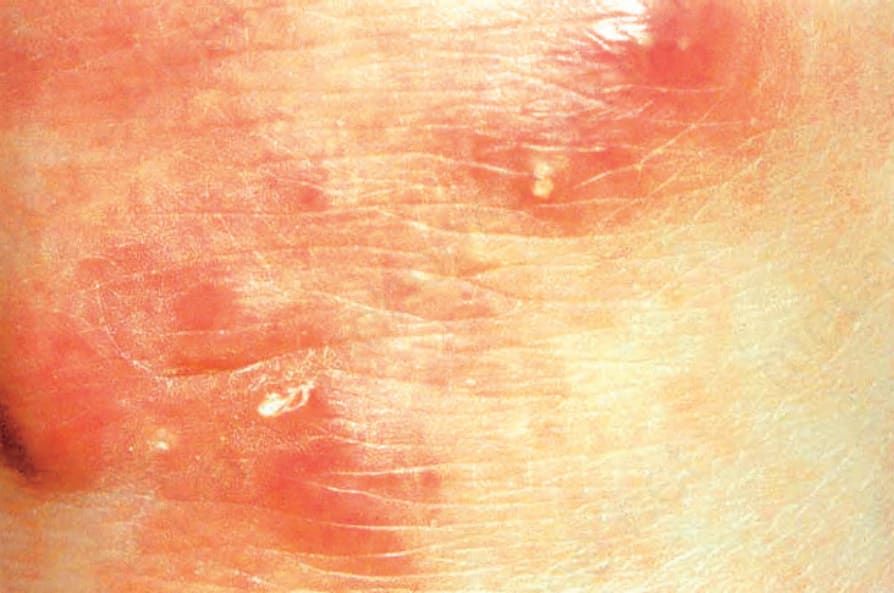
Fig. 13.150 Tumoral calcinosis: these small deposits are undergoing transepidermal elimination. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
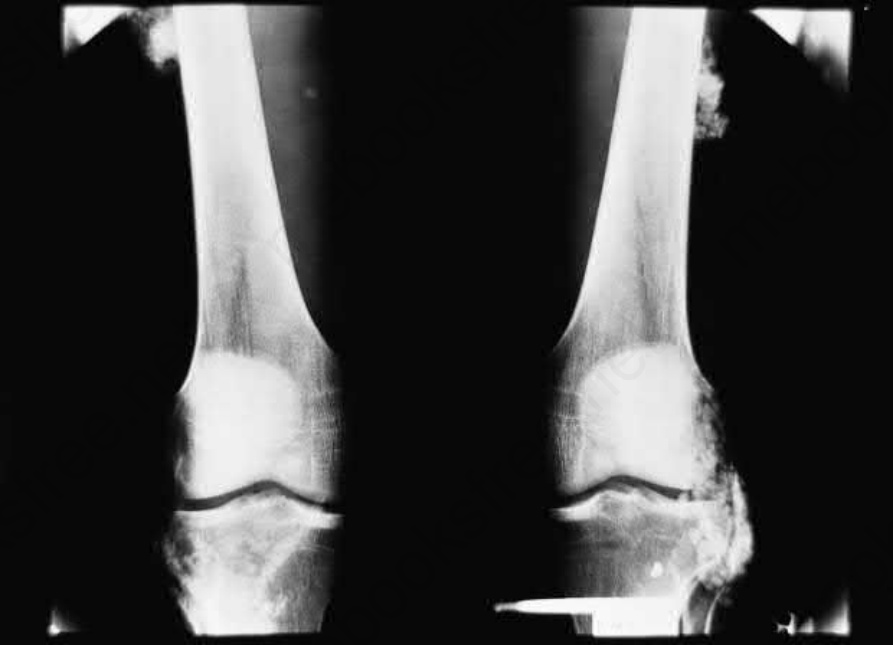
Fig. 13.151 Tumoral calcinosis: subcutaneous deposits are present overlying the thigh and lateral border of the knee. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
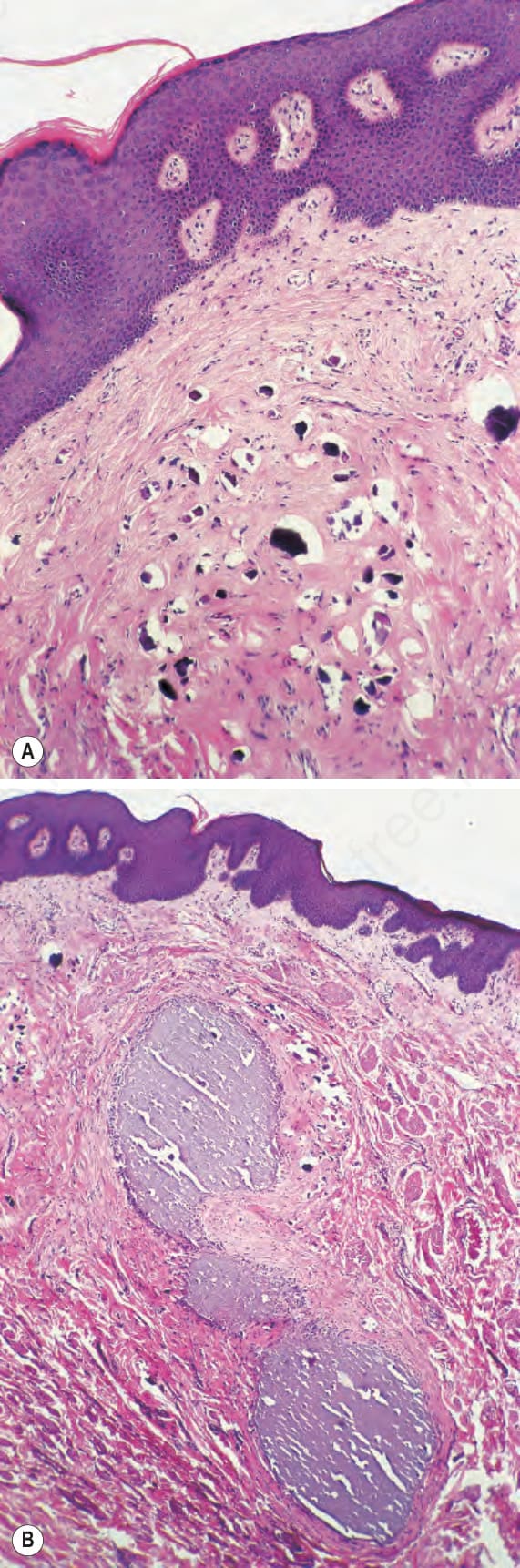
Fig. 13.152 Calcinosis cutis: (A) small deposits of intensely basophilic material are present in the superficial dermis; (B) these calcium deposits are associated with scarring.
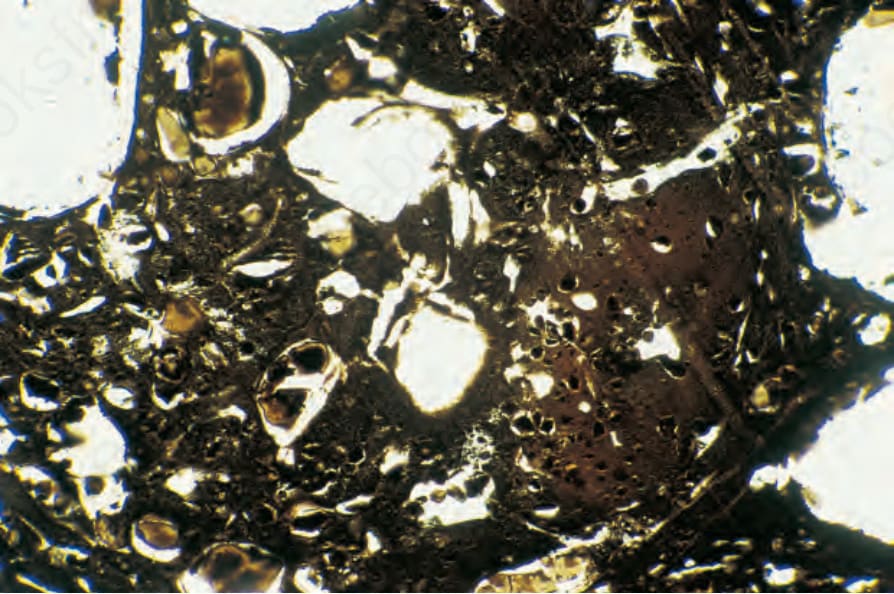
Fig. 13.153 Calcinosis cutis: the calcified deposit stains positively with the Von Kossa reaction.
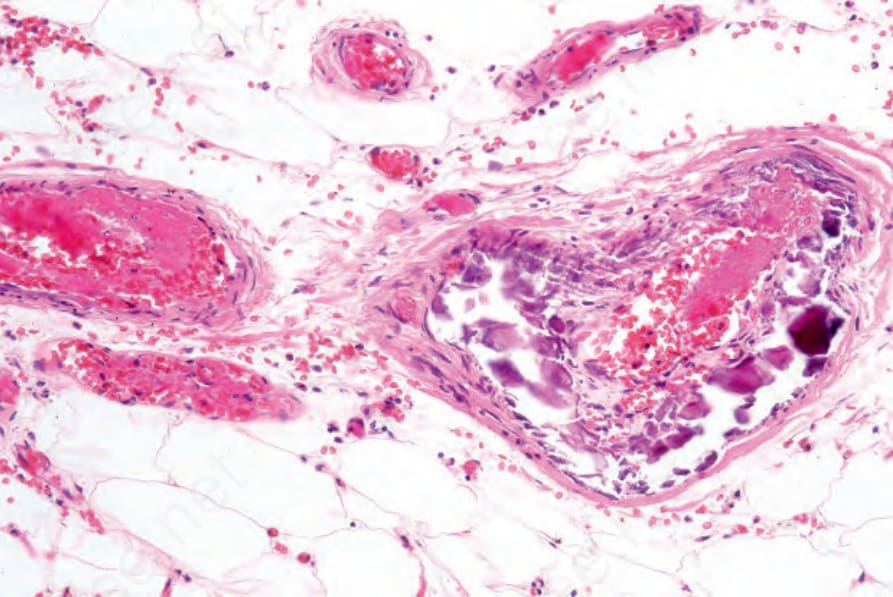
Fig. 13.154 Calciphylaxis: note the subendothelial calcification and thrombosis.
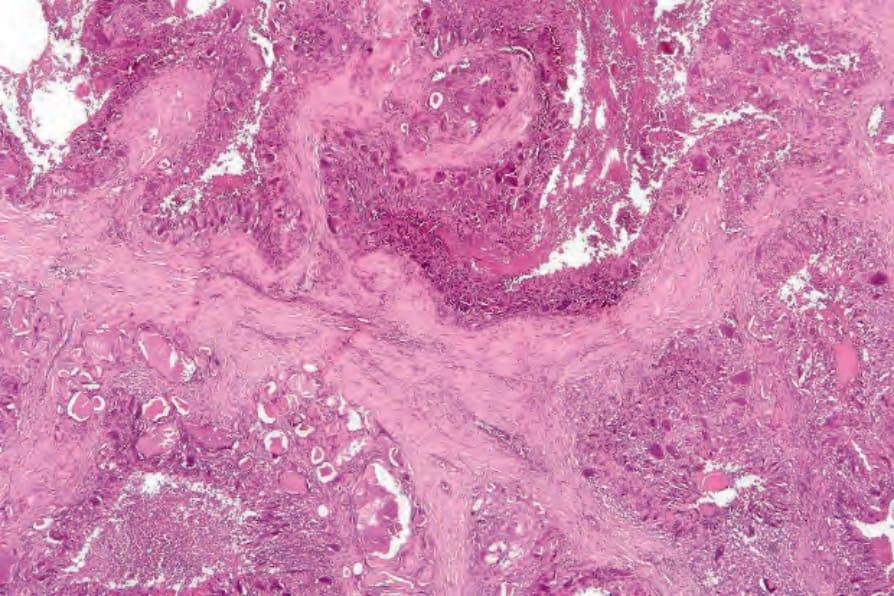
Fig. 13.155 Tumoral calcinosis: this low-power view shows a dense hyalinized stroma with numerous cystic cavities containing necrotic and calcified debris.