Dystrophic calcinosis cutis
Dystrophic calcinosis cutis
Clinical features In this, the most common variant of calcinosis, the changes are limited to the dermis and subcutaneous tissues and there is no involvement of internal organs. This form of calcinosis always occurs in tissue that has been previously damaged either by external agents or as the result of a disease. Under this variant, iatrogenic calcinosis cutis induced by local application of chemicals or medications is also included. In the localized form of dystrophic calcinosis cutis, the underlying anomaly may be inflammatory or traumatic in nature, for example acne scars, burns, fat necrosis or subcutaneous and intramuscular injections.4–7 Calcification and necrosis have been reported following electroencephalography and electromyography.8,9 Calcification is a characteristic feature of pancreatic disease-associated panniculitis and in older lesions of subcutaneous fat necrosis of the newborn. Auricular calcification (also known as ‘petrified ear’) may occur as a result of chondritis, trauma or frostbite.1,10,11 Less commonly, it is associated with hypercalcemia associated with systemic disorders and endocrinopathies.10,11 A distinct example of dystrophic calcification is infantile calcinosis cutis of the heel, in which calcific dermal nodules develop approximately 1 year after birth in infants who have had multiple heel punctures for venesection.12,13 A rare case as a complication of radiation therapy for breast cancer has been described.14 An exceptional case following cutaneous exposure to a calcium chloride solution has been reported.15
Localized dystrophic calcinosis may also complicate epithelial cysts or neoplasms (Fig. 13.144).16 It is particularly seen within the keratin of trichilemmal cysts. Calcification may occur in many adnexal tumors, for example pilomatrixoma, desmoplastic trichoepithelioma, and microcystic adnexal carcinoma. It is much more common in basal cell carcinoma than in squamous cell carcinoma.17,18 Subungual epidermoid inclusions are rare tumors of the nail bed in which calcification may occur.19
Calcinosis cutis has also been documented following the intravenous administration of calcium chloride, phosphate, and gluconate (iatrogenic calcinosis cutis) (Fig. 13.145).20–23 Lesions consist of multiple, erythematous nodules, which can ulcerate. They usually develop within a few weeks of exposure.22 Deep soft tissue calcification has been described in association with pentazocine and pitressin.23,24 Similar reactions following calcium-containing heparin in patients with renal insufficiency have also been reported.25,26
Widespread dystrophic calcification occurs most commonly as a sequel to connective tissue disease (Figs 13.146 and 13.147). Localized dystrophic calcification with bone formation has also been described in mixed connective tissue disease.27,28 Dermatomyositis, especially in children, may be complicated by extensive deposits of calcium in the skin and subcutaneous tissues, muscles, and tendons and the dystrophic calcification may be
609 Calcinosis cutis
the presenting sign.29,30 Scleroderma, especially the CREST variant, tends to show localized deposition of calcium, particularly on the digits and over bony prominences. Fingertip lesions are a common presentation in patients with Raynaud phenomenon (with or without underlying connective tissue disease) and have also been reported in a patient with Sjögren syndrome who did not have Raynaud syndrome.31,32 Systemic lupus erythematosus is infrequently associated with calcinosis.33,34 It is usually an incidental radiological observation, most commonly seen in the buttocks and extremities and unassociated with panniculitis. Mostly it develops in patients with severe acute disease, including cardiac, renal, or CNS manifestations.2 It also appears to correlate with high doses of corticosteroids and myositis.35,36 Calcification complicating discoid lupus erythematosus and subacute lupus erythematosus is limited to isolated case reports.37–39 Lupus panniculitis and other types of panniculitis (including pancreatic fat necrosis) may also be associated with calcification.40 Patients with porphyria cutanea tarda rarely develop calcinosis cutis. Lesions are most common on the scalp, neck, preauricular area, and hands, and are more likely to develop in patients with sclerodermoid disease.41 Calcium is also deposited in inherited connective tissue disorders, especially Werner syndrome, pseudoxanthoma elasticum (PXE), and Ehlers-Danlos syndrome, in which small calcific nodules typically develop within atrophic scars over bony prominences. Alternatively, dystrophic calcification in PXE may occur as large, painful, pruritic nodules in areas involved by the underlying disease.42
Albright hereditary osteodystrophy is a genetic disorder associated with end-organ resistance to parathyroid hormone. Patients present in infancy or childhood with obesity, short stature, mild mental retardation, shortened fourth and fifth metacarpals, cutaneous calcification, osteoma cutis, and calcifying aponeurotic fibroma-like lesions.54–56 The skin lesions are typically multiple erythematous to purpuric papules, plaques, and nodules on the trunk and extremities.
Vascular calcification with thrombosis may lead to livedo reticularis, ulceration, and gangrene, particularly affecting the hands, fingers, toes, and lower legs (so-called clinical calciphylaxis).49,57,58 A frequent complication is sepsis and this often results in death. Patients usually have chronic renal failure in association with hyperphosphatemia and hyperparathyroidism.59–61 Other conditions associated with calciphylaxis include hypervitaminosis D and A, hypercalcemia, primary or secondary hyperparathyroidism, AIDS, and protein C deficiency.62,63 The exact mechanism of calciphylaxis is not clear, but it seems to be related to an imbalance in calcium and/or phosphorus metabolism.64,65 Rarely, the condition occurs in patients with normal levels of calcium and phosphorus.64–68
Calcification has been described in patients with nephrogenic systemic fibrosis, associated with the cutaneous lesions as well as in fascia and muscle.43,44 The etiology of calcification in this disease is debated. Some believe it occurs secondarily as part of a dystrophic process while others contend that calcification is intrinsic to the pathological process, particularly as it is also seen in vessels, in patterns resembling calciphylaxis.45
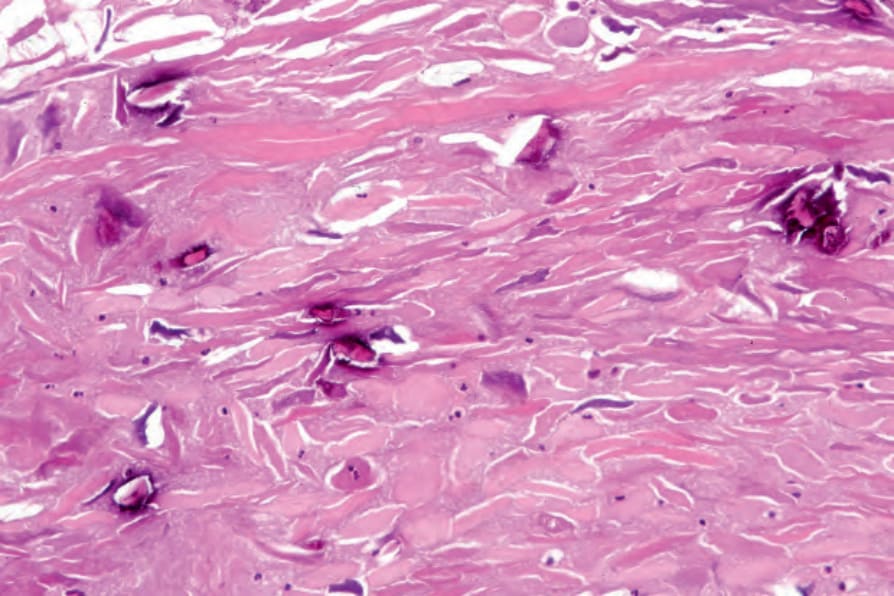
Fig. 13.144 Dystrophic calcinosis cutis: calcification has developed in this ruptured cyst.
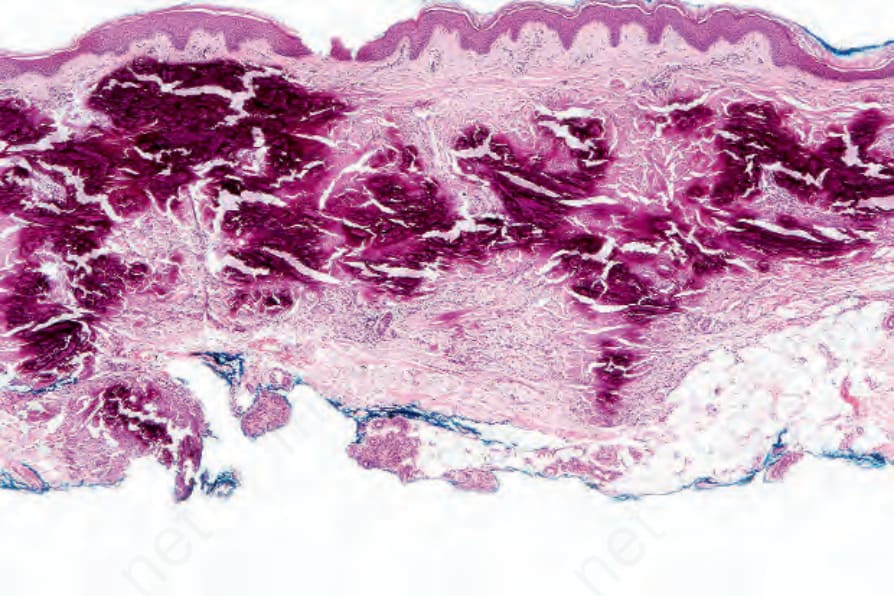
Fig. 13.145 Iatrogenic calcinosis cutis: this widespread dermal calcification followed calcium gluconate infusion.

Fig. 13.146 Dystrophic calcinosis cutis: this large deposit is associated with focal ulceration and transepidermal elimination. By courtesy of the Institute of Dermatology, London, UK.

Fig. 13.147 Dystrophic calcinosis cutis: multiple digital deposits are present. By courtesy of the Institute of Dermatology, London, UK.

Fig. 13.148 Metastatic calcinosis cutis: there are gross deposits, many ulcerated. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.