Alkaptonuria
Alkaptonuria
Clinical features This is an autosomal recessively inherited condition (with an approximate incidence of 1 : 106) in which deficiency of homogentisate 1,2-dioxygenase (HGD) in the liver and kidneys (necessary for the catabolism of phenylalanine and tyrosine) leads to the accumulation of homogentisic acid (2,5-hydroquinone acetic acid) in cartilage, tendon, skin, and fibrous tissue.1–5 The condition is particularly seen in patients of Eastern European origin, mainly those from Slovakia where the incidence is as high as 1 : 19 000.6 Clinical features relate particularly to joint and cardiovascular involvement, renal and prostatic stones, and ocular and cutaneous lesions. Alkaptonuria, or blackening of the urine after standing or alkalinization due to oxidation of homogentisic acid, usually becomes obvious in childhood. Most patients present with either dark urine or early-onset arthritis. The blue–black discoloration of the tissues (known as ochronosis) is due in part to the Tyndall effect.
604 Degenerative and metabolic diseases
A
B
patients and mainly consists of pigmentation and calcification of the aortic valve, which may lead to stenosis.17–20 The cardiac manifestations appear to be independent from other cardiac risk factors.20 Cardiovascular pigmentation, which is especially seen on the endocardium and valves (aortic and mitral), also affects the intima and media of arteries. Surprisingly, even with heavy pigment deposition and smooth muscle cell degeneration, aneurysm formation is not a feature of vascular involvement.21
In up to 60% of patients the kidneys typically show very marked pigmentation, especially involving the pyramids and calculi.22 Ochronotic prostatic stones are a nearly invariable feature, but bladder calculi are much less frequent.4,21 In addition to stones, patients may develop chronic renal disease.15,16 A case with a rapidly fatal course in a patient with chronic renal disease has been reported. This patient had intravascular hemolysis related to toxic effects from elevated plasma soluble melanins due to accumulation of homogentisic acid that precipitated acute renal failure.23 Asymptomatic ocular involvement is seen in up to 70% of patients.24 Pigmentation particularly affects the sclera and to a lesser extent the conjunctiva and cornea.7,21 The lesions are typically noninflammatory.
The cutaneous changes develop later, at about 30–40 years of age. They are seen particularly on sun-exposed skin and areas with maximum numbers of sweat glands.1–4 Deposition of polymerized oxidase pigment in the ear cartilage produces painful thickening and blue–black speckled discoloration. Involvement of the eardrum and ossicles may result in tinnitus and deafness.4 Subsequently, discoloration of the sclera, conjunctiva, tendons, and skin of the face, hands, and flexures occurs.7 A rare case of vaginal hyperpigmentation has been reported.8 The skin pigmentation may be more prominent on the palms and soles.9,10 Finally, a characteristic arthritis, which is often severe, develops in almost all patients.4,11 Low back pain is followed by involvement of the large joints of the limbs. Spinal involvement leads to disc herniation, spondylosis, and osteophytosis with resultant limitation of movement and loss of height.1,12 Musculoskeletal disease caused by alkaptonuria can be severe and result in significant disability.13,14 Despite widespread morbidity, alkaptonuria is not associated with significant mortality, and life expectancy is typically normal, though mortality related to renal disease or cardiac complications has been reported.1,15,16
Ochronotic pigmentation is frequently seen in the hyaline cartilage of the larynx, trachea, and bronchi.21,25 Involvement of endocrine organs, CNS, and teeth is rare.26–28
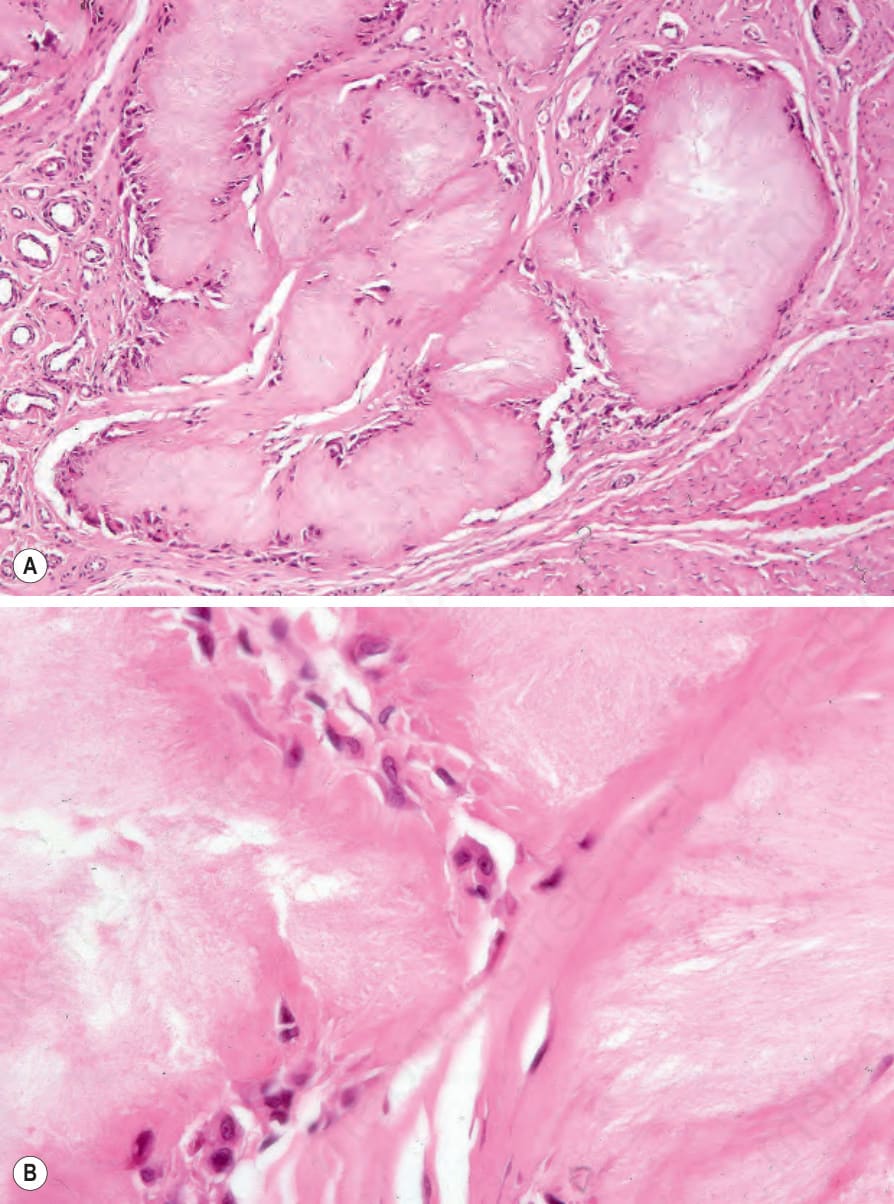
Fig. 13.132 Gout: (A) circumscribed deposits of uric acid are scattered within the dermis, note the accompanying fibrosis; (B) formalin fixation has destroyed the uric acid crystals to leave amorphous eosinophilic material.
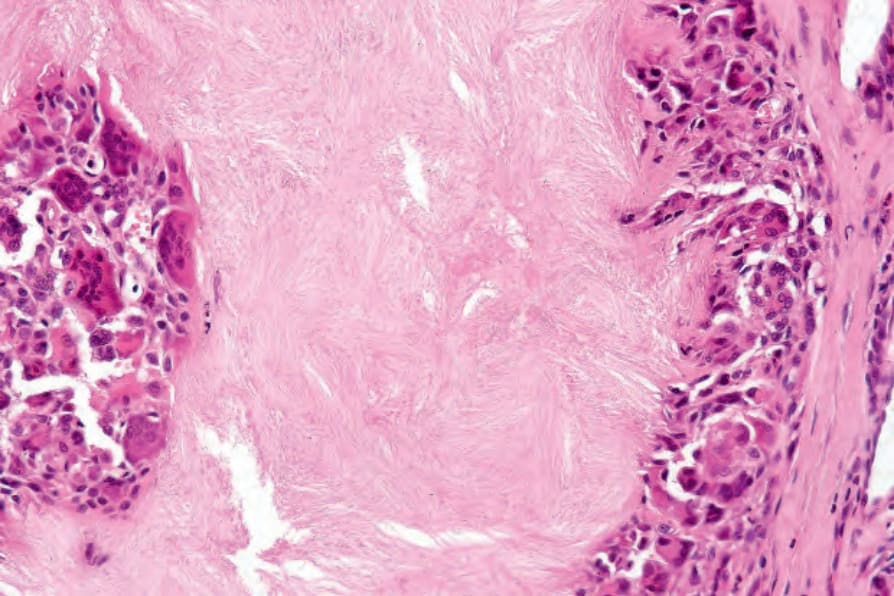
Fig. 13.133 Gout: multinucleate giant cells are present.
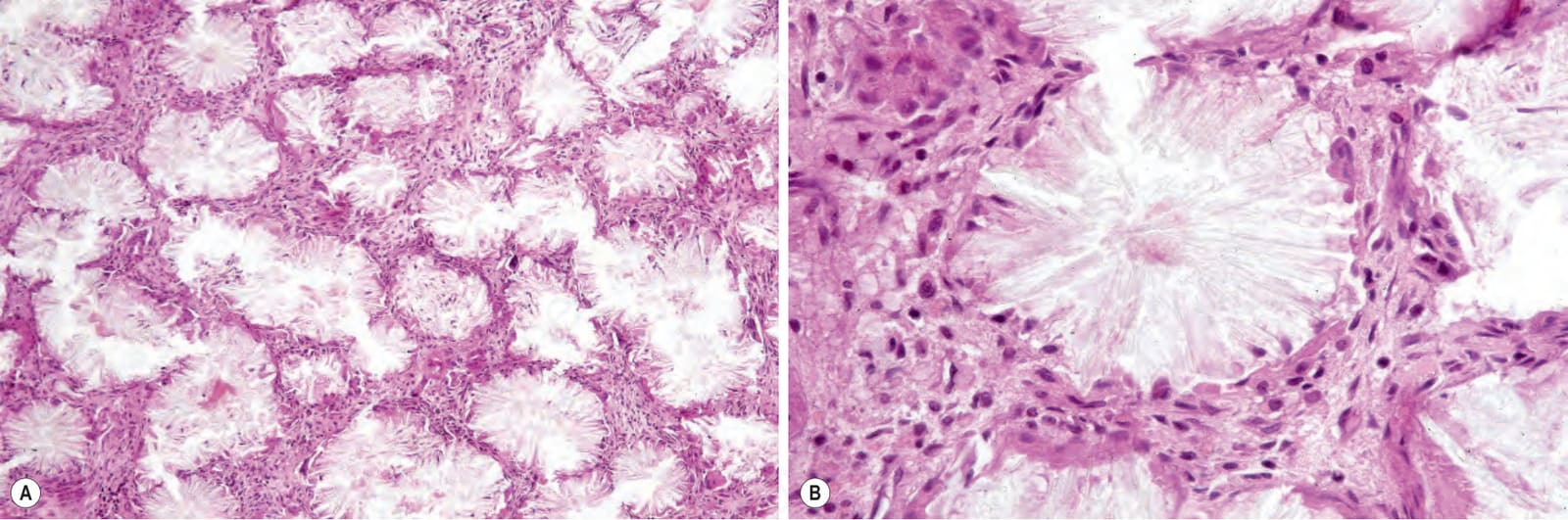
Fig. 13.134 (A, B) Gout: characteristic needle-shaped uric acid crystals are seen in alcohol-fixed and anhydrous processed material.
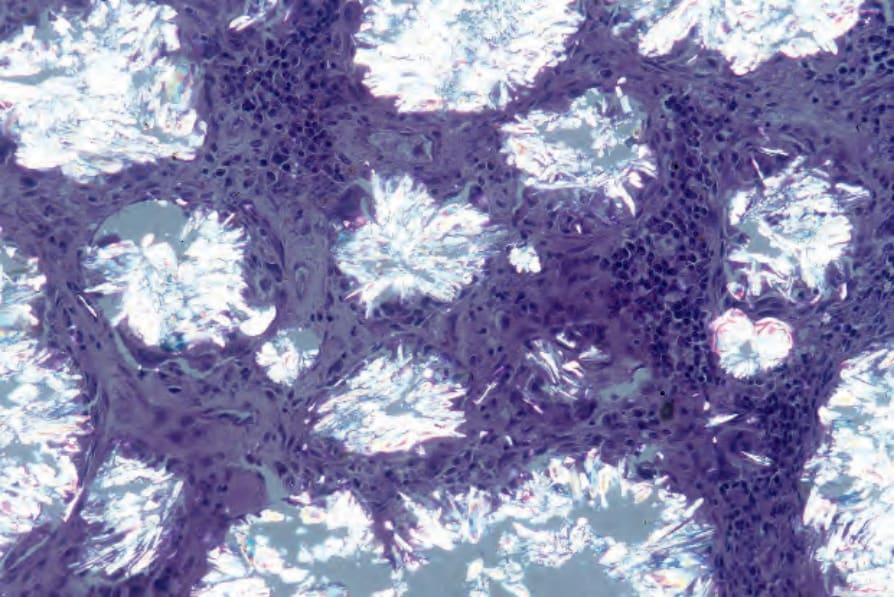
Fig. 13.135 Gout: the crystals display striking birefringence when viewed with polarized light.