Gout
Gout
Clinical features Gout represents a group of disorders of purine metabolism in which elevated levels of uric acid occurs.1–4 The majority of affected patients have reduced excretion of purines which may be caused by diuretic therapy or renal disease. Hyperuricemia may also complicate diabetic ketoacidosis and starvation, and can develop in patients with sarcoidosis and psoriasis.5,6 Some have increased purine synthesis and this type of disturbance can occur dramatically in the myeloproliferative diseases, particularly following
602 Degenerative and metabolic diseases
A
B
A
B
present with tophi because of improvement in the diagnosis and treatment of the disease.25 Tophi are rarely the first manifestation of the disease.26,27 They have exceptionally been described in the mitral valve, breast, nose, cervical spine, sacroiliac joint, larynx, and eyes.28–34 Bone involvement gives rise to characteristic lytic lesions in the distal subchondral region of the digits.4 Fracture due to bone erosion has been reported.35
Renal disease, which is an important complication, presents as urate nephropathy and/or uric acid nephrolithiasis.20,36,37 In secondary types associated with increased cell turnover, including myeloproliferative disease and multiple myeloma, acute precipitation of uric acid crystals sometimes occurs in the collecting ducts of the kidney during chemotherapy. Uric acid nephropathy may also develop in patients with the inherited variants. Patients present with acute renal failure. More commonly, in primary gout, renal stones are a feature, and chronic urate nephropathy (due to deposition of monosodium urate monohydrate salt crystals in the interstitial tissues of the kidney), presenting as mild proteinuria and hypertension, occasionally develops.4 Uric acid stones develop in about 40% of patients with gout secondary to myeloproliferative diseases and in 10–25% of patients with the primary variants.4
The diagnosis of gout rests primarily on the identification of uric acid crystals within joint fluid or tophi rather than on serum uric acid levels,
603 Ochronosis
A
which can be unreliable. Acute attacks of gout can be associated with normal uric acid levels.13
Histologic features The demonstration of uric acid crystals in tophi requires alcohol fixation and anhydrous processing because monosodium urate is water soluble (Fig. 13.131).38 In formalin-fixed sections, uric acid crystals appear as amorphous material in the dermis or subcutaneous tissues, surrounded by a marked granulomatous response in which many giant cells are usually evident (Figs 13.132 and 13.133). Urate crystals can sometimes be detected in formalin-fixed tissue by polariscopy of 10-micron-thick, unstained sections from the paraffin block.39 Calcification may be a late complication. In secondarily infected lesions, a neutrophil polymorph infiltrate is sometimes present.40 In alcohol-fixed sections, the deposits are seen to be composed of needle-shaped brown crystals, which lie in bundles and show negative birefringence with polarized light and a first-order red compensator filter (Figs 13.134 and 13.135).41
B
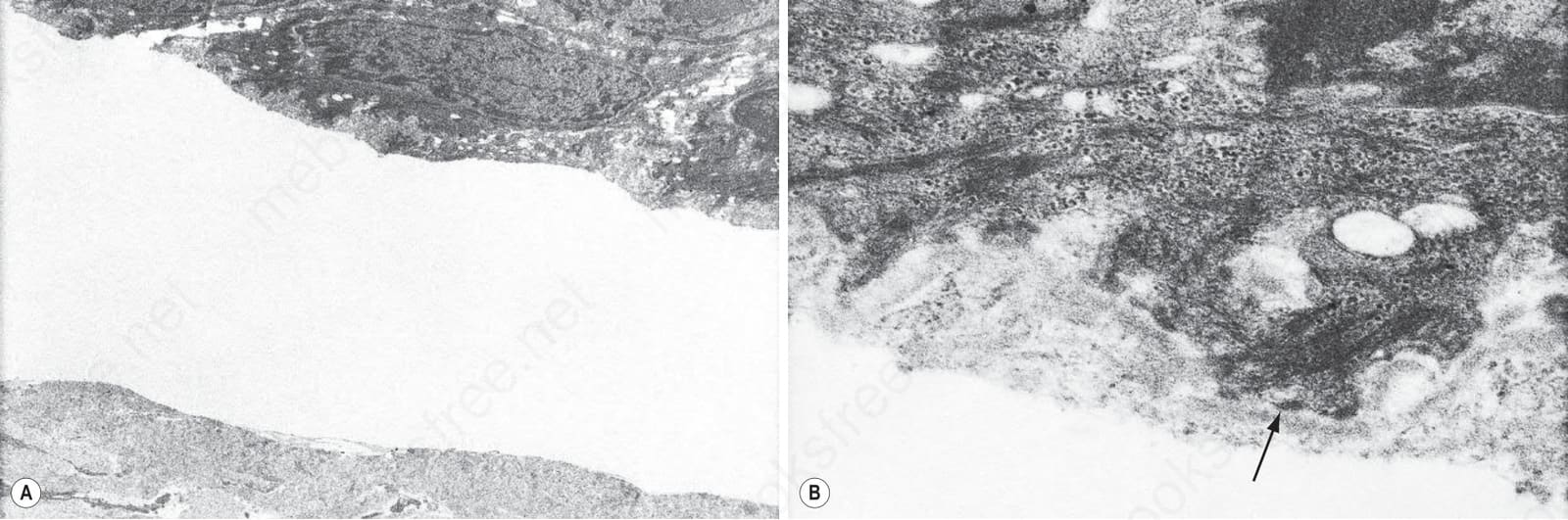
Fig. 13.128 (A, B) Pseudoporphyria: in this example, the blister is located in the superficial papillary dermis deep to the lamina densa (arrowed).
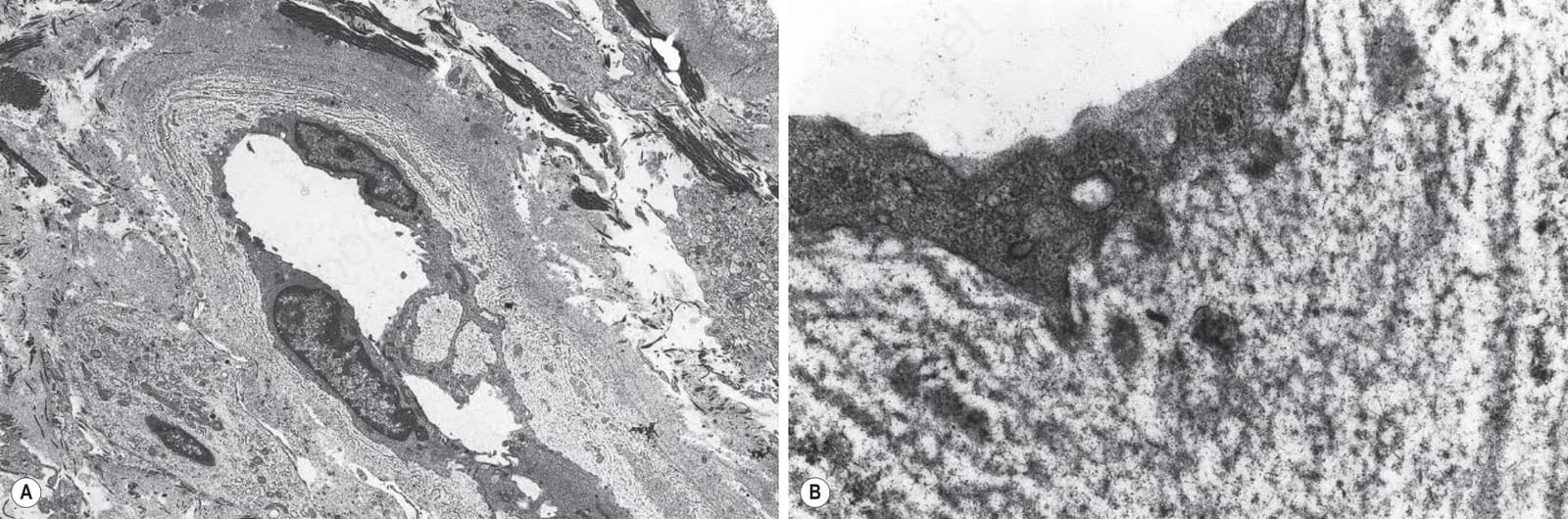
Fig. 13.129 (A, B) Pseudoporphyria: note the striking basement membrane duplication.

Fig. 13.130 Gout: massive deposit on the dorsal aspect of the hand.
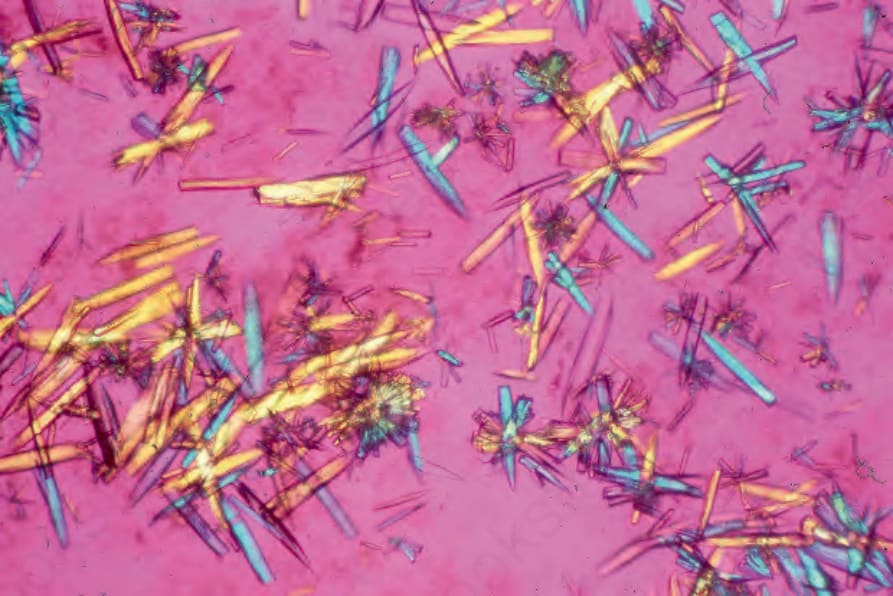
Fig. 13.131 Gout: characteristic needle-shaped crystals. By courtesy of G.T. McKee, MD, Massachusetts General Hospital, Boston, USA.
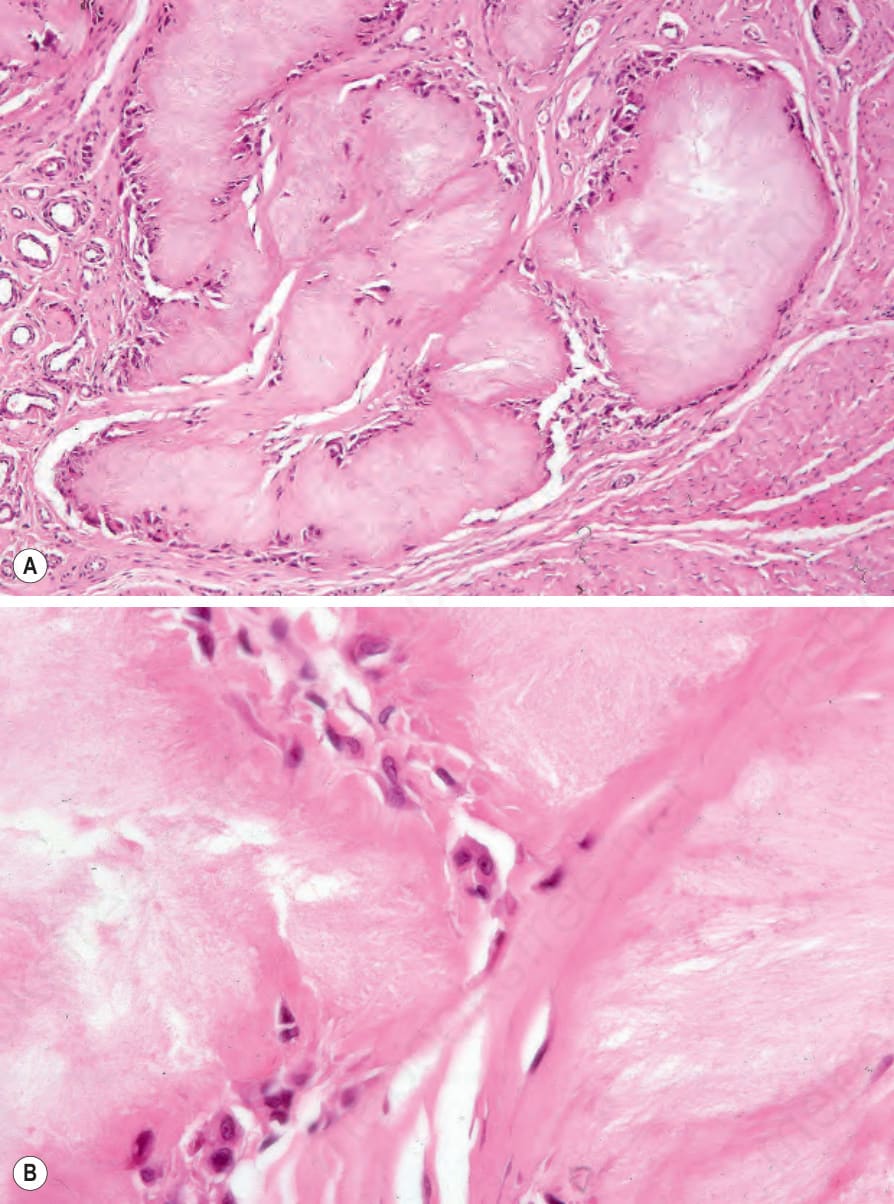
Fig. 13.132 Gout: (A) circumscribed deposits of uric acid are scattered within the dermis, note the accompanying fibrosis; (B) formalin fixation has destroyed the uric acid crystals to leave amorphous eosinophilic material.
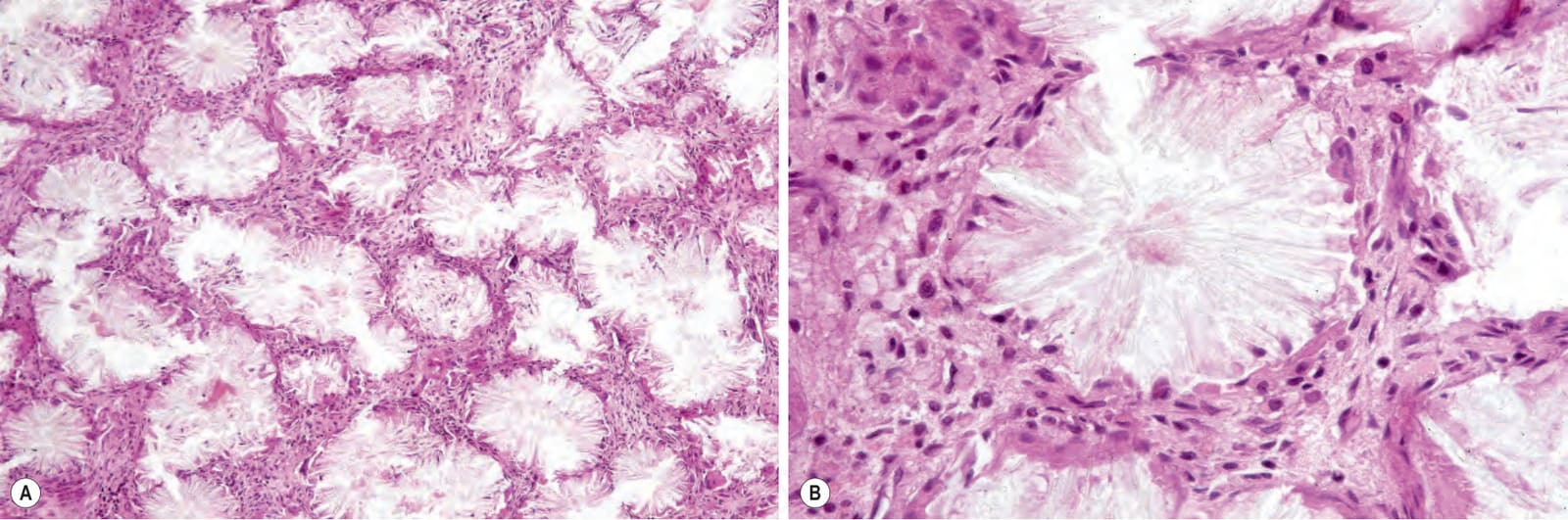
Fig. 13.134 (A, B) Gout: characteristic needle-shaped uric acid crystals are seen in alcohol-fixed and anhydrous processed material.