Juvenile colloid milium
Juvenile colloid milium
Clinical features The juvenile variant, which is exceedingly rare, develops in children before puberty and sometimes has a familial incidence.7–9 Patients present with discrete, or sometimes confluent, papules measuring 0.2–1.5 cm in diameter.8–10 An unusual periocular and perioral linear pattern has been reported.9 Lesions, which are yellow–brown in color, appear translucent and when punctured characteristically express gelatinous material. The underlying tissues often feel indurated. Juvenile colloid milium predominantly affects the face, in particular the cheeks, nose, and around the mouth (Figs 13.69–13.71). Induction of purpura after stroking has been described in both juvenile and adult colloid milium.11 This phenomenon has been attributed to vascular fragility due to infiltration of the blood vessel walls by colloid material. Exceptionally, juvenile colloid milia may present with gingival deposits and ligneous conjunctivitis as a result of infiltration of these tissues by colloid-like material.12–14
Pathogenesis and histologic features Although the etiology remains unknown, in some cases at least, sunlight plays an important role. The pathogenesis, however, shows considerable overlap with macular and lichenoid amyloidosis. Juvenile colloid milium represents a primary degenerative disorder of epidermal keratinocytes, which through the process of apoptosis are transformed into colloid bodies within the superficial dermis.
The initial change is one of filamentous transformation whereby the relatively straight electron-dense keratin filaments are converted into shortened, curved 8–10 nm filaments arranged in weaved or whorled fascicles (Fig. 13.72).10 Occasionally, both types of filament may be identified simultaneously within the cytoplasm of basal keratinocytes. With progression, filamentous transformation comes to affect the entire cell, and nuclear, cytoplasmic, and desmosomal remnants may be identified within the filamentous mass (Fig. 13.73). Residual desmosomes are sometimes present around the border of the colloid deposit. Finally, the apoptotic cell is extruded into the adjacent dermis. In addition to the transformed filaments characteristic of all cytoid bodies, amyloid filaments have also been identified in juvenile colloid milium, thereby prompting the authors to classify this entity along with other amyloid-K dermatoses.3 Positive labeling of the deposits for epidermal keratin gives support to this hypothesis.3,15
Juvenile colloid milium has also been shown by direct immunofluorescence to be accompanied by immunoglobulin, complement, and fibrin
deposits.8 Whether this represents an autoimmune-mediated reaction as is seen in macular-lichenoid amyloidosis or a secondary non-specific reactive phenomenon has yet to be determined.
Histologically, the deposits are present in the superficial dermis where they impinge on the overlying and often somewhat frayed epidermis (Figs 13.74–13.77). The colloid is composed of eosinophilic amorphous aggregates, often showing a fractured appearance. The overlying epithelium shows prominent cytoid bodies, while laterally, acanthosis associated with downward and inward growth results in cuffing or even encirclement of
584 Degenerative and metabolic diseases
the colloid islands by an epidermal collarette.3 An admixture of fibroblasts and mast cells may be evident and pigmentary incontinence is sometimes present. Juvenile colloid milium is histochemically indistinguishable from amyloid: it is diastase-resistant, PAS positive, thioflavine-T positive, and shows positive staining with Congo red with apple-green birefringence.
may be skin-colored to brown.3,16 Adult colloid milium affects fair-skinned patients and follows excessive sun exposure. This has been dramatically illustrated in patients whose lesions are limited to sun-exposed areas of the body.17,18 Adult colloid milium has also been reported following the excessive use of cosmetic ultraviolet A (UVA) sunbed exposure.19 A rare association with multiple myeloma has been described.20 A further report described a patient who developed lesions of adult colloid milia in areas exposed to mineral oils.21 A single case has also been described in a patient with beta thalassemia major.22 Rare cases of pigmented colloid milium have been documented as a consequence of exogenous ochronosis due to bleaching creams and fertilizers.1,16

Fig. 13.69 Juvenile colloid milium: there is papular thickening of the skin, particularly involving the cheeks, nose, and forehead. By courtesy of S. Handfield-Jones, MD, Institute of Dermatology, London, UK.
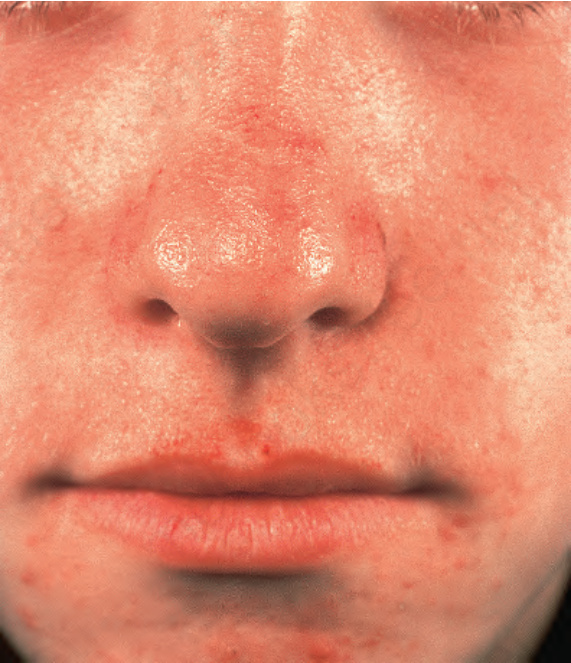
Fig. 13.70 Juvenile colloid milium: this less severely affected child shows typical yellow– brown translucent papules on the nose and upper lip. By courtesy of S. Handfield- Jones, MD, Institute of Dermatology, London, UK.

Fig. 13.71 Juvenile colloid milium: close-up view from the brother of the patient shown in Fig. 13.70. By courtesy of S. Handfield-Jones, MD, Institute of Dermatology, London, UK.
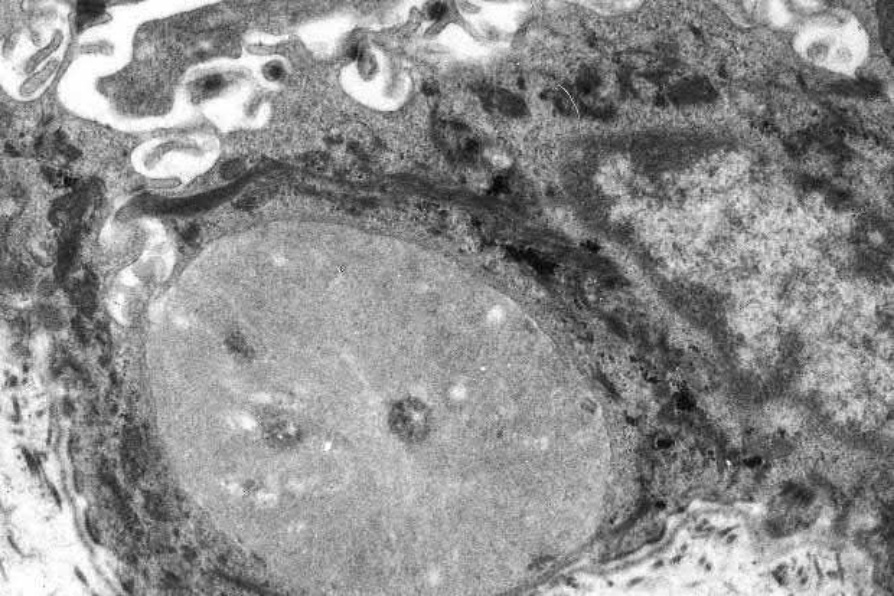
Fig. 13.72 Juvenile colloid milium: this shows an apoptotic keratinocyte, the cytoplasm of which is filled with fascicles of pale-staining filaments that contrast strikingly with adjacent tonofilaments.
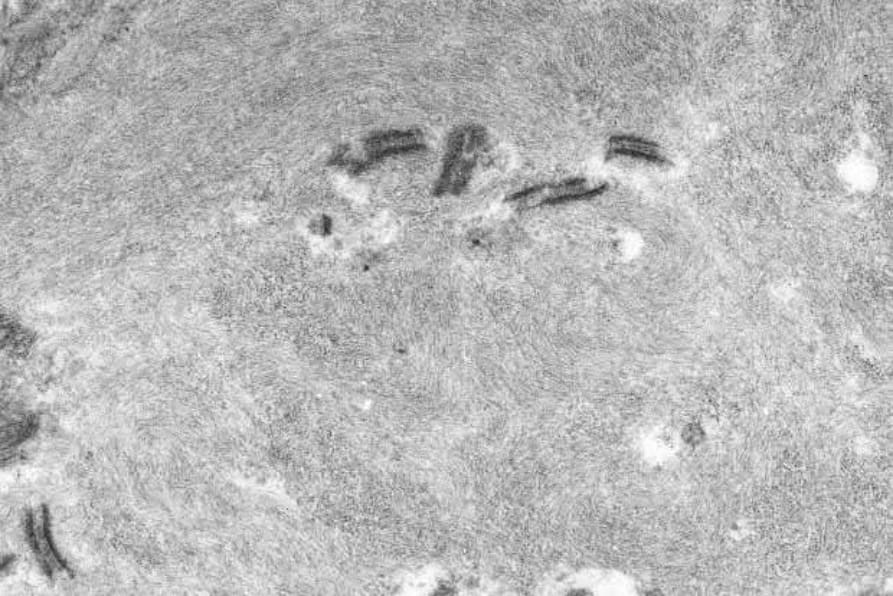
Fig. 13.73 Juvenile colloid milium: internalized desmosomes are evident within this degenerate keratinocyte.
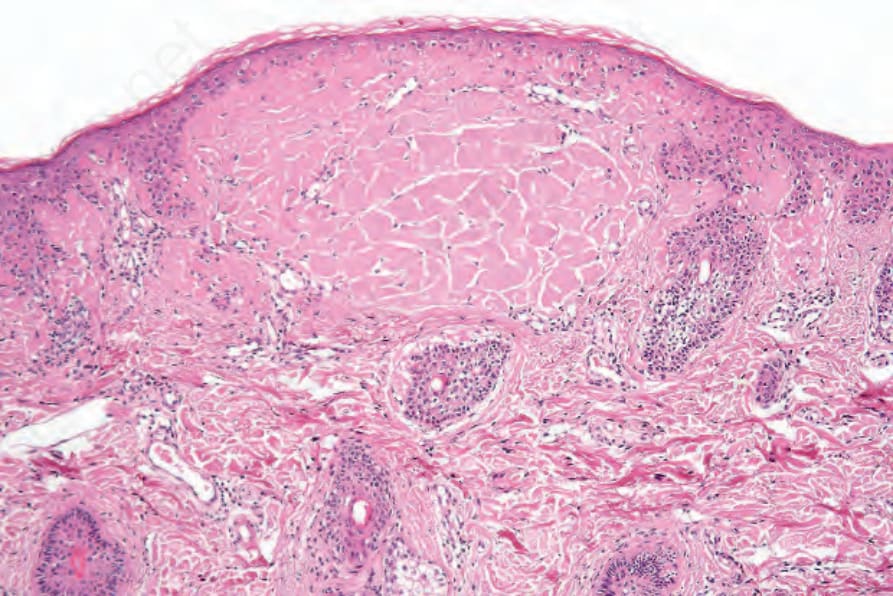
Fig. 13.74 Juvenile colloid milium: the papule consists of an intradermal deposit of eosinophilic material. There is no inflammatory response.