Amyloid elastosis
Amyloid elastosis
Clinical features Amyloid elastosis is a very rare disease, characterized by cutaneous deposits of amyloid in association with elastic fibers of the skin. Only a handful of cases have been reported to date, all in the setting of systemic amyloidosis, except for one in the setting of primary cutaneous amyloidosis.1–7 The clinical manifestations are variable. Most have skin-colored to yellow cobblestoned papules and plaques. Some patients had a pseudoxanthoma-like lesions on the neck and/or intertriginous areas.1,2,3,6 One patient had widespread skin-colored papules and a whitish cobblestone plaque around the urethral meatus.4 Some patients had cordlike thickening of superficial blood vessels, livedo reticularis-like changes on the trunk, Raynaud phenomenon, venous and arterial thrombosis, and the nephrotic syndrome.1,2 The patient with primary cutaneous amyloidosis presented a plaque with prominent skin folds and peripheral erythema involving his left axilla.7 The causes of the systemic amyloidosis included lambda light chain paraprotein and myeloma.2–6
Histologic features Amyloid is seen in the dermis, around adnexal structures, surrounding elastic fibers, sometimes forming small globules, and in blood vessel walls, together with striking deposits in the dermal, subcutaneous, and serosal elastic tissue.1–3,7
Primary localized cutaneous amyloidosis, lichen and macular types
Clinical features Lichen and macular amyloidoses (skin-limited amyloidoses) represent different manifestations of the same process and both entities may coexist (biphasic amyloidosis) or one may transform into the other.1–4 A large study of primary localized cutaneous amyloidosis found that 67% of cases represented lichen amyloidosis, 8% macular amyloidosis, and 25% biphasic variants.5 Although most cases are sporadic, up to 10% of patients demonstrate an autosomal dominant inheritance pattern (see familial primary cutaneous amyloidosis).6,7
usually moderately pruritic (Fig. 13.50). More commonly, however, macular amyloid appears as small, 2–3 mm diameter lesions or else as confluent macular foci, which sometimes have superimposed micropapules.8 Lesions sometimes follow Blaschko lines, resembling incontinentia pigmenti.11,12 Exceptionally, widespread diffuse pigmentation occurs.13 Predominantly hypopigmented macules have been described, mimicking guttate morphea and vitiligo.14
Macular primary cutaneous amyloidosis. This is most commonly seen in patients from the Middle East, Asia, and Central and South America.1,8 It affects females more often than males (3 : 1), is seen in younger age groups, and is usually a chronic condition.9,10 Patients present with a macular, dark brown or grayish, symmetrical pigmentation, which occurs most frequently on the upper chest and back, although the extremities and face may also be affected (Fig. 13.49).1,9 The lesions sometimes have a very characteristic reticulated or rippled appearance, which can be quite subtle, and they are
Papular or lichen amyloidosis. In papular or lichen amyloidosis, discrete papules and/or plaques occur, which are often scaly, persistent, and pigmented (Fig. 13.51). They are usually severely pruritic. Excoriations, lichenification, and nodular prurigo-like lesions due to chronic scratching are sometimes evident.10 Lesions are especially common on the front of the shins and extensor aspect of the forearms (Figs 13.52 and 13.53).15,16 The calves, ankles, dorsa of the feet, thighs, and trunk may also be affected.17–19 Presentation is most often in young adults. The sex incidence is equal.1,20 Lichen amyloidosis shows a predilection for the Chinese race and familial cases have been recorded.18,19 An association with Epstein-Barr virus infection has been reported in a single case, but this was not confirmed in a larger study.21
Association with systemic disease is probably coincidental but there have been a number of cases described with progressive systemic sclerosis.22,23
578 Degenerative and metabolic diseases
Other primary cutaneous amyloidoses. These include anosacral and poikilodermatous variants:
• Anosacral amyloidosis presents as scaly hyperpigmented macules and lichenoid papules spreading out from the perianal skin.24,25 It is seen in patients from Japan and China and is very rare. The disease may present early in life and its cause has not been established, although a relationship to keratinocyte apoptosis has been suggested.25 Clinically, lesions can be confused with lichen simplex chronicus, a dermatophyte infection or even postinflammatory hyperpigmentation.
• Poikiloderma-like cutaneous amyloidosis is an extremely rare manifestation of localized cutaneous amyloidosis.26,27 Patients present with poikilodermatous skin lesions and lichenoid papules. It may be associated with photosensitivity, short stature, and palmoplantar keratoderma.27 Blisters are rarely seen. The condition presents early in life or in young adults. Confusion with other conditions associated with poikiloderma, including poikiloderma atrophicans vasculare, is possible. A single case of poikiloderma-like amyloidosis associated with lichen, dyschromic, and bullous variants has been described.28
Pathogenesis and histologic features Chronic irritation to the skin has been proposed as the cause of amyloid deposition in the macular and lichenoid variants, although this has never been proven.29,30 The documentation, however, of friction amyloidosis due to nylon brush skin massage and towels does offer some support to this hypothesis.31–34 It may be that chronic trauma in a susceptible or ‘primed’ individual may be associated with an increased risk of developing cutaneous amyloidosis. It has been suggested that amyloid deposition in lichen amyloidosis is a consequence of scratching, as pruritus tends to be the presenting symptom even before amyloid is detected in skin biopsies.35 The chronic damage to the epidermis induces apoptosis of keratinocytes and this leads to amyloid deposition in the papillary dermis. A similar mechanism has been proposed in notalgia paresthetica. This is a condition characterized by pruritus, a burning sensation, and paresthesia or hyperesthesia in an area of the back between dermatomes D2 and D6.36,37 The resultant irritation and scratching induce cutaneous hyperpigmentation and amyloid deposition. It has even been suggested that the cutaneous amyloidosis observed in patients with multiple endocrine neoplasia type 2A is secondary to notalgia paresthetica (see below).38
In both variants the amyloid is deposited high in the papillary dermis, often immediately adjacent to the epidermis.8,9,17,39,40
In the macular type, the amount of amyloid present is often very small and focally distributed. It frequently has a faceted appearance (Figs 13.54–13.56).2,9 Special stains and/or immunocytochemistry are sometimes necessary as the deposits can easily be missed. Intraepidermal cytoid bodies
579 The amyloidoses
When special stains fail to demonstrate the presence of amyloid, ultrastructural studies are usually successful in detecting the presence of the protein.41
are present in about 33% of cases.8 Typically, there is associated pigmentary incontinence, but only minor epidermal changes of hyperkeratosis and acanthosis are generally evident. Melanin pigment may be present in the stratum corneum. A slight perivascular chronic inflammatory cell infiltrate is often found in the superficial dermis.9 Mild vacuolar interface alteration can be present.14
In papular or lichen amyloidosis, the histopathological changes are similar and cannot be reliably distinguished from those of the macular variant, except that the quantities deposited are greater and there is often more marked epidermal acanthosis, hypergranulosis, and hyperkeratosis. Basal cell hydropic degeneration may be evident and colloid bodies are usually visible (Figs 13.57 and 13.58).1 Satellite cell necrosis is sometimes a feature.1 A superficial perivascular chronic inflammatory cell infiltrate is typically present.
In contrast to skin involvement in systemic disease, blood vessel deposits are not a feature of primary cutaneous localized lesions.
In earlier literature it was postulated that the amyloid might have been derived from mast cells or fibroblasts. The application of newer technology, however, has shown that it is indisputably of keratinocyte derivation, and amyloid deposits have been shown to contain disulfide bonds and bullous pemphigoid antigen.8 Numerous recent publications confirm the presence of epidermal keratin in the deposits in both macular and lichenoid forms using monoclonal immunocytochemistry.3,42–50 The amyloid of the skin-limited variants, so-called amyloid-K, has been shown to contain 50 and 67 kD keratin filaments.29,49 Apolipoprotein E, one of the proteins found in the amyloid plaque of Alzheimer disease and in systemic amyloidosis, has also been demonstrated in the amyloid present in localized cutaneous amyloidosis.51,52 Electron microscopic studies have provided further evidence that amyloid-K is of keratinocyte origin by showing tonofilament filamentous (apoptotic) degeneration into amyloid filaments both within the epidermis
580 Degenerative and metabolic diseases
K
bodies show ultrastructural differences. Amyloid fibrils are irregularly distributed whereas the filaments in cytoid bodies are arranged in bundles or whorls.54
A
It is postulated that the development of localized cutaneous amyloidosis is dependent upon mild chronic trauma resulting in excessive production of cytoid bodies and their subsequent conversion into amyloid deposits. It would seem that despite a normal humoral response as shown by the presence of IgM and IgG in association with complement fixation, the normal cellular response whereby apoptotic keratinocytes are removed is lacking.29,55–57
Amyloid deposits are frequently found in intimate association with dermal elastic fibers and the deposits in macular amyloidosis have been shown to contain fibrillin.58 Whether this is of pathogenetic significance or is merely a secondary phenomenon is uncertain.
The apoptotic theory of amyloidogenesis in the cutaneous variants has, however, been challenged. On the basis of finding amyloid deposits immediately below the basal keratinocyte, separating its cell membrane from the lamina densa in the absence of any evidence of filamentous degeneration, it has been suggested that cutaneous amyloid deposits may also be a direct secretory product of keratinocytes.59,60 It could be that both mechanisms are in operation.
B

Fig. 13.49 Macular amyloid: hyperpigmented lesion in a characteristic site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.50 Macular amyloid: close-up view of a lesion showing the typically rippled appearance. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.51 Lichen amyloidosis: pigmented papules on the chest. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.52 Lichen amyloidosis: scaly lichenoid papules on the shin. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
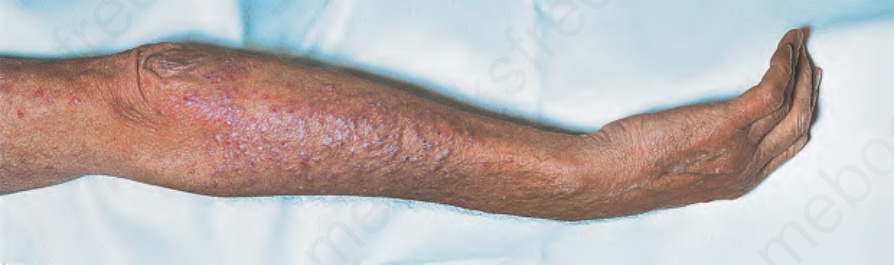
Fig. 13.53 Lichen amyloidosis: grouped, erythematoviolaceous papules, with a lichenoid surface and showing excoriations in some areas. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
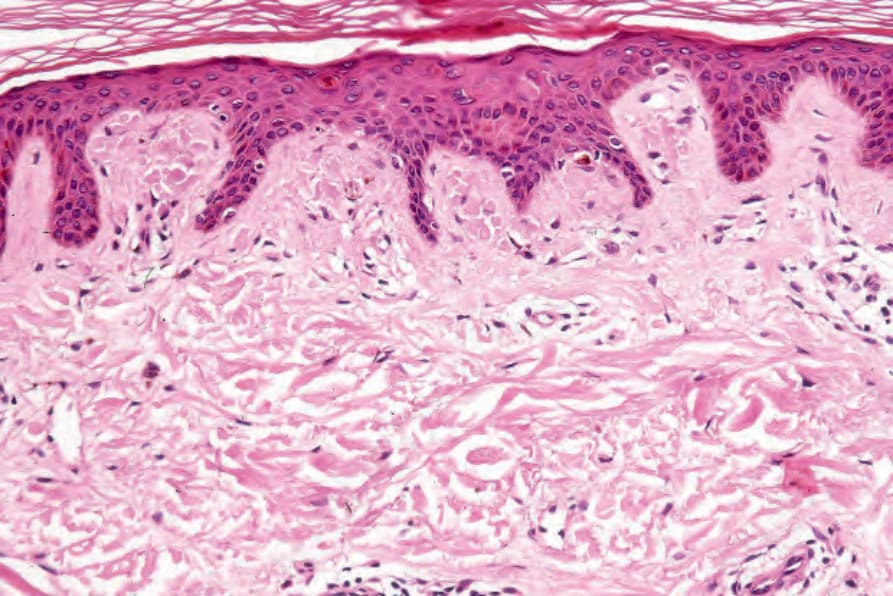
Fig. 13.54 Macular amyloidosis: typical eosinophilic faceted deposits are present in the papillary dermis.
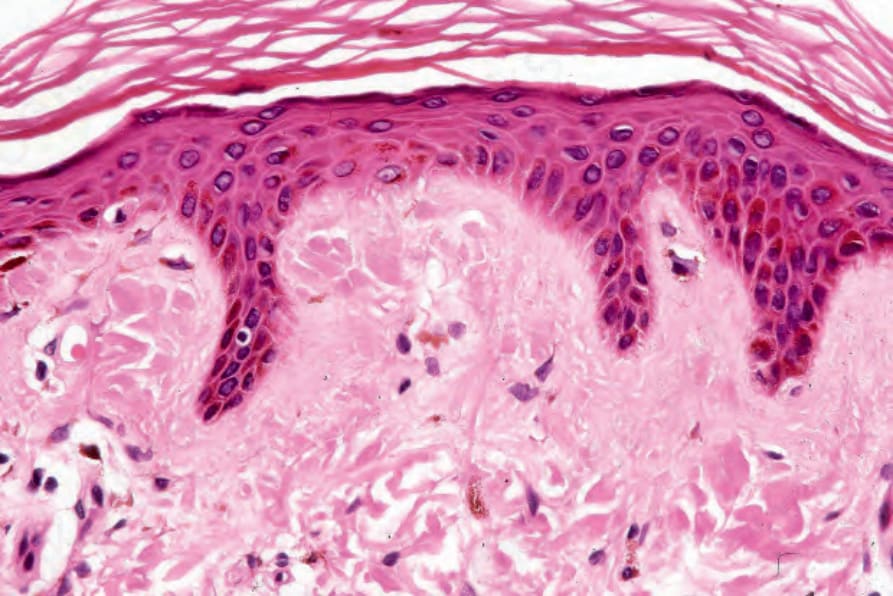
Fig. 13.55 Macular amyloidosis: close-up view of faceted deposits.
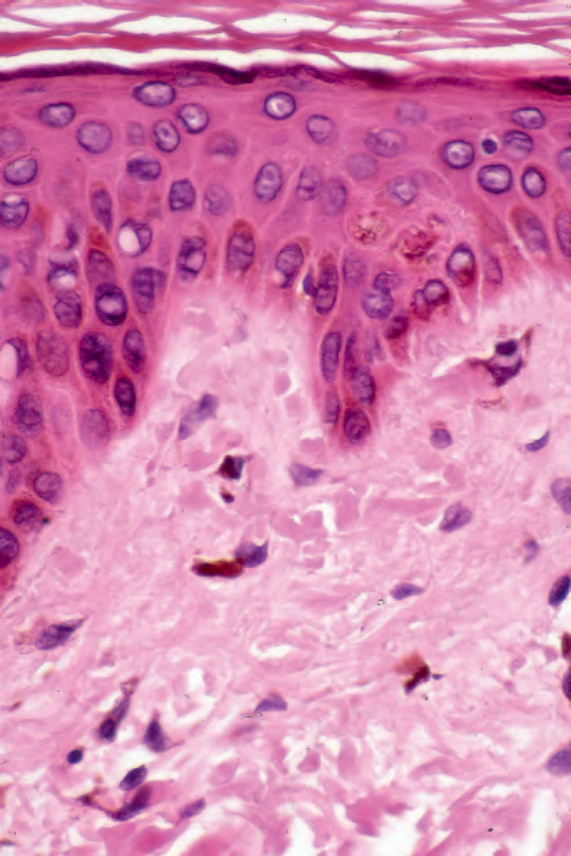
Fig. 13.56 Macular amyloidosis: pigmentary incontinence is typically present.
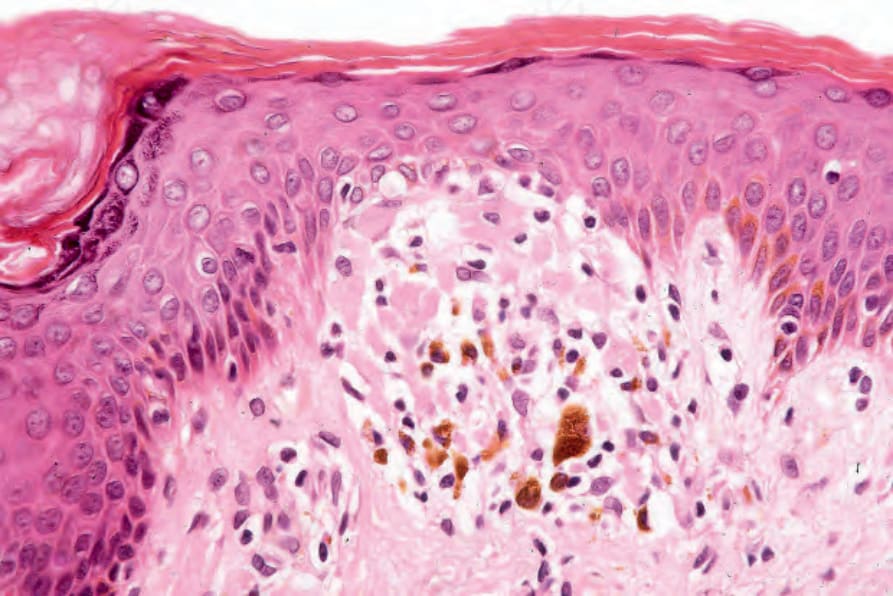
Fig. 13.57 Lichen amyloidosis: there is hyperkeratosis, acanthosis, and basal cell hydropic degeneration; small eosinophilic globules are present in the papillary dermis. A mild chronic inflammatory cell infiltrate is present. Note the pigmentary incontinence.
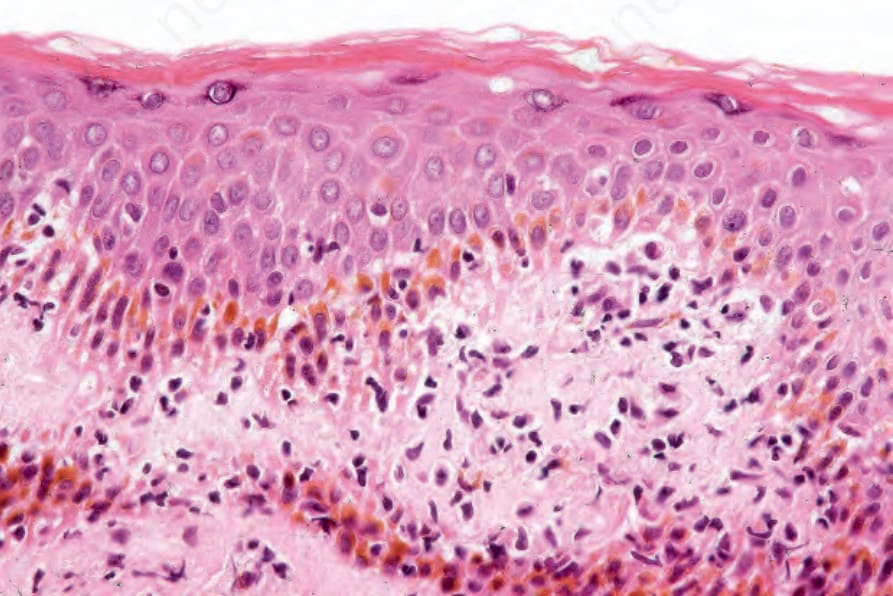
Fig. 13.58 Lichen amyloidosis: in this view, there is interface change and a lymphocytic infiltrate.
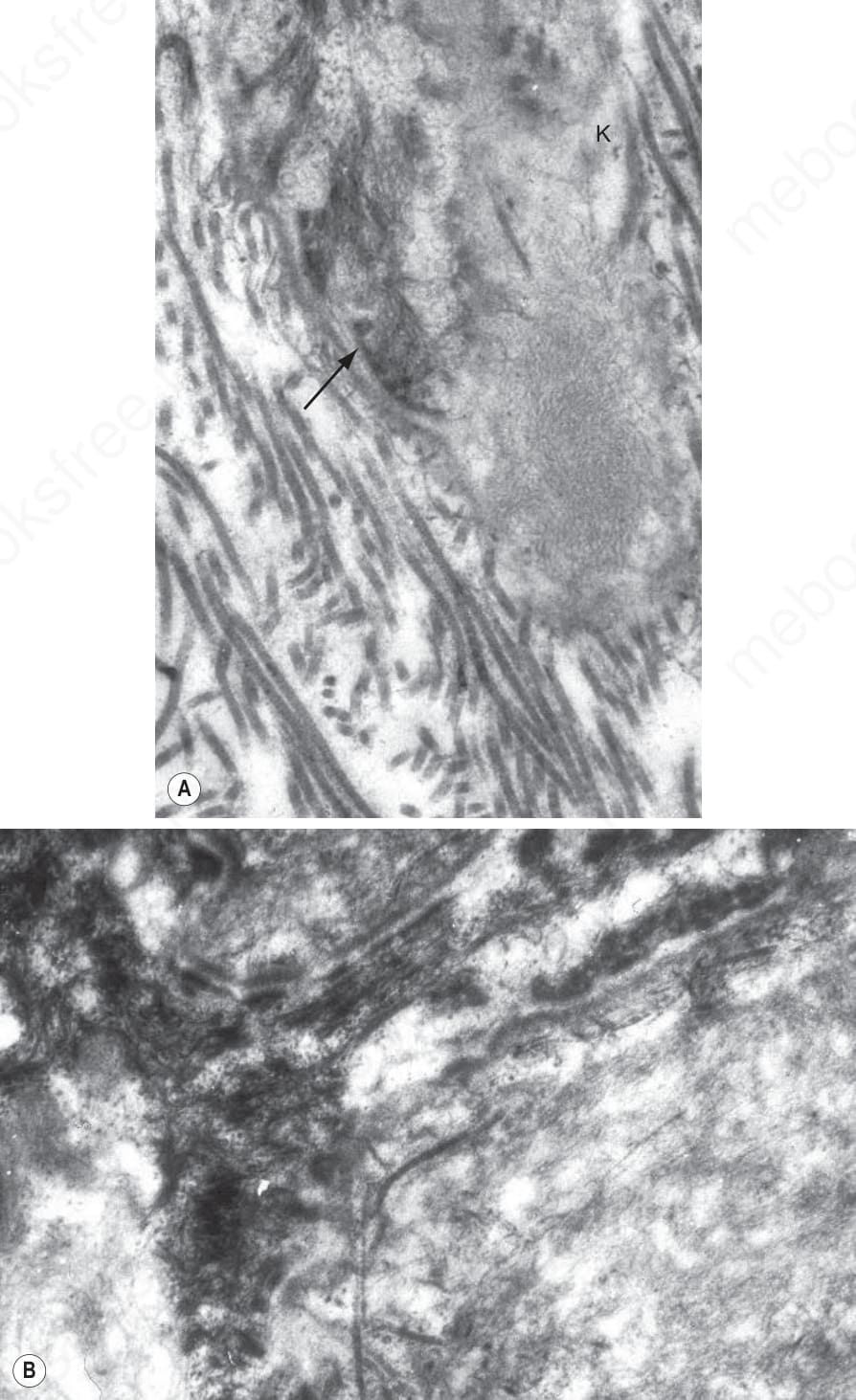
Fig. 13.59 Lichen amyloidosis: (A) early filamentous degeneration is seen in this basal keratinocyte (K), lamina densa is arrowed; (B) compare the organized appearance of the tonofilaments with the haphazardly orientated amyloid immediately adjacent to the lamina densa.
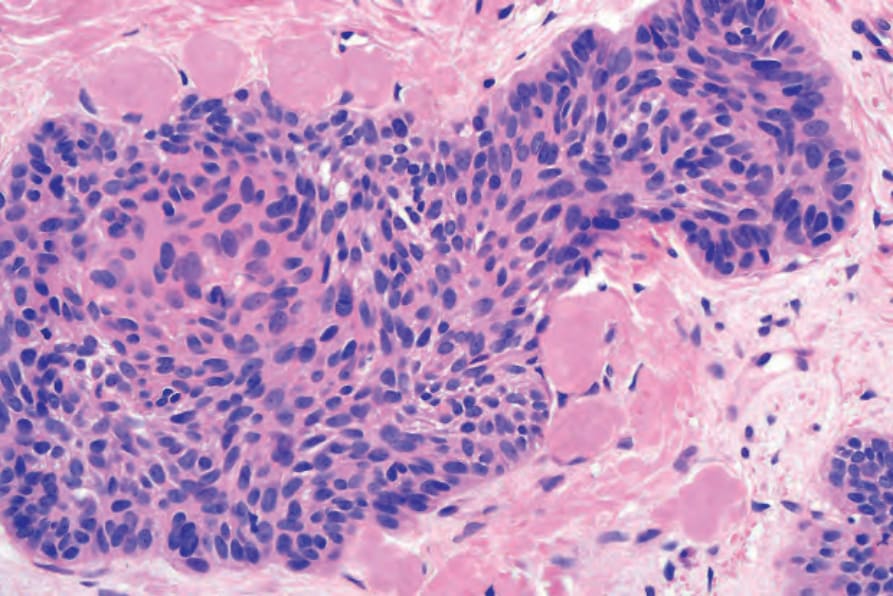
Fig. 13.60 Tumor-associated amyloid: amyloid deposits in a basal cell carcinoma.