Planar xanthomata
Planar xanthomata
Clinical features Planar xanthomata are typically soft yellow dermal macules or plaques that occur most frequently around the eyes, where they are known as xanthelasmata (Fig. 13.18).1,2 About 50% of patients with xanthelasmata have associated hyperlipidemia (hypercholesterolemia or HPL type III) which is often accompanied by a cholesterol corneal arcus.3–5 Many of those who
566 Degenerative and metabolic diseases
A
A
B
B
appear biochemically normal on routine testing, however, are shown to have subtle abnormalities of lipid metabolism on more detailed analysis.6 There is a particularly increased risk of coronary artery atherosclerosis in younger patients.1 When very extensive (diffuse or generalized plane xanthomatosis) and associated with orange–yellow planar xanthomata around the head and neck, and occasionally the upper trunk and arms, there may be an associated systemic disorder such as multiple myeloma with paraproteinemia, cryoglobulinemia, benign paraproteinemia or, less commonly, leukemia and rheumatoid arthritis (necrobiotic xanthogranuloma) (Fig. 13.19).1,3,7–14 More exceptional associations include idiopathic Bence Jones proteinuria, Sézary syndrome, Castleman disease, relapsing polychondritis, acquired palmoplantar keratoderma, adult T-cell leukemia/lymphoma, and Takayasu disease.15–21 A patient with monoclonal gammopathy and cutaneous lesions with features of both plane xanthoma and amyloidosis has been documented.22 The latter case was also associated with myeloma.
In cases of myeloma and plane xanthoma, it has been demonstrated that complexes form between serum lipoproteins and paraprotein, suggesting that this interaction may induce a hyperlipidemia and xanthoma formation.23,24 The serum lipid levels of patients with diffuse plane xanthomata are normal or raised. Plane xanthomata may present in the gingiva and, in this location, are usually associated with hyperlipidemia.25 An exceptional case has been described in an infant presenting with normolipemic papular and nodular lesions progressing to plane xanthomata and resulting
567 The hyperlipidemias
in spontaneous resolution.26 Diffuse plane normolipemic xanthomata with mucosal and conjunctival involvement and aortic valve xanthomatosis may occur exceptionally.27 Lesions have been reported that clinically resembled plane xanthomata in a patient with systemic lupus erythematosus but histologically showed degeneration of collagen bundles with secondary fat deposition.28
Intertriginous xanthomata seen in patients with raised LDLs and pathognomonic of homozygous familial hypercholesterolemia present as yellow papules and plaques, often with a cobblestone appearance. These occur in the finger webspaces and to a lesser extent in the axillae and antecubital and popliteal fossae.29 They have a particularly high association with early and severe atherosclerosis. Intertriginous xanthomata may also rarely be seen in heterozygous familial hypercholesterolemia.30
Planar xanthomata presenting as yellow-orange macules in the skin creases of the palm and fingers (xanthoma striatum palmare) are diagnostic of familial dysbetalipoproteinemia (HPL type III, broad beta disease) (Fig. 13.20), which is due to an abnormality of the apoprotein ApoE (homozygous ApoE2/E2).1,2,31 This results in impaired uptake of lipoprotein remnant particles by the liver and macrophages with resultant HPL and increased atherogenesis.30 Interestingly, the tendency to familial dysbetalipoproteinemia is present in 1% of the population, but a second lipid abnormality appears to be necessary to induce symptoms.30
Plane xanthomata of cholestasis, for example due to primary biliary cirrhosis and biliary atresia, present as well-demarcated, beige–orange plaques that are particularly found on the hands and feet, but may occur elsewhere.2 They can also develop in patients with diabetes mellitus and have been described in the setting of cholestasis resulting from chronic graft-versushost disease.32
Planar xanthomata have also been described as a feature of HDL deficiency.33
Histologic features In planar xanthomata, the characteristic lipid-laden foam cells are situated within the superficial dermis (Figs 13.21–13.23). There is minimal fibrosis. In rare cases, the histology may overlap with that of necrobiotic xanthogranuloma.34.
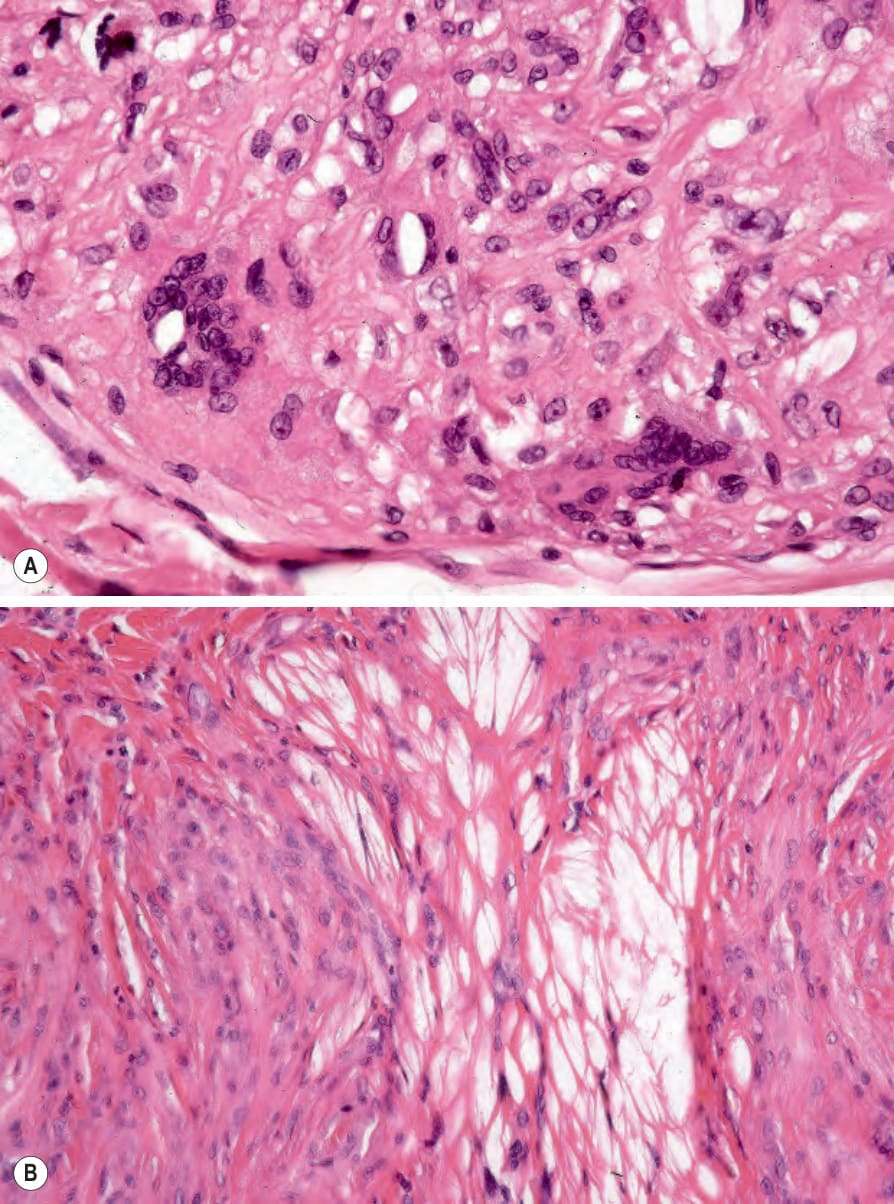
Fig. 13.17 (A, B) Tuberous xanthoma: in addition to xanthoma cells, occasionally there are foreign body giant cells containing cholesterol clefts. The lipid has been dissolved out during processing.
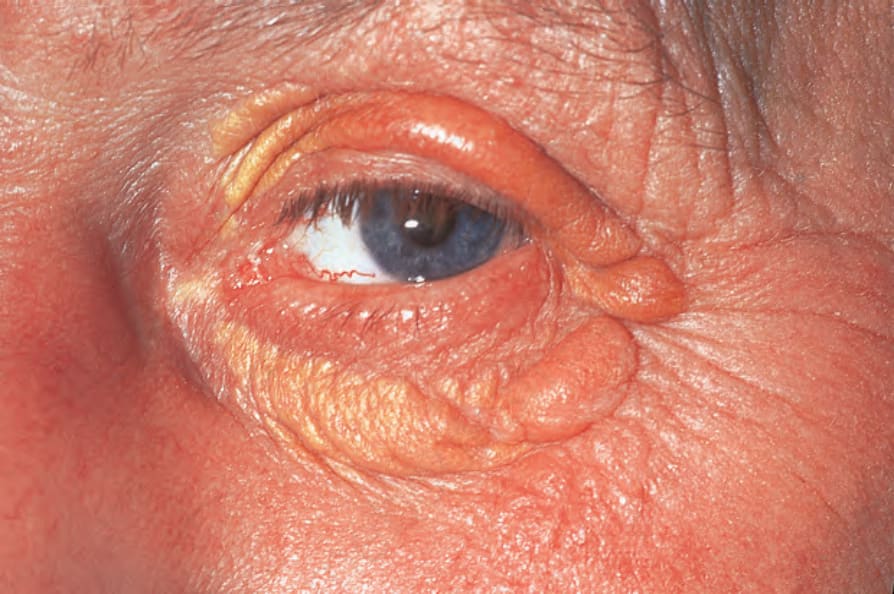
Fig. 13.18 Xanthelasmata: note the yellow, periorbital plaques. These are a common manifestation of hypercholesterolemia. By courtesy of the Institute of Dermatology, London, UK.

Fig. 13.19 Planar xanthoma: (A) widely distributed lesions over the forehead, eyelids, and cheeks; (B) extensive yellow plaques on the scalp. This appearance should prompt a search for an associated paraproteinemia. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 13.20 Planar xanthoma: palmar lesions presenting as discrete macules with accentuation in the skin creases. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
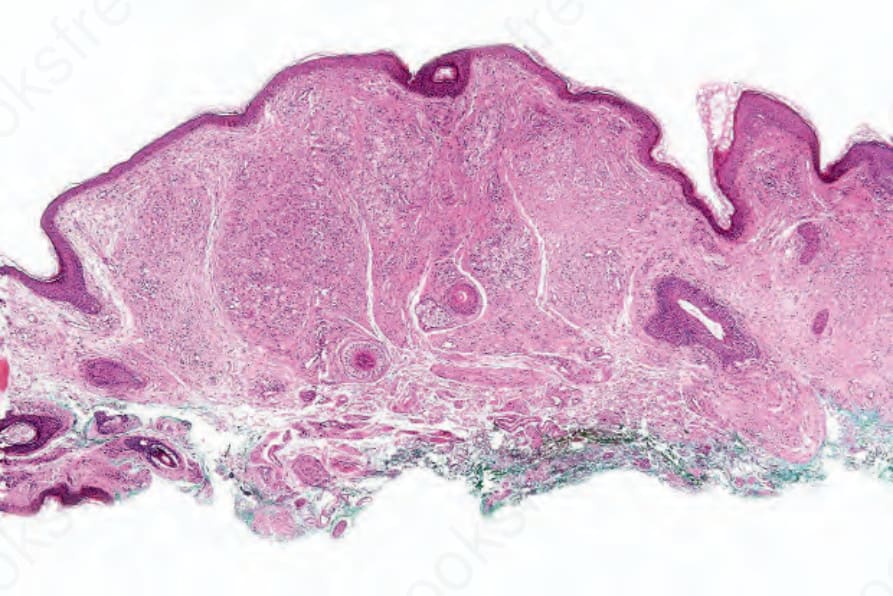
Fig. 13.21 Planar xanthoma: a dense infiltrate is present in the upper dermis.
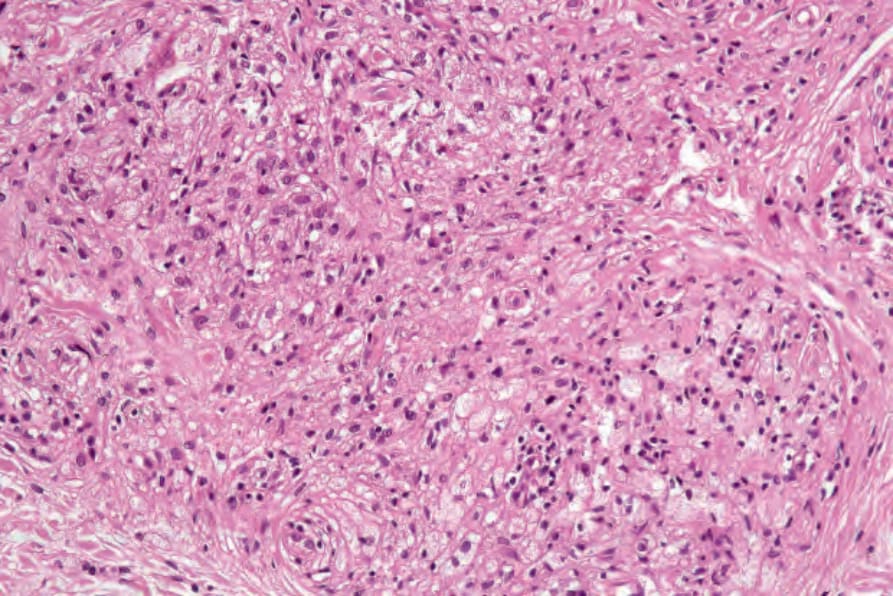
Fig. 13.22 Planar xanthoma: there is an admixture on nonlipidized and lipidized histiocytes.