The hyperlipidemias
The hyperlipidemias
The hyperlipidemias may present as cutaneous xanthomata, which are localized aggregates of histiocytes containing accumulated lipid (primarily free and esterified cholesterol), in the form of five main clinical types:
• eruptive,
• tendinous,
• tuberous,
• planar,
• disseminated.1
The last, xanthoma disseminatum, in which serum lipid levels are normal, is discussed in Chapter 29 (see xanthogranuloma). Xanthoma cells are histiocytes and express CD4, CD11c, CD14b, CD68 and CD163 in addition to human leukocyte antigen (HLA) class II antigens.2,3
The plasma lipids are composed of triglycerides and cholesterol; these are insoluble and their transport is facilitated by their aggregation into lipoproteins. The latter are macromolecular complexes composed of an outer shell of hydrophilic phospholipids, nonesterified cholesterol, and apo(lipo) proteins, which emulsify the associated hydrophobic core of triglycerides and cholesterol ester.5 There are a large number of apoproteins, with variable structure and function (e.g., ApoB-48, which is required for the secretion of chylomicrons into the thoracic duct).4 In addition to giving structure to the lipoprotein, apoproteins also represent ligands for specific receptors (e.g., ApoE is a ligand for liver chylomicron receptors). They also act as cofactors for a number of lipid-modifying enzymes (e.g., ApoCII activates lipoprotein lipase).6 Lipoprotein metabolism, which is summarized in Fig. 13.1, involves both exogenous (dietary) and endogenous pathways.7 For more detailed information the reader is particularly referred to references 1 and 7.
Hyperlipidemias may be primary, or secondary to conditions such as diabetes mellitus, obesity, pancreatitis, renal disease (the nephrotic syndrome or chronic renal failure), hypothyroidism, alcohol consumption, pregnancy, cholestatic liver disease (e.g., primary biliary cirrhosis), and paraproteinemias. Drug-induced hyperlipidemia also occurs as a result of administration of estrogens, corticosteroids, or 13-cis-retinoic acid. It is often associated with serious, potentially life-threatening disorders, such as atherosclerosis (low-density lipoproteins) and pancreatitis (hypertriglyceridemia).4
The presence of xanthomata commonly represents a cutaneous manifestation of systemic disease, and their recognition should therefore be followed by exhaustive investigations to exclude the latter (Table 13.1).2,5 Although not a hard and fast rule, xanthoma morphology and distribution can sometimes point toward specific hyperlipidemia variants.
The classification of hyperlipidemias is based upon the electrophoretic separation, on paper or agarose gel, of abnormal quantities of lipoprotein in the plasma (Fig. 13.2). There are seven main classes of lipoprotein, with differing electrophoretic mobilities:
• chylomicrons, which are composed predominantly of exogenous triglycerides produced by small intestinal mucosal epithelium in response to dietary lipid,
• very low density (pre-beta) lipoproteins (VLDL) of hepatic derivation, which are particularly involved in the transportation of endogenous triglyceride,
• intermediate density lipoproteins (IDL), which are thought to be VLDL remnants,
560 Degenerative and metabolic diseases
liver LDL receptor
chylomicron remnant receptor
intestine
extrahepatic tissues
7
LDL receptor
7
4
6a
1
chylomicron chylomicron remnant
VLDL LDL VLDL remnant
B48
B48
A
3
E E CII
2
capillary
B100
B100
B100
E E
6b
CII
5
lipoprotein lipase lipoprotein lipase
adipose and muscle tissue
Hyperlipidemic xanthomatoses: disorders characterized by elevated plasma triglycerides or cholesterol
Normolipidemic xanthomatoses: disorders characterized by normal plasma triglycerides and cholesterol
Primary hyperlipoproteinemias
Elevated plasma triglycerides lipoprotein lipase deficiency familial hyperlipoproteinemia, type V familial hypertriglyceridemia Elevated plasma triglycerides and cholesterol familial dysbetalipoproteinemia, type III Elevated plasma cholesterol familial hypercholesterolemia
Disorders characterized by altered lipoprotein content or structure
Accumulation of unusual sterols in LDL cerebrotendinous xanthomatosis (cholestanol) sitosterolemia (sitosterol, campesterol, stigmasterol, etc.) Deficiency of HDL plantar and buccal mucosal xanthomas diffuse plane xanthomas Normocholesterolemic dysbetalipoproteinemia tuberous xanthelasmas Hyperapobetalipoproteinemia tendon xanthomas xanthelasmas
Secondary hyperlipoproteinemias
Elevated plasma triglycerides diabetes mellitus drug-induced chylomicronemia alcohol estrogens retinoids hypothyroidism nephrotic syndrome type I glycogen storage disease (von Gierke disease) Elevated plasma cholesterol hepatic cholestasis primary biliary cirrhosis biliary atresia hypothyroidism dysglobulinemias or paraproteinemias multiple myeloma
Disorders associated with antibodies directed against lipoprotein components
States with no demonstrated lipoprotein abnormalities
Multiple myeloma Other paraproteinemias
Underlying lymphoproliferative disease multiple myeloma cryoglobulinemia Waldenström macroglobulinemia leukemia lymphoma other Xanthomatosis antedated by local tissue alterations normolipemic eruptive xanthomas (after erythema) xanthelasmas and planar xanthomas (after erythroderma) Verruciform xanthomas (in areas of dystrophic epidermolysis bullosa) Other hereditary tendinous and tuberous xanthomas normolipemic tendon and tuberous xanthomas normolipemic subcutaneous xanthomatosis
HDL, high density lipoprotein; LDL, low density lipoprotein. Reprinted from Cruz, P.D., East, C., Bergstresser, P.R. (1988) Journal of the American Academy of Dermatology, 19, 95–111 with permission from the American Academy of Dermatology, Inc.
• low density (beta) lipoproteins (LDL), which are mainly involved in cholesterol transport and derived from IDL or else produced by the liver,
• high density (alpha) lipoproteins (HDL) composed predominantly of lipoprotein and equal quantities of cholesterol and phospholipid,
• high density lipoprotein variant HDL2,1,6
• high density lipoprotein variant HDL3.1,6
The hyperlipidemias are classified into six types according to the lipoprotein anomaly present (Table 13.2). However, it should be noted that each of these six types may result from a variety of pathogeneses, including
561 The hyperlipidemias
those of a known or presumed genetic basis and others that complicate a diverse group of disease processes (secondary hyperlipidemia).8–10 HDLs are not atherogenic.4 Indeed, their function is to remove cholesterol from the tissues and high levels serve to protect against vascular disease.6 Conversely, HDL deficiency (e.g., Tangier disease) is associated with cholesterol accumulation.11
The lipid content of xanthomata is probably mostly derived from the plasma, presumably by lipoprotein (particularly LDL and VLDL) permeation of blood vessel walls with the release of lipid and its subsequent phagocytosis by histiocytes, although localized lipogenesis may also be of importance.11–14 The subgroups and proportions of lipid deposited within xanthomata are similar to those found in atheromatous plaques, raising the possibility of a shared pathogenesis.1
Xanthomata are, however, not always associated with hypercholesterolemia or hyperlipoproteinemia.15 Under such circumstances, they may evolve as a consequence of altered lipoprotein content or structure, represent local tissue changes or develop as a consequence of systemic disease including lymphoma, multiple myeloma, and Waldenström macroglobulinemia.16 Normocholesterolemic xanthomata can therefore arise as a consequence of the accumulation of cholesterol-like substances within histiocytes (e.g., cerebrotendinous xanthomatosis and β-sitosterolemia).
Cerebrotendinous xanthomatosis represents an abnormality of bile acid metabolism inherited in an autosomal recessive pattern.17–19 As a consequence of mitochondrial enzyme sterol 27-hydroxylase deficiency and resultant impaired oxidation of the cholesterol side chain during the production of cholic acid, cholestanol (and cholesterol) accumulates in the tissues, especially the tendons, lungs, and brain. The xanthomata particularly affect the Achilles tendons and the tendons of the knees, elbows, and the interphalangeal joints.20 In addition to tendinous xanthomata, patients develop juvenile cataracts and progressive neurological dysfunction including mental retardation, dementia, pyramidal signs, cerebellar ataxia, spinal cord paresis, and sensory changes due to dysmyelination.19,21,22 Coronary atherosclerosis,
Type Anomaly Primary cause Secondary cause Atherogenesis Xanthoma Associations
I Raised chylomicrons Familial lipoprotein lipase deficiency Apoprotein Cll deficiency
IIA Raised LDL Familial hypercholesterolemia Familial multiple type hyper lipoproteinemia Common hypercholesterolemia
IIB Raised LDL and VLDL
Familial hypercholesterolemia Familial multiple type hyperlipidemia
– – Eruptive Hepatomegaly Pancreatitis Lipemia retinalis Abdominal pain
- Tendinous Xanthelasma Arcus Tuberous (rare)
Hepatoma Porphyria Myxedema Anorexia nervosa Nephrotic syndrome Cushing syndrome
–
- Tendinous Xanthelasma Arcus Tuberous
Nephrotic syndrome Cushing syndrome
–
III Raised IDL Familial dysbetalipoproteinemia Paraproteinemia + Palmar Tendinous Tuberous
IV Raised VLDL Familial multiple type hyperlipidemia Familial hypertriglyceridemia Sporadic hypertriglyceridemia
V Raised chylomicrons and VLDL
Familial multiple type hyperlipoproteinemia Familial lipoprotein lipase deficiency Apoprotein Cll deficiency Familial hypertriglyceridemia Familial type V hyperlipoproteinemia
Diabetes Gout Obesity
- Eruptive Tendinous Tuberous
Diabetes Uremia Paraproteinemia Alcoholism Lipodystrophy Obesity
–
- Eruptive Hepatomegaly Pancreatitis Lipemia retinalis
Diabetes Obesity Pancreatitis
IDL, intermediate density lipoprotein; LDL, low density lipoprotein; VLDL, very low density lipoprotein.
562 Degenerative and metabolic diseases
endocrine abnormalities, and diarrhea may also be present. In addition to cholestanol accumulation, cerebrotendinous xanthomatosis has been shown to be characterized by abnormal HDLs, which result in impaired cholesterol (and cholestanol) transport and contribute to the consequent xanthomatization.17 The mortality is high, patients usually dying in the fourth to sixth decades, most often from progressive neurological dysfunction, pseudobulbar paralysis or myocardial infarction.22
Tendinous and tuberous xanthomata may also represent a manifestation of β-sitosterolemia. This is an autosomal recessive condition in which increased intestinal absorption of the plant sterols β-sitosterol, campesterol, and stigmasterol results in tissue deposition along with cholesterol and subsequent xanthoma formation.23–25 Normally these sterols are almost completely unabsorbed from the gastrointestinal tract. β-Sitosterolemia is associated with an increased risk of atherosclerosis.4
They may also rarely develop as a manifestation of primary hyperlipoproteinemia (HPL), particularly autosomal recessive lipoprotein lipase deficiency (HPL type I) in children and familial HPL type V in adults.10,11 An exceptional association with β-sitosterolemia, a condition usually presenting with tuberous or tendinous xanthomata, has been documented.12 Much rarer associations include familial hypertriglyceridemia, the nephrotic syndrome, chronic pancreatitis, von Gierke disease, and hypothyroidism.8,13,14 An association with acanthosis nigricans (AN) has also been reported.15 Dystrophic xanthomatization resulting in eruptive xanthomas at the site of prior herpes zoster as a manifestation of Wolf isotopic response has also been reported.16 There are also reports of eruptive xanthomas developing in tattoos.17,18
Xanthomata may occur in extracutaneous locations mimicking tumors in patients with hyperlipidemia. Sites include deep soft tissues and mediastinum.26
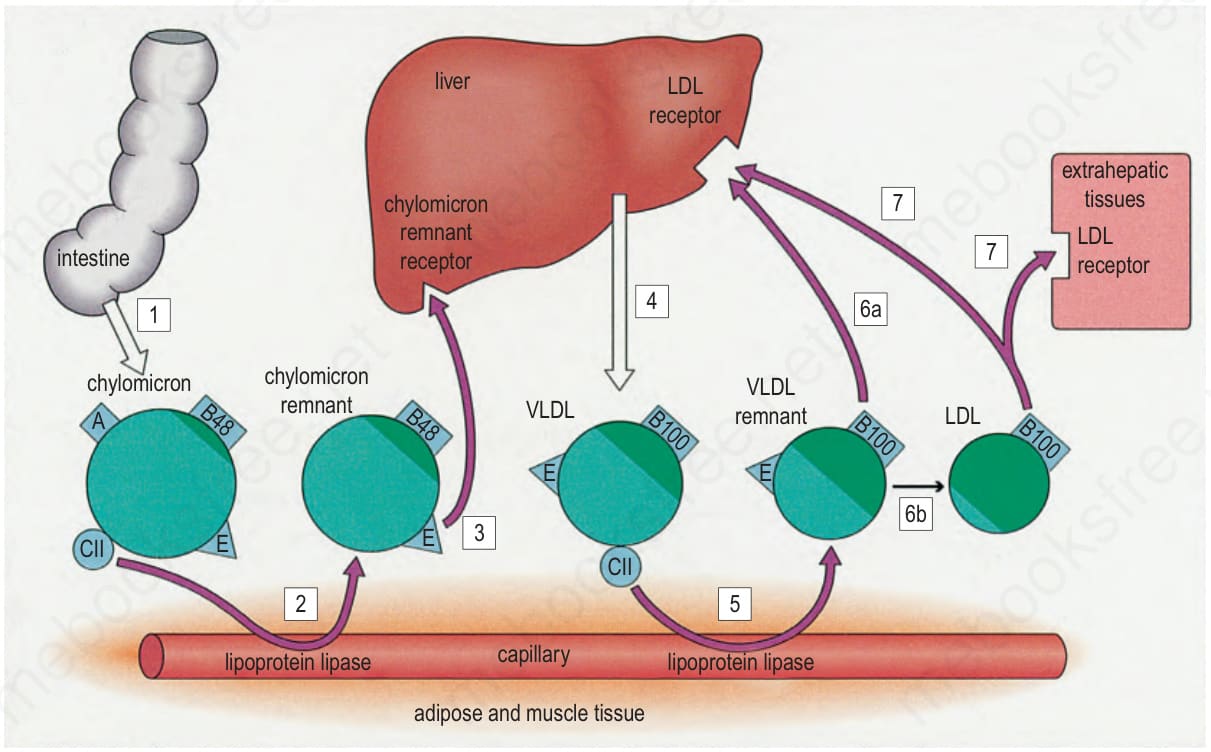
Fig. 13.1 Lipoprotein metabolism. (LDL, low density lipoprotein; VLDL, very low density lipoprotein.) Reproduced with permission from Cruz, P.D., East, C., Bergstresser, P.R. (1988) Journal of the American Academy of Dermatology, 19, 95–111.
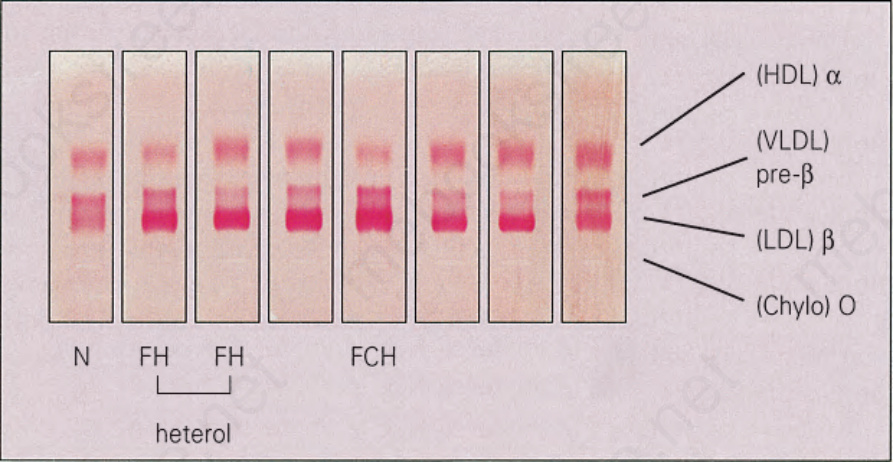
Fig. 13.2 Hyperlipidemia: electrophoretic separation of serum lipids. (Chylo, chylomicron; HDL, high density lipoprotein; LDL, low density lipoprotein; VLDL, very low density lipoprotein.) By courtesy of B. Lewis, MD, St Thomas’ Hospital, London, UK.

Fig. 13.3 Eruptive xanthoma: numerous small yellow papules are present on the buttocks. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
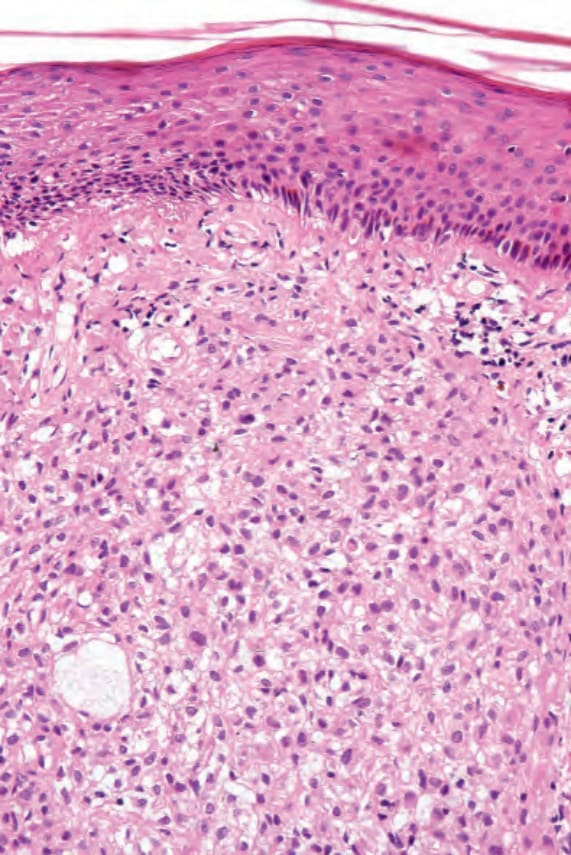
Fig. 13.4 Eruptive xanthoma: biopsy of an established lesion. The histiocytes have abundant vacuolated cytoplasm.
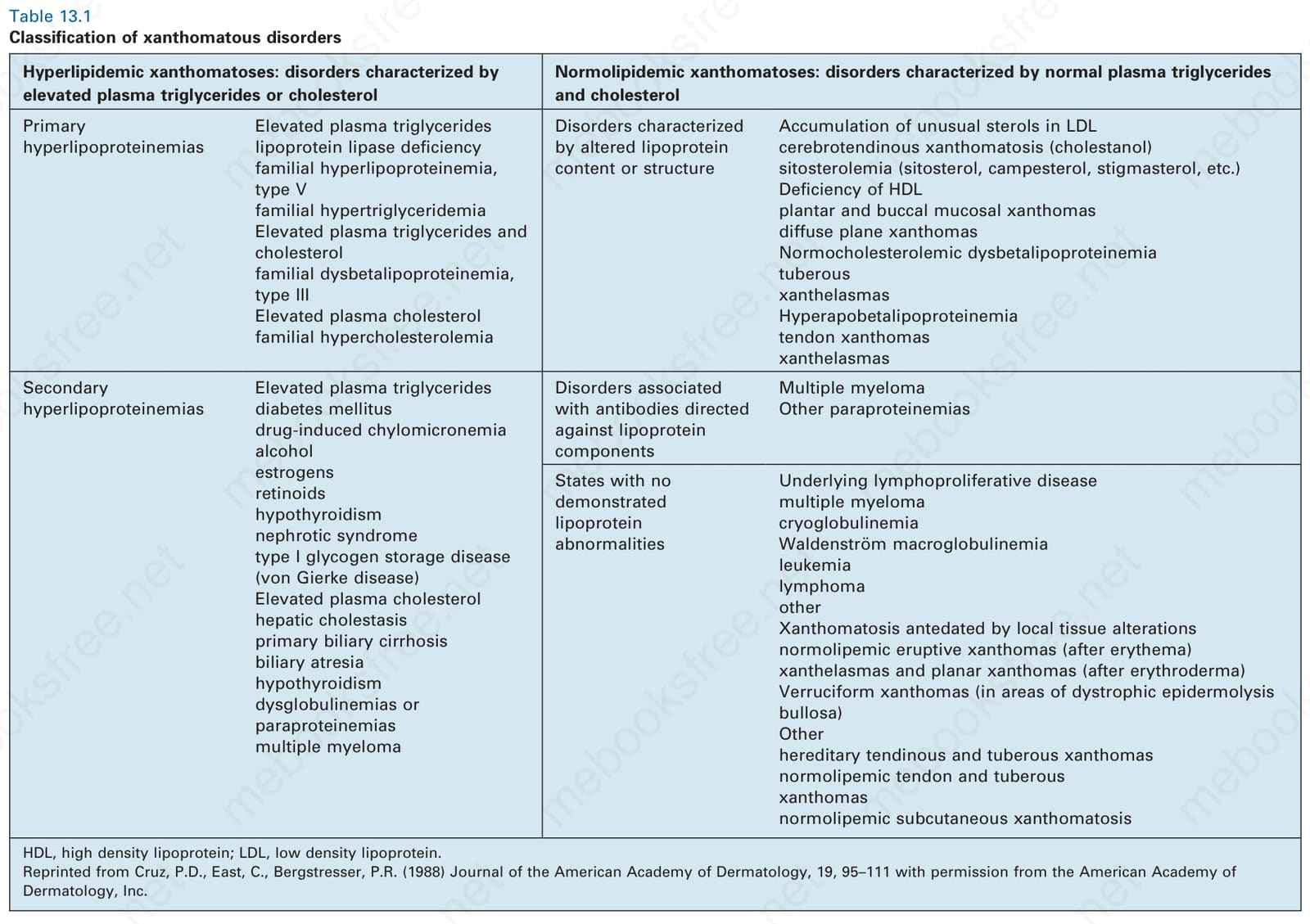
Table 13.1 Classification of xanthomatous disorders
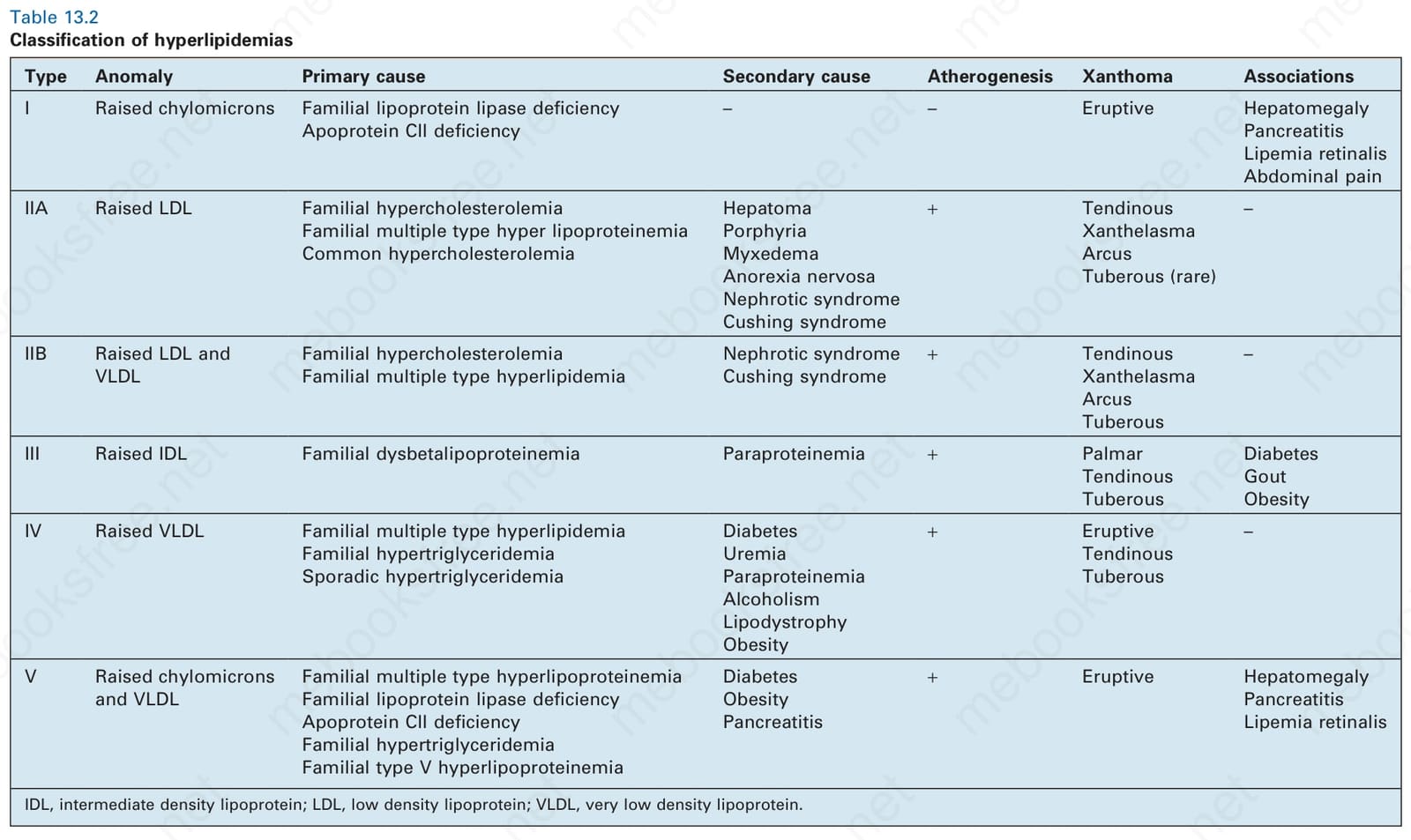
Table 13.2 Classification of hyperlipidemias